Summarise vocal cords paralysis
Reading File
Finding Sources
Finding Sources
Searching PubMed
"vocal cord paralysis" OR "vocal fold paralysis"
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative sources. Let me compile the full summary.
Vocal Cord Paralysis
Definition & Anatomy
Vocal cord paralysis (VCP) is the loss of normal motion of one or both vocal folds due to disruption of the neural supply - either the vagus nerve (CN X), its recurrent laryngeal nerve (RLN) branch, or the superior laryngeal nerve. The RLN's anatomy determines the pattern of disease: the left RLN loops under the aortic arch, while the right RLN rounds beneath the right subclavian artery. This long peripheral course makes both nerves susceptible to compressive or infiltrative lesions anywhere from the skull base to the mediastinum.
- ~75% of cases are unilateral
- ~90% of all paralyses arise from peripheral nerve lesions; only ~10% are central (and these are almost always accompanied by other cranial neuropathies)
Causes
| Category | Examples |
|---|---|
| Neoplasm (36%) | Bronchial, esophageal, thyroid, laryngeal, neck tumors; glomus jugulare |
| Surgical/Iatrogenic (25%) | Thyroid/parathyroid surgery (most common for unilateral VCP), carotid artery surgery, anterior cervical spine surgery, esophageal surgery, cardiac surgery (ligation of PDA) |
| Inflammatory (13%) | Viral/idiopathic neuritis |
| Neurologic - Adults | ALS, MS, Wallenberg syndrome, pseudobulbar palsy, encephalitis, poliomyelitis |
| Neurologic - Children | Arnold-Chiari malformation, hydrocephalus, low tentorium cerebelli, meningomyelocele |
| Trauma | Blunt (clothesline injury, MVA, birth trauma), penetrating (GSW, stab) |
| Idiopathic | Presumed viral; diagnosis of exclusion |
- Textbook of Family Medicine, p. 442
Clinical Features
Unilateral VCP
- Hoarseness / dysphonia - often the dominant complaint; many patients compensate with the opposite cord and maintain a near-normal voice
- Aspiration / cough on swallowing - from glottic incompetence
- Recurrent pneumonia (from chronic aspiration)
- Weak cry (in children)
- Inability to perform a Valsalva maneuver (cannot hold breath against a closed glottis)
- Mild stridor (if cord lies in abducted position)
- The cord lies in a paramedian position on laryngoscopy
Bilateral VCP
- Presents with significant respiratory distress / inspiratory stridor - bilateral medialization of the cords obstructs the glottis
- Voice/cry is often preserved or near-normal (a key contrast to unilateral VCP)
- May require emergency airway establishment (intubation or tracheostomy)
- In children, bilateral VCP is the second most common congenital laryngeal anomaly after laryngomalacia
Diagnosis
- Laryngoscopy (indirect or flexible fibre-optic nasolaryngoscopy) - primary diagnostic tool; shows immobile cord, usually in paramedian position
- CT from skull base to mediastinum/pulmonary hila - evaluates the entire course of the vagus nerve; excellent for neck/chest lesions
- MRI - superior for skull base evaluation
- Laryngeal ultrasound - useful in children unfit for general anaesthesia, and for monitoring
- Videolaryngostroboscopy (VLS) - provides diagnostic and prognostic information
Imaging signs of VCP on CT/MRI:
- Paramedian position of the vocal cord
- Anteromedial displacement of the arytenoid cartilage
- Ipsilateral dilation of the piriform sinus
- Tilting of the thyroid cartilage
- Enlarged/prominent laryngeal ventricle
CT image below - left vocal cord paralysis secondary to squamous cell carcinoma (A: large left upper lobe mass abutting the aortic arch along the course of the left RLN; B: medially displaced left vocal cord, arrow):
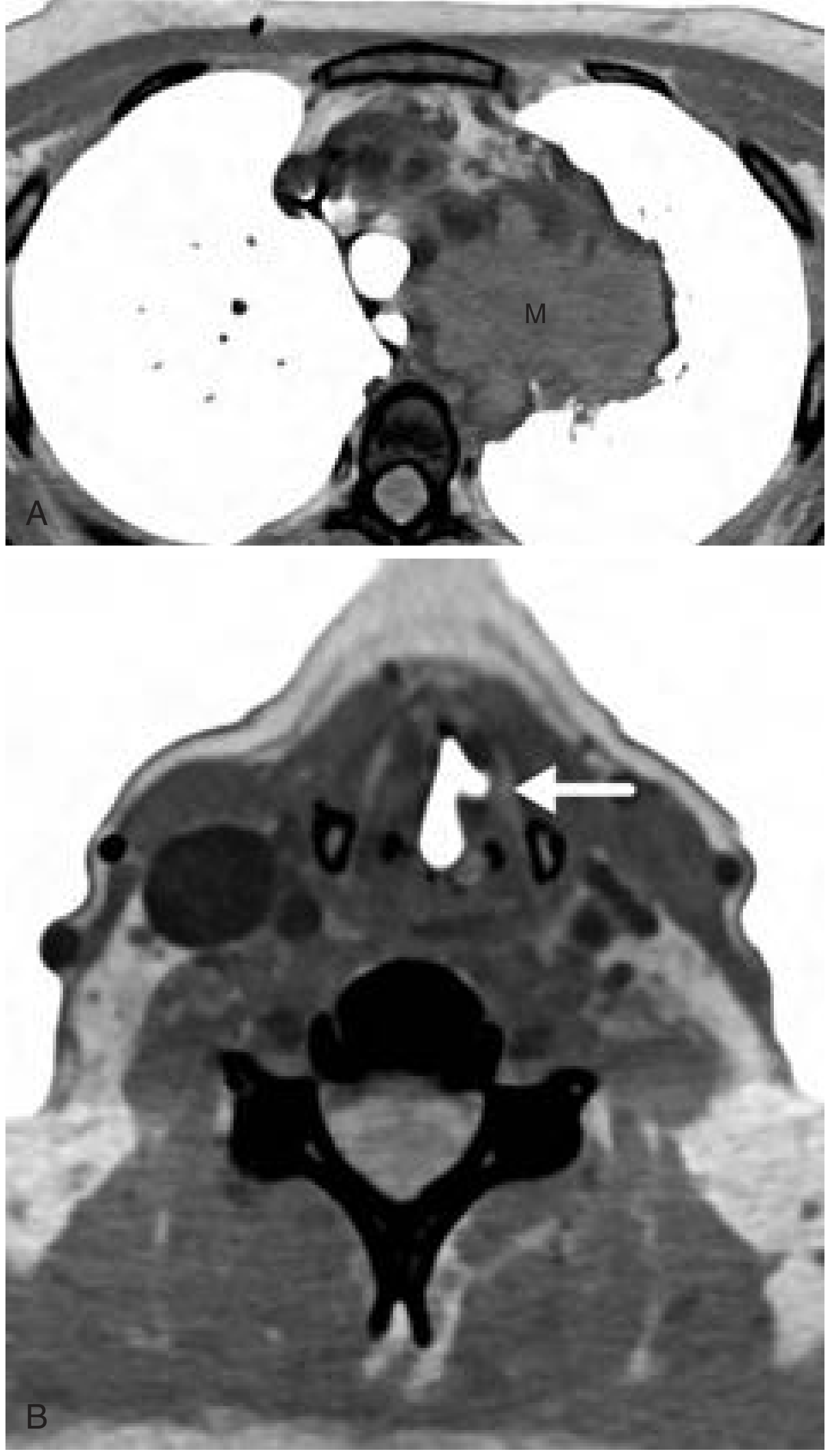
- Cummings Otolaryngology Head and Neck Surgery, p. 1961
Management
Unilateral VCP
- Conservative/observation - if cord is in intermediate position, voice often improves as the contralateral cord compensates or spontaneous recovery occurs
- Voice therapy - to optimise compensation
- Injection laryngoplasty (endoscopic) - autologous fat, collagen, calcium hydroxyapatite, or alloplastic material injected to medialise the paralyzed cord; can provide temporary or permanent improvement. A 2025 systematic review (PMID: 40130411) evaluated techniques under local anaesthesia specifically
- Medialization thyroplasty (Type I) - silastic implant placed via external approach for permanent unilateral paralysis; produces excellent results; silastic restricted to post-pubertal patients in children
- Re-innervation (ansa cervicalis nerve transfer) - restores laryngeal tone; limited success in restoring voluntary movement; most promising in children
Bilateral VCP
- Emergency airway if acute respiratory distress - intubation or tracheostomy (required in ~50% of congenital cases)
- Treat the underlying cause - e.g., VP shunt for hydrocephalus/Arnold-Chiari promptly improves cord movement and may avoid tracheostomy
- Observation - in congenital bilateral VCP, up to 58% recover spontaneously (some after >5 years), so conservative management is strongly favoured
- Surgical enlargement of the glottis (if no recovery and airway remains inadequate):
- Endoscopic laser cordotomy or arytenoidectomy - widens the posterior glottis for breathing while preserving the anterior glottis for voice
- Can be attempted from age 2 in urgent cases; generally deferred to age 11+
- External arytenoidectomy via laryngofissure as a fallback
- Permanent tracheostomy - last resort
Important caveat: An immobile vocal cord is not always paralyzed. In previously intubated patients (especially children), immobility may be due to cricoarytenoid joint fixation or posterior glottic scarring. This distinction is critical - paralysis tends toward spontaneous recovery; fixation/scarring does not - and distinguishing them prevents years of unnecessary waiting before surgical intervention.
Key Points at a Glance
| Feature | Unilateral | Bilateral |
|---|---|---|
| Main symptom | Dysphonia, aspiration | Stridor, airway obstruction |
| Voice | Hoarse (often compensates) | Often preserved/normal |
| Cord position | Paramedian (one side) | Paramedian (both sides) |
| Emergency airway needed | Rarely | Frequently |
| Main treatment | Injection / thyroplasty | Treat cause; laser glottoplasty / trach |
| Congenital recovery rate | Most improve | Up to 58% recover |
Sources:
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol 2, Chapter on Vocal Cord Paralysis
- Cummings Otolaryngology Head and Neck Surgery, p. 1961
- Textbook of Family Medicine 9e, pp. 441-442
This is a shared conversation. Sign in to Orris to start your own chat.