Define Cardiopulmonary bypass its principles Define hypothermia and deep circulatory arrest
Cardiopulmonary Bypass (CPB): Definition and Principles
Definition
"CPB provides distinctly nonphysiological conditions because mean arterial pressure is usually less than normal and blood flow is usually nonpulsatile." - Morgan and Mikhail's Clinical Anesthesiology, 7e, p. 811
Basic Circuit Components
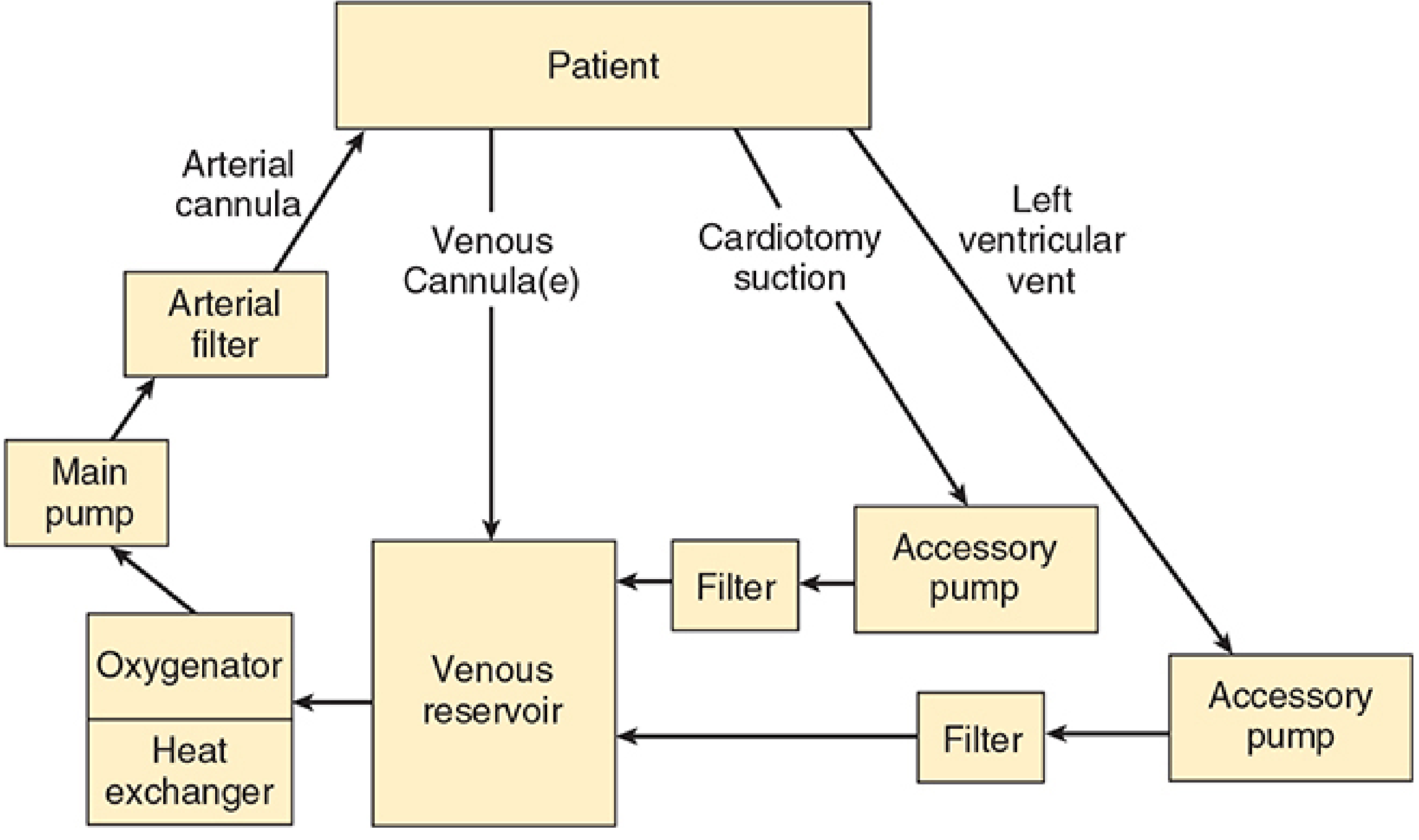
| Component | Function |
|---|---|
| Venous reservoir | Receives deoxygenated blood from the patient via venous cannulae; acts as a buffer for volume |
| Oxygenator | Adds O2 and removes CO2 via a thin, gas-permeable silicone membrane (membrane oxygenator) or by bubbling O2 through blood (bubble oxygenator) |
| Heat exchanger | Controls patient temperature by warming or cooling the perfusate |
| Main pump | Propels blood back into the patient - typically a roller pump (occludes tubing) or centrifugal pump |
| Arterial filter | Fine mesh (20-30 µm) removes emboli (air, particulate matter, debris) before blood returns to the patient |
| Tubing | Conducts blood between components and the patient |
Principles of CPB
1. Cannulation
- The heart and great vessels are exposed via a median sternotomy.
- Venous cannulation: One or two cannulae placed in the right atrium, SVC/IVC, or a femoral vein; blood drains to the reservoir by siphonage (gravity).
- Arterial cannulation: Return cannula placed in the ascending aorta (most common) or femoral artery; oxygenated, pressurized blood is pumped back to the patient.
2. Anticoagulation
- Systemic heparin is given before cannulation to prevent clotting within the circuit.
- After separation from bypass, heparin is reversed with protamine sulphate.
3. Priming the Circuit
- The circuit is primed with 1,200-1,800 mL fluid (adults), typically lactated Ringer's solution, often with added colloid, mannitol, heparin, and bicarbonate.
- In adults, this dilutes the hematocrit to ~22-27%. Blood is added to the prime for neonates, infants, and severely anemic adults.
4. Oxygenation and CO2 Removal
- Membrane oxygenators (current standard): Blood and gas are separated by a thin silicone membrane - no direct blood-gas contact, minimal foaming and protein denaturation.
- Bubble oxygenators (older): Oxygen froth is mixed directly with blood and de-foamed; still available but largely replaced.
- Arterial CO2 tension is controlled by adjusting total gas flow past the oxygenator.
5. Pump Mechanism
- Roller pump: Occludes tubing sequentially to propel a defined volume per revolution; most common.
- Centrifugal pump: Uses a rotating head to create a pressure gradient; does not pump air but output varies with afterload.
- Typical adult flow rates: 50-65 mL/kg/min (normal CO ~5 L/min), maintaining mean arterial pressure of 50-80 mmHg.
6. Heat Exchanger
- Blood passes over a large water bath within the circuit.
- Used both to cool the patient at the start (to reduce metabolic demand) and to rewarm the patient at the end of the procedure.
7. Myocardial Protection
- Aortic cross-clamping excludes the coronary arteries from the bypass flow, creating elective cardiac arrest.
- Cardioplegia (cold or warm chemical solution) is infused via the coronary arteries or coronary sinus to arrest myocardial electrical activity and reduce metabolic demand.
- Topical hypothermia: Ice-slush applied around the heart provides additional protection.
8. Non-physiological Nature of CPB
- Flow is typically non-pulsatile - unlike the normal pulsatile cardiac output.
- Systemic blood pressure is usually lower than normal.
- Inflammatory response is triggered by blood contact with artificial surfaces, activating complement, cytokines, and neutrophils.
Hypothermia During CPB
Definition
Classification by Temperature
| Grade | Temperature | Application |
|---|---|---|
| Mild (tepid) hypothermia | 30°C-35°C | Routine adult cardiac surgery; allows temperature to "drift" down |
| Moderate hypothermia | 25°C-30°C | Most adult cardiac surgery; common default target |
| Deep hypothermia | 15°C-20°C | Complex repairs, aortic arch surgery, pediatric CHD |
| Profound hypothermia | <15°C | Rarely used; maximum metabolic suppression |
- In adults, temperature is rarely lowered below 25°C.
- In pediatric/neonatal patients, deep hypothermia (15-20°C) is commonly used.
Deep Hypothermic Circulatory Arrest (DHCA)
Definition
"For complex repairs, profound hypothermia to temperatures of 15°C to 18°C allows total circulatory arrest for durations of as long as 60 min. During that time, both the heart and the CPB machine are stopped." - Morgan and Mikhail's Clinical Anesthesiology, 7e, p. 816
Scientific Rationale
- Whole-body and cerebral O2 consumption decrease by a factor of 2 to 2.5 for every 10°C reduction in temperature.
- Deep hypothermia reduces metabolic demand so profoundly that organs (especially the brain) can tolerate complete absence of blood flow for a limited period.
- At 18°C, cerebral metabolic rate is reduced to ~15-20% of normal.
Indications
- Complex congenital heart defect repair in neonates and infants (e.g., Norwood stage 1 for hypoplastic left heart syndrome, repair of interrupted aortic arch)
- Aortic arch surgery in adults (e.g., thoracoabdominal aortic aneurysm repair - TAAA)
- Situations where cannulae in the operative field would obstruct the repair
Conduct of DHCA
- Institution of CPB and systemic cooling via the heat exchanger + topical surface cooling.
- When core temperature reaches 18°C: head is packed in ice; a bolus of propofol is given to achieve BIS = 0 (electrocerebral silence).
- Patient is placed in steep Trendelenburg position.
- CPB flow is gradually reduced then stopped entirely - circulatory arrest is established.
- The aorta is cross-clamped; the surgical repair is performed.
- CPB is restarted and rewarming begins; reperfusion of the brain and body is restored.
Organ Protection Adjuncts
- Ice packing around the head - delays cerebral rewarming
- Pharmacological neuroprotection: methylprednisolone 30 mg/kg and mannitol 0.5 g/kg
- Cerebrospinal fluid drainage (CSFD) - maintained open to 10 mmHg to lower spinal cord perfusion pressure
- Neuromonitoring: SSEP and MEP (benefit not proven); EEG
Safe Duration and Neurological Risk
- Short periods (<30-35 min) are generally tolerated well.
- A large study of 549 subjects (Norwood stage 1) found DHCA >45 minutes to be a risk factor for 30-day mortality.
- During reperfusion, cerebral blood flow and metabolism remain transiently depressed in neonates and infants.
- During deep hypothermia, cerebral autoregulation is lost - perfusion becomes entirely dependent on the extracorporeal circuit and post-bypass hemodynamics.
- Effects are not strictly linear; patient-related, procedural, and postoperative factors modify outcomes.
Regional Cerebral Perfusion (RCP) - Alternative to Full DHCA
Summary Table
| Feature | Moderate Hypothermia | Deep Hypothermia (DHCA) |
|---|---|---|
| Temperature | 25-32°C | 15-18°C |
| CPB continued? | Yes | No (complete arrest) |
| Duration tolerated | N/A | Up to ~45-60 min |
| Primary use | Routine cardiac surgery | Complex arch/CHD repair |
| Brain protection | Partial metabolic suppression | Near-complete metabolic suppression |
| Main risk | Coagulopathy, platelet dysfunction | Neurological injury if prolonged |
Make it as university exam answer presentation
ls /home/daytona/workspace/ 2>/dev/null && echo "exists" || mkdir -p /home/dayto…
mkdir -p /home/daytona/workspace/cpb-presentation && echo "created"
Not ppt Just answer
Q. Define Cardiopulmonary Bypass and its Principles. Define Hypothermia and Deep Circulatory Arrest.
CARDIOPULMONARY BYPASS (CPB)
Definition
Principles of CPB
1. Surgical Access and Cannulation
- The heart is exposed via a median sternotomy.
- Venous cannula(e) are placed in the right atrium, SVC/IVC, or a femoral vein. Blood drains passively by siphonage (gravity) into the bypass machine.
- Arterial cannula is placed in the ascending aorta (most common) or femoral artery. Oxygenated blood is pumped back into the systemic circulation from here.
2. Anticoagulation
- Systemic heparin is administered before cannulation to prevent thrombosis within the circuit.
- After bypass is discontinued, heparin is reversed with protamine sulphate.
- Activated clotting time (ACT) is monitored throughout - target ACT >400-480 seconds on bypass.
3. Priming the Circuit
- The circuit is pre-filled (primed) with fluid before use to displace air.
- Adults: 1,200-1,800 mL of balanced salt solution (e.g., lactated Ringer's), often supplemented with colloid, mannitol, heparin, and bicarbonate.
- This causes hemodilution - hematocrit falls to ~22-27% in adults at onset of bypass.
- For neonates, infants, and severely anemic adults, blood is added to the prime to prevent excessive dilution.
4. Components of the CPB Machine
| Component | Function |
|---|---|
| Venous Reservoir | Collects deoxygenated blood from venous cannulae; acts as volume buffer |
| Oxygenator | Adds O2 and removes CO2 via a thin gas-permeable silicone membrane (membrane oxygenator) |
| Heat Exchanger | Controls patient temperature - cools at start, rewarming at end |
| Main Pump | Propels blood back to patient (roller pump or centrifugal pump) |
| Arterial Filter | Fine mesh filter (20-30 µm) removes air bubbles, particulate emboli, debris |
| Tubing | Connects all components and the patient |
- Roller pump - occludes flexible tubing sequentially; delivers a precise defined volume per revolution; most widely used.
- Centrifugal pump - rotating magnetic head creates a pressure gradient; does not pump air; output varies with afterload (preload-sensitive).
- Membrane oxygenator (current standard) - blood and gas separated by a thin silicone membrane; no direct blood-gas contact; minimal protein denaturation and foaming.
- Bubble oxygenator (older, largely replaced) - oxygen is bubbled directly through blood; requires de-foaming chambers.
5. Conduct of Bypass
- At the start of bypass, the aorta is cross-clamped, which excludes the coronary arteries from circulation.
- Cardioplegia solution (cold or warm, crystalloid or blood) is infused antegrade via the aortic root or retrograde via the coronary sinus to arrest myocardial electrical activity and reduce myocardial oxygen demand.
- Topical hypothermia (ice-slush around the heart) provides additional myocardial protection.
- The CPB machine now takes over entirely - providing artificial circulation and ventilation.
6. Pump Flow and Pressure
- Adult flow rates: 50-65 mL/kg/min (approximating normal cardiac output ~5 L/min).
- Mean arterial pressure maintained at 50-80 mmHg in adults.
- Flow is typically non-pulsatile (unlike normal cardiac output) - a non-physiological state.
- Pediatric patients require higher flow rates (up to 200 mL/kg/min) and tolerate lower pressures (20-50 mmHg).
7. Non-physiological Effects of CPB
- Non-pulsatile flow, hemodilution, hypothermia
- Systemic inflammatory response - blood contact with artificial surfaces activates complement, cytokines, and neutrophils
- Altered pharmacokinetics of drugs (changes in protein binding, volume of distribution, clearance)
- Coagulopathy, platelet dysfunction
- Risk of air/particulate microembolism
8. Weaning from CPB
- The heart is de-aired, cross-clamp released, cardiac rhythm restored (spontaneous or with defibrillation).
- Rewarming via heat exchanger to normothermia.
- Ventilation is re-established.
- CPB flow is gradually reduced as the heart takes over.
- Heparin is reversed with protamine sulphate.
- Cannulae are removed and cannulation sites repaired.
HYPOTHERMIA
Definition
Physiological Basis
- Metabolic oxygen requirement is approximately halved for every 10°C reduction in body temperature (Q10 effect; described by the Arrhenius equation: k = Ae⁻RT).
- At deep hypothermic temperatures, cerebral metabolic rate falls to ~15-20% of normal baseline.
- This allows organs to tolerate periods of reduced or zero blood flow that would otherwise cause irreversible ischemic damage.
Classification by Temperature
| Grade | Temperature | Clinical Use |
|---|---|---|
| Mild / Tepid | 30°C - 35°C | Routine adult cardiac surgery; temperature allowed to "drift" |
| Moderate | 25°C - 30°C | Standard for most adult cardiac procedures |
| Deep | 15°C - 20°C | Complex pediatric CHD repair, aortic arch surgery |
| Profound | < 15°C | Rarely used; maximum metabolic suppression |
- In adults, temperature is rarely lowered below 25°C.
- In neonates and infants undergoing complex CHD surgery, 15-20°C is common.
Adverse Effects of Hypothermia
- Platelet dysfunction and coagulopathy
- Depression of myocardial contractility
- Altered drug pharmacokinetics (e.g., reduced esterase activity - remifentanil clearance decreases ~20% per degree below 37°C)
- Impaired autoregulation at very low temperatures
- Metabolic acidosis on rewarming
DEEP HYPOTHERMIC CIRCULATORY ARREST (DHCA)
Definition
"For complex repairs, profound hypothermia to temperatures of 15°C to 18°C allows total circulatory arrest for durations of as long as 60 min. During that time, both the heart and the CPB machine are stopped." (Morgan & Mikhail's Clinical Anesthesiology, 7e)
Indications
- Complex congenital heart defect repair in neonates and infants (e.g., Norwood stage 1 for hypoplastic left heart, interrupted aortic arch repair)
- Aortic arch surgery in adults (e.g., thoracoabdominal aortic aneurysm - TAAA repair)
- Any procedure where cannulae or blood in the operative field would obstruct precise surgical repair
Scientific Rationale
- At 18°C, whole-body O2 consumption decreases by a factor of 2 to 2.5 for every 10°C of temperature reduction.
- The brain, the organ most sensitive to ischemia, is protected by near-complete suppression of cerebral metabolic rate.
- This provides a "metabolic window" during which the circulation can safely be arrested.
Conduct of DHCA (Step-by-Step)
- Institution of CPB - venous and arterial cannulation established.
- Active systemic cooling via the heat exchanger combined with topical surface cooling; head packed in ice.
- Target temperature reached: 15°C-18°C (core temperature monitored by nasopharyngeal/bladder/rectal probes).
- Pharmacological brain protection administered:
- Propofol bolus to achieve EEG silence (BIS = 0)
- Methylprednisolone 30 mg/kg
- Mannitol 0.5 g/kg
- Patient placed in steep Trendelenburg position (empties cerebral venous sinuses).
- CPB pump flow reduced then stopped - circulatory arrest established.
- Surgical repair performed in a completely bloodless, cannula-free field.
- CPB flow restarted - reperfusion and rewarming begins via heat exchanger.
Safe Duration and Neurological Risk
- The brain is the most vulnerable organ during DHCA - most sensitive and least tolerant of ischemia and reperfusion injury.
- Brainstem and cortical evoked potentials are altered after DHCA and are related to arrest duration.
- During reperfusion, cerebral blood flow and metabolism remain transiently depressed in neonates.
- At deep hypothermic temperatures, cerebral autoregulation is lost - perfusion becomes entirely dependent on the extracorporeal circuit.
- A large study of 549 patients (Norwood stage 1) found DHCA >45 minutes to be a significant risk factor for 30-day mortality.
- The effect of DHCA is not linear - short durations (<30-35 min) are generally well tolerated; adverse neurological outcomes increase markedly beyond 45-60 min.
Adjuncts to Reduce Neurological Risk
| Adjunct | Mechanism |
|---|---|
| Ice packing around the head | Delays cerebral rewarming; promotes brain cooling |
| Propofol / thiopentone | Achieves EEG silence; reduces baseline cerebral metabolic rate |
| Methylprednisolone | Reduces inflammatory and reperfusion injury |
| Mannitol | Osmotic diuresis; reduces cerebral edema |
| Cerebrospinal fluid drainage (CSFD) | Reduces spinal cord perfusion pressure (target ≤10 mmHg) |
| pH-stat CO2 management | Better brain cooling in pediatric patients during DHCA |
Regional Cerebral Perfusion (RCP) - Alternative Strategy
SUMMARY TABLE
| Feature | Moderate Hypothermia | DHCA |
|---|---|---|
| Temperature | 25-32°C | 15-18°C |
| Pump continued? | Yes | No - complete arrest |
| Safe duration | Continuous | Up to ~45-60 min |
| Primary use | Routine adult cardiac surgery | Aortic arch, complex CHD repair |
| Brain protection | Partial metabolic suppression | Near-complete metabolic suppression |
| Main risk | Coagulopathy, platelet dysfunction | Neurological injury if prolonged |
Deep circulation arrest
Q. Write a Short Note / Define and Describe Deep Hypothermic Circulatory Arrest (DHCA)
Definition
"DHCA involves reducing the patient's core temperature to profoundly hypothermic levels (15–22°C) before globally interrupting blood flow to the body, draining all the blood out of the patient, and collecting it in the ECC reservoir."
- Miller's Anesthesia, 10e
Physiological Basis / Rationale
- Metabolic oxygen requirement is reduced by 50% for every 7-10°C fall in body temperature.
- At 18°C, cerebral metabolic rate for oxygen (CMRO2) is only 15-19% of normal.
- At 8°C, cerebral oxygen requirement falls to approximately 11% of baseline.
- Hypothermia reduces both the electrophysiologic energy consumption and the energy needed for basic cellular integrity and homeostasis - a reduction that no drug (including barbiturates) can achieve alone.
- This provides a limited but critical "metabolic window" during which ischemia from complete circulatory arrest can be tolerated without irreversible organ damage.
"Hypothermia is the principal cerebral protective technique for circulatory arrest procedures. It unequivocally enhances cerebral tolerance for episodes of ischemia." - Miller's Anesthesia, 10e
Indications
| Category | Examples |
|---|---|
| Adult aortic surgery | Aortic arch aneurysm repair, Type A aortic dissection, thoracoabdominal aortic aneurysm (TAAA) |
| Pediatric congenital heart surgery | Norwood stage 1 for hypoplastic left heart, interrupted aortic arch repair, transposition with complex anomalies |
| Any procedure requiring a bloodless, cannula-free field | When blood or cannulae in the field would compromise precise surgical reconstruction |
Conduct of DHCA - Step by Step
Step 1: Institution of CPB
- Standard venous and arterial cannulation.
- Full heparinization (ACT >400 sec).
- CPB initiated and systemic cooling begins via the heat exchanger.
Step 2: Cooling Phase
- Temperature lowered by the CPB heat exchanger and surface cooling (ice packs to the head and body).
- Target temperature: 15°C-18°C (monitored at nasopharynx, bladder, rectum, and tympanic membrane - multiple sites used to confirm uniform brain cooling).
- For an average adult, cold arterial perfusion at full flow should continue for 20-30 minutes after reaching the target arterial blood temperature to allow adequate time for brain parenchymal equilibration (a time lag exists between arterial blood cooling and brain tissue cooling).
- As temperature falls, blood viscosity increases (at 18°C with Hct 30-35%, viscosity rises 3-4 times normal) - hemodilution to Hct ~18-20% is used to minimize microcirculatory disturbance.
Step 3: Blood Gas Management During Cooling
- Adults: α-stat management (temperature-uncorrected PaCO2 ~40 mmHg).
- Pediatric patients: pH-stat management (temperature-corrected; higher CO2 promotes cerebral vasodilation and better brain cooling).
Step 4: Pre-Arrest Pharmacological Neuroprotection
| Agent | Dose | Purpose |
|---|---|---|
| Propofol (or thiopentone) | Bolus to achieve BIS = 0 | EEG isoelectricity - confirm electrical silence before arrest |
| Methylprednisolone | 30 mg/kg | Reduce inflammatory/reperfusion injury |
| Mannitol | 0.5 g/kg | Osmotic cerebral edema prevention; promotes diuresis |
Step 5: Circulatory Arrest
- Patient placed in steep Trendelenburg position (empties cerebral venous sinuses, provides additional cerebral protection).
- CPB pump flow is gradually reduced then stopped entirely.
- Patient's blood is drained into the ECC reservoir and recirculated within the circuit at the target temperature to prevent stasis.
- Gas flow to the oxygenator is stopped.
- Surgical repair is performed - completely bloodless field, no cannulae obstructing the view.
Step 6: Reperfusion and Rewarming
- CPB pump flow is slowly restarted - reperfusion commences gradually.
- Rewarming via the heat exchanger - gradual rewarming is essential; rapid rewarming causes cerebral hyperthermia which dramatically worsens ischemic injury.
- Cardiac rhythm is restored (spontaneous or electrical cardioversion).
- Ventilation is re-established.
- Heparin reversed with protamine; cannulae removed.
Safe Duration and the "Time Limit"
| Duration of Arrest | Expected Outcome |
|---|---|
| < 30-35 min | Generally well tolerated; neurological outcomes usually normal |
| 30-45 min | Increasing risk; outcomes inconsistent |
| > 45 min | Significant risk factor for mortality and neurological injury |
| > 60 min | High risk of severe, permanent neurological damage |
- A large study of 549 patients undergoing Norwood stage 1 procedure found DHCA > 45 minutes to be a significant risk factor for 30-day mortality.
- The effect is not linear - there is a threshold phenomenon, not a simple dose-response relationship.
- Outcomes are modified by patient age, diagnosis, pH management strategy, and postoperative care.
Cerebral Monitoring During DHCA
| Monitor | Purpose |
|---|---|
| EEG / BIS | Confirm electrical silence (isoelectricity) before arrest; BIS target = 0 |
| SSEP / MEP | Somatosensory and motor evoked potentials - altered duration-dependently after arrest |
| Multi-site temperature probes | Nasopharyngeal, tympanic, bladder, rectal - confirms brain cooling |
| NIRS (cerebral oximetry) | Monitors cerebral oxygen saturation during arrest and reperfusion |
Complications of DHCA
Neurological (Most Feared)
- Stroke - from air embolism, particulate emboli, incomplete cerebral cooling
- Neurocognitive dysfunction - subtle memory and attention deficits; common even with short arrest times
- Seizures - post-arrest cortical hyperexcitability
- Choreoathetosis - basal ganglia injury; more common in children after prolonged arrest
- Cerebral edema - reperfusion injury
Systemic
- Coagulopathy - platelet dysfunction, dilutional factor deficiency worsened by deep hypothermia
- Myocardial depression - hypothermia suppresses contractility; inotropes required on rewarming
- Systemic inflammatory response - blood-circuit interaction, ischemia-reperfusion
- Acute kidney injury - ischemia during arrest period
- Metabolic acidosis - lactic acidosis on reperfusion
Alternatives to Full Circulatory Arrest
| Technique | Description |
|---|---|
| Selective Antegrade Cerebral Perfusion (ACP) | Perfusion of brain via axillary artery or direct carotid cannulation; most widely used; many centers now use moderate hypothermia (22-24°C) with ACP instead of deep hypothermia |
| Retrograde Cerebral Perfusion (RCP) | Cold oxygenated blood perfused retrogradely via SVC; mainly flushes debris and maintains cooling; limited nutritive flow |
"Because ACP provides excellent brain protection, many surgeons now use more moderate levels of hypothermia (often between 22°C and 24°C) to decrease the risks associated with deep hypothermia." - Schwartz's Principles of Surgery, 11e
Key Points for Exam
- DHCA = core temperature 15-22°C + complete cessation of CPB pump flow + exsanguination into circuit reservoir.
- Rationale: metabolic O2 requirement halved for every 7-10°C fall in temperature; at 18°C, CMRO2 is ~15-19% of normal.
- EEG isoelectricity must be confirmed by hypothermia (not drugs alone) before arrest begins.
- Cooling time lag: allow 20-30 min of cold perfusion after target arterial temperature to ensure brain equilibration.
- Safe arrest time: generally <30-35 min; risk increases sharply beyond 45-60 min.
- Brain is the most sensitive and least tolerant organ during DHCA.
- Adults: α-stat CO2 management; Pediatric: pH-stat (better brain cooling).
- Main neurological risks: stroke, choreoathetosis (children), neurocognitive decline.
- Alternatives: ACP (preferred modern adjunct) allows moderate rather than profound hypothermia.
- Rewarming must be gradual - rapid rewarming causes cerebral hyperthermia and worsens injury.
Like diagram
Line diagram
Clean black and white medical line diagram of Deep Hypothermic Circulatory Arrest (DHCA) showing the step-by-step process as a vertical flowchart with labeled boxes and arrows. Steps shown: 1) Institution of CPB (venous and arterial cannulation), 2) Systemic Cooling via heat exchanger (target 15-18°C), 3) Pharmacological Neuroprotection (propofol BIS=0, methylprednisolone, mannitol), 4) EEG Isoelectricity confirmed, 5) Steep Trendelenburg position, 6) CPB Pump Stopped - Circulatory Arrest - blood drained to reservoir, 7) Surgical Repair (bloodless cannula-free field), 8) CPB Restarted - Reperfusion, 9) Gradual Rewarming + Ventilation restored. Include a side panel showing temperature scale with labels: Mild 30-35°C, Moderate 25-30°C, Deep 15-20°C with arrow pointing to DHCA range. Include safe arrest time note: less than 30-35 min safe, greater than 45 min high risk. White background, bold black lines, neat medical textbook illustration style, no color
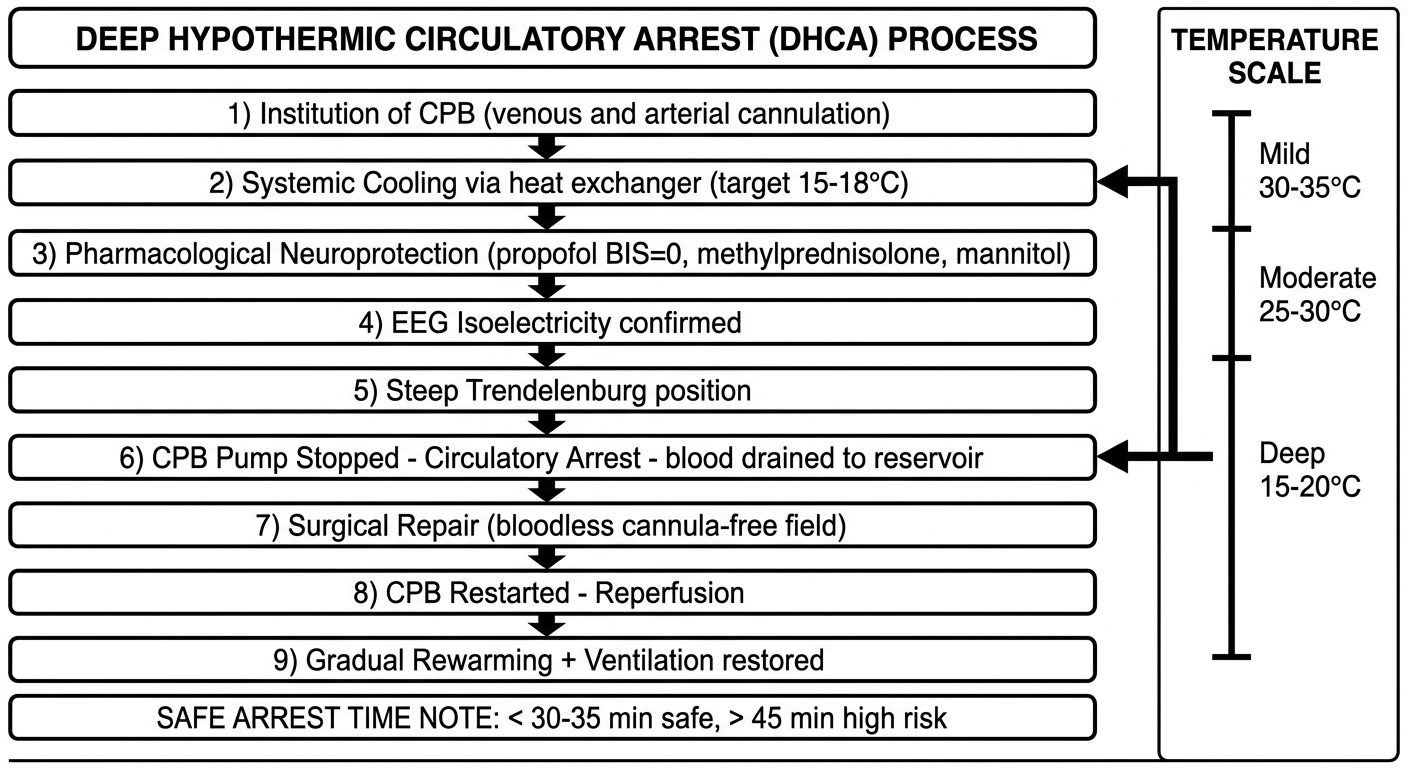
- Left column: Sequential steps from CPB institution → cooling → arrest → repair → rewarming
- Right panel: Temperature classification scale showing where DHCA sits (15-18°C = deep hypothermia)
- Bottom note: Safe arrest time limits (<30-35 min safe; >45 min high risk)
Complications of cpb
Q. Write a Note on Complications of Cardiopulmonary Bypass (CPB)
Introduction
"CPB is a complex technique requiring careful interaction and communication between surgeon, anaesthetist and perfusionist to ensure patient safety. Difficulties can occur during cannulation, at the start of CPB and at the end of CPB." - Bailey & Love's Surgery, 28e
Classification of Complications
COMPLICATIONS OF CPB
│
├── TECHNICAL / MECHANICAL
├── HAEMATOLOGICAL
├── CARDIOVASCULAR
├── NEUROLOGICAL
├── PULMONARY
├── RENAL
├── GASTROINTESTINAL
└── SYSTEMIC INFLAMMATORY RESPONSE
1. Technical / Mechanical Complications
| Phase | Complication |
|---|---|
| Cannulation | Aortic dissection (arterial cannula misplaced), atrial wall injury, venous cannula malposition, femoral vessel injury |
| On bypass | Oxygenator failure, pump failure, circuit disconnection, tubing rupture, low reservoir level (air pumped to patient) |
| Anticoagulation failure | Inadequate heparin - thrombosis within circuit; clot formation in oxygenator |
| Protamine reaction | Anaphylaxis, pulmonary hypertension, systemic hypotension on reversal |
- Occurs if the venous reservoir empties and the roller pump propels air into the arterial cannula
- Presents as sudden loss of EEG activity, cardiovascular collapse
- Managed by immediate cessation of CPB, Trendelenburg position, aspiration of air
2. Haematological Complications
a) Coagulopathy (Most Common Haematological Complication)
- Dilutional coagulopathy - circuit priming solution dilutes clotting factors and platelets; hematocrit falls to 22-27%
- Platelet dysfunction - contact with artificial surfaces activates then depletes platelets; hypothermia further suppresses platelet function
- Fibrinolysis - CPB activates plasminogen, causing fibrin degradation
- Heparin rebound - residual heparin effect after protamine reversal, causing delayed bleeding
- Protamine-heparin complex - platelet aggregation and complement activation
b) Haemolysis
- Roller pump trauma, suction catheters, and oxygenator cause red cell destruction
- Results in haemoglobinaemia, haemoglobinuria, and risk of renal tubular injury
c) Thrombocytopaenia
- Platelet consumption at artificial surfaces and sequestration in the circuit
3. Cardiovascular Complications
a) Myocardial Stunning
- Transient, reversible systolic and diastolic dysfunction following ischaemia-reperfusion
- Manifests as low cardiac output after weaning from bypass
- Responds to positive inotropic support; recovers with time
b) Myocardial Infarction
- Incomplete myocardial protection, coronary embolism, or graft failure
- Risk increases with aortic cross-clamp time >120 minutes
c) Low Cardiac Output Syndrome
- Post-bypass ventricular dysfunction
- Managed with inotropes (dopamine, dobutamine, epinephrine), IABP, or mechanical circulatory support
d) Arrhythmias
- Atrial fibrillation - most common (30-50% post-cardiac surgery)
- Ventricular arrhythmias - related to myocardial ischaemia or reperfusion
- Heart block - surgical trauma to conduction system
e) Cardiac Tamponade
- Post-bypass haemorrhage into pericardial space
- Presents with rising CVP, falling BP, muffled heart sounds (Beck's triad)
4. Neurological Complications
a) Stroke (Type I Neurological Injury)
- Incidence: ~1-5% in adults undergoing CABG; higher in valvular surgery
- Causes:
- Macroembolism - atheromatous debris from aortic manipulation
- Air embolism - inadequate de-airing of cardiac chambers
- Particulate embolism - calcified debris, thrombus, fat
- Hypoperfusion during low-flow states
- Presents as focal neurological deficit on recovery from anaesthesia
b) Neurocognitive Dysfunction (Type II Neurological Injury)
- More common than overt stroke
- Short-term - confusion, memory impairment, attention deficits in first weeks
- Long-term - subtle cognitive decline persisting months to years (controversial)
- Attributed to microemboli, inflammatory mediators, and cerebral hypoperfusion
c) Cerebral Hyperthermia
- Rapid rewarming on CPB causes brain temperature to overshoot 37°C
- Even 1°C rise above normal dramatically worsens ischaemic injury
- Post-operative temperatures >38.5°C occur in ~40% of patients and correlate with cognitive dysfunction 6 weeks post-operatively
- Prevention: slow, gradual rewarming; no monitored temperature should exceed 37°C
d) Choreoathetosis (in children)
- Basal ganglia injury after prolonged DHCA
- Involuntary, purposeless movements appearing 1-2 days post-operatively
5. Pulmonary Complications
a) Post-Pump Lung / Pump Lung
- Diffuse alveolar damage from complement activation, neutrophil sequestration in lung, and ischaemia-reperfusion
- Manifests as hypoxaemia, increased A-a gradient, bilateral infiltrates on CXR
- In severe form: ARDS (acute respiratory distress syndrome)
b) Atelectasis
- Most common pulmonary complication
- Due to deflation of the lungs during bypass, compression by retractors, diaphragmatic dysfunction
- Treated with physiotherapy, CPAP, incentive spirometry
c) Pleural Effusion
- Left-sided pleural effusion common after CABG (internal mammary artery harvest disturbs pleural integrity)
d) Pulmonary Hypertension
- Especially in patients with pre-existing mitral valve disease
- Exacerbated by protamine administration
6. Renal Complications
a) Acute Kidney Injury (AKI)
- Incidence: ~5-30% (degree of severity varies)
- Causes:
- Non-pulsatile flow causing reduced renal perfusion
- Microembolism to renal vasculature
- Haemoglobinuria from haemolysis (renal tubular toxicity)
- Reduced cardiac output post-bypass
- Nephrotoxic drugs (contrast, aminoglycosides)
- Severe AKI requiring dialysis occurs in ~1-5%
b) Prevention
- Maintain adequate perfusion pressure (MAP 50-80 mmHg on CPB)
- Mannitol in pump prime promotes diuresis
- Avoid nephrotoxins perioperatively
7. Gastrointestinal Complications
- Less common but carry high mortality when they occur
- Causes: splanchnic hypoperfusion from non-pulsatile low-flow states, microembolism, mesenteric vasoconstriction
| Complication | Features |
|---|---|
| Mesenteric ischaemia | Abdominal pain, ileus, lactic acidosis - mortality up to 70% |
| Acute pancreatitis | Elevated amylase/lipase, abdominal pain |
| GI bleeding | Stress ulceration, coagulopathy |
| Bowel infarction | Most lethal GI complication |
| Hepatic dysfunction | Jaundice, elevated LFTs from hepatic hypoperfusion |
8. Systemic Inflammatory Response Syndrome (SIRS)
Mechanism
Blood + Artificial Surface
↓
Complement activation (C3a, C5a)
↓
Neutrophil activation → cytokine release (TNF-α, IL-1, IL-6, IL-8)
↓
Endothelial injury → capillary leak
↓
SIRS → Multiorgan dysfunction / failure
- Hypothermia, ischaemia-reperfusion, surgical trauma, and endotoxaemia all compound this response.
- Manifestations: fever, hypotension, capillary leak, oedema, multiorgan failure in severe cases.
Minimizing SIRS
- Mini-CPB circuits (smaller surface area - reduced inflammatory activation)
- Off-pump CABG (beating heart surgery) - avoids CPB entirely; limited to CABG
- Leucocyte depletion filters
- Heparin-coated circuits
- Corticosteroids (dexamethasone) - modest benefit in reducing AF; no mortality benefit in large RCTs
Summary Table
| System | Key Complication |
|---|---|
| Technical | Aortic dissection, air embolism, oxygenator failure |
| Haematological | Coagulopathy, haemolysis, thrombocytopaenia |
| Cardiovascular | Myocardial stunning, low CO, AF, tamponade |
| Neurological | Stroke, cognitive dysfunction, cerebral hyperthermia |
| Pulmonary | Pump lung, atelectasis, ARDS |
| Renal | AKI, renal failure |
| GI | Mesenteric ischaemia, pancreatitis |
| Systemic | SIRS, multiorgan failure |
Myocardial preservation techniques during cardiopulmonary bypass.
Q. Describe Myocardial Preservation Techniques During Cardiopulmonary Bypass
Introduction
"Myocardial protection of the heart from ischaemic damage during CPB is achieved via: institution of hypothermia, induction of cardioplegia to facilitate arrest, and decompression of the LV; the goal is to minimize myocardial metabolic function." - Barash's Clinical Anesthesia, 9e
Pathophysiology of Myocardial Ischaemia During CPB
Coronary flow ceases
↓
Aerobic ATP production stops
Anaerobic metabolism begins → lactic acidosis
↓
High-energy phosphates (ATP, creatine phosphate) rapidly depleted
↓
Intracellular Ca²⁺ overload
Na⁺/K⁺-ATPase pump failure → cellular oedema
↓
On reperfusion: oxygen free radicals generated
→ Ischaemia-reperfusion injury
↓
Myocardial stunning (reversible) or Necrosis (irreversible)
- Poor preoperative LV function
- Ventricular hypertrophy
- Diffuse severe coronary artery disease
- Prolonged aortic cross-clamp time (>120 minutes increases risk significantly)
Techniques of Myocardial Preservation
TECHNIQUE 1: AORTIC CROSS-CLAMPING
- A still, bloodless, motionless operative field
- A closed system into which cardioplegia can be delivered under controlled pressure
TECHNIQUE 2: CARDIOPLEGIA
Definition
Mechanism of Cardiac Arrest
- Potassium (20-30 mEq/L induction dose) depolarises the cardiac myocyte membrane
- Membrane potential is maintained at a depolarised level → no action potential generation → electromechanical silence
- Potassium-induced arrest alone reduces myocardial oxygen consumption (MVO₂) by 90%
- Combined with hypothermia (temperature <22°C): MVO₂ reduced by 97%
Composition of Cardioplegia Solutions
| Component | Role | Typical Concentration |
|---|---|---|
| Potassium (arrest agent) | Depolarises membrane → diastolic arrest | Induction: 20-30 mEq/L; Maintenance: 10 mEq/L |
| Sodium (reduced) | Limits ischaemia-induced intracellular Na⁺ accumulation | <140 mEq/L |
| Calcium (low) | Maintains cellular integrity without triggering contracture | 0.7-1.2 mmol/L |
| Magnesium | Blocks excessive intracellular Ca²⁺ influx | 1.5-15 mmol/L |
| Buffer (bicarbonate/THAM/histidine) | Prevents acid metabolite accumulation; alkalotic pH improves preservation | pH ~7.4-7.8 |
| Osmotic agents (mannitol) | Reduces cellular oedema; free radical scavenger | Added as needed |
| Energy substrates | Replenish depleted ATP stores | Glucose, glutamate, aspartate |
| Membrane stabilisers | Reduce electrical irritability | Lidocaine, procaine, glucocorticoids |
Types of Cardioplegia - By Composition
| Type | Description | Advantage | Disadvantage |
|---|---|---|---|
| Crystalloid cardioplegia | Potassium in electrolyte solution (e.g., St Thomas', HTK) | Simple, cheap, single-dose possible | No O₂ carrying capacity |
| Blood cardioplegia (most common in North America) | Blood mixed with crystalloid (ratio 4:1 or 8:1) | Carries O₂; provides energy substrates; more physiological | More complex preparation |
| del Nido solution | 1:4 blood:crystalloid + lidocaine, MgSO₄, NaHCO₃, mannitol, KCl | Single-dose for short cross-clamp; good protection for 60-90 min | Less flexible for very long cases |
| HTK (Histidine-Tryptophan-Ketoglutarate) | Crystalloid; single large volume dose | Safe arrest up to 90 minutes without redosing | Large volume; no O₂; expensive |
Types of Cardioplegia - By Temperature
| Temperature | Degree | Effect | Use |
|---|---|---|---|
| Cold (4-10°C) | Hypothermic | Further reduces metabolism; powerful protection | Most common; intermittent delivery |
| Warm/Normothermic (37°C) | Normothermic | Better enzyme activation; superior metabolic recovery post-arrest | Must be delivered continuously (cannot work in a dry field) |
| Tepid (28-32°C) | Between cold and warm | Compromise; reasonable protection + some metabolic benefits | Increasingly used |
"Warm cardioplegic solutions may facilitate better myocardial recovery postoperatively by aiding activation of intramyocardial enzymes." - Bailey & Love's Surgery, 28e
Route of Cardioplegia Delivery
A. Antegrade Cardioplegia (Standard)
- Delivered proximal to the aortic cross-clamp, into the aortic root at 60-100 mmHg
- Flows forward through coronary ostia → into coronary arteries → myocardium
- Most physiological route
- Limitation: fails to reach myocardium distal to high-grade coronary obstructions; unreliable if aortic regurgitation present (cardioplegia leaks back through valve into LV rather than entering coronaries)
B. Retrograde Cardioplegia
- Balloon-tipped catheter placed into the coronary sinus via the right atrium
- Cardioplegia delivered at 200-400 mL/min to a venous back-pressure of 30-50 mmHg
- Flows retrograde through coronary veins → capillaries → myocardium
- Advantages: more uniform distribution in diffuse CAD; independent of aortic valve competence; continuous delivery possible
- Limitation: poor perfusion of RV free wall and posterior 1/3 of interventricular septum (RCA territory); less nutritive flow to microvasculature
C. Combined Antegrade + Retrograde (Optimal)
- Most complete myocardial protection
- Antegrade delivers to coronary artery territory; retrograde supplements areas not reached antegrade
- Especially useful in severe multi-vessel CAD and repeat cardiac surgery
D. Direct Coronary Ostial Delivery
- In aortic valve surgery with AI, direct cannulation of individual coronary ostia
- Ensures cardioplegia reaches coronaries despite incompetent valve
Frequency of Dosing
| Solution | Redosing Interval | Safe Arrest Time |
|---|---|---|
| Standard cold blood/crystalloid | Every 20-30 minutes | 20-30 min per dose |
| del Nido | Single dose | 60-90 min |
| HTK | Single large dose | Up to 90 min |
| Warm blood | Continuous infusion | Continuous |
TECHNIQUE 3: SYSTEMIC HYPOTHERMIA
- CPB heat exchanger reduces core body temperature to 25-32°C in routine surgery
- For each 1°C reduction below 37°C, cellular metabolism decreases by approximately 8%
- At 28°C, metabolic rate falls to 50% of normal
- Reduces myocardial O₂ consumption independent of cardioplegia
TECHNIQUE 4: TOPICAL MYOCARDIAL COOLING (ICE-SLUSH)
- Cold saline or ice-slush solution bathed around the heart in the pericardial well
- Provides direct surface cooling of the myocardium
- Maintains myocardial temperature at 10-15°C (measured directly by a thermistor probe in the ventricular wall)
- Combats rewarming from adjacent warm structures (descending aorta, ambient air in theatre)
- Simple, effective adjunct to cardioplegia
TECHNIQUE 5: LEFT VENTRICULAR VENTING
- LV distension during CPB is actively harmful - increases wall tension, raises MVO₂, and causes subendocardial ischaemia
- An LV vent catheter (placed via pulmonary vein or aortic root) decompresses the cavity
- Monitored intraoperatively with transoesophageal echocardiography (TEE)
- Especially important in patients with aortic insufficiency (antegrade cardioplegia may regurgitate into LV, preventing coronary delivery and causing distension)
TECHNIQUE 6: REPERFUSION MANAGEMENT ("HOT SHOT")
- Oxygen free radical generation
- Rapid intracellular calcium overload
- Neutrophil-endothelial activation
- Cellular oedema
| Strategy | Mechanism |
|---|---|
| "Hot shot" - warm blood cardioplegia given just before unclamping | Washes out metabolic byproducts; replenishes energy substrates before O₂ is restored |
| Reduce perfusion pressure at moment of reperfusion | Prevents hyperaemic injury to stunned myocardium (altered coronary autoregulation) |
| Avoid hypercalcaemia during reperfusion | Prevents Ca²⁺-mediated contracture |
| Mannitol in perfusate | Free radical scavenging |
| Gradual rewarming | Prevents rapid metabolic demand outstripping substrate delivery |
TECHNIQUE 7: INTERMITTENT CROSS-CLAMP FIBRILLATION (ICCF)
- An alternative to cardioplegia, used mainly for short coronary bypass procedures
- A small electrical charge is applied to induce ventricular fibrillation (VF)
- The heart does not eject, is relatively still, but not completely bloodless
- The aorta is intermittently clamped to create short periods of ischaemia (10-20 minutes)
- Cross-clamp is periodically released, allowing the heart to reperfuse and recover
- Simple technique; avoids cardioplegia-related complications
- Limitation: not suitable for valvular or complex intra-cardiac repairs requiring a bloodless field
TECHNIQUE 8: TOTAL CIRCULATORY ARREST (DHCA)
- For cases where even a still heart is insufficient - requires a completely bloodless, cannula-free field
- CPB used to cool to 15-18°C then pump stopped entirely
- See separate note on DHCA for full details
Summary: Hierarchy of Myocardial Preservation
PRIMARY PROTECTION
━━━━━━━━━━━━━━━━━━
① Aortic cross-clamp → stops coronary flow
② Cardioplegia (K⁺) → arrests electromechanical activity (-90% MVO₂)
③ Hypothermia (systemic + topical) → reduces basal metabolism (-97% MVO₂ combined)
ADJUNCTS
━━━━━━━━
④ LV venting → prevents distension/subendocardial ischaemia
⑤ Optimal delivery route (antegrade ± retrograde)
⑥ Redosing at 20-30 min intervals
REPERFUSION PROTECTION
━━━━━━━━━━━━━━━━━━━━━
⑦ Hot shot before unclamping
⑧ Controlled reperfusion pressure
⑨ Free radical scavengers (mannitol)
Key Points for Exam
- Aortic cross-clamping is the foundation - creates a bloodless, still field.
- Potassium-induced arrest reduces MVO₂ by 90%; combined with hypothermia (<22°C) reduces it by 97%.
- Cardioplegia must be redosed every 20-30 minutes (standard); del Nido gives 60-90 min single-dose protection.
- Cold blood cardioplegia is the most common choice in current practice.
- Antegrade = physiological but fails beyond coronary obstructions; retrograde = uniform in diffuse CAD but misses RV free wall.
- Topical ice-slush maintains myocardial temperature at 10-15°C.
- LV venting is mandatory to prevent distension-induced injury, especially in AI.
- "Hot shot" (warm blood cardioplegia before reperfusion) limits ischaemia-reperfusion injury.
- CPB times >120 minutes increase myocardial injury risk regardless of preservation technique.
- Inadequate preservation manifests post-bypass as: low cardiac output, arrhythmias, worsened LV function on TEE.