Create a ppt, topic Dermatology of Dermatology RICHARD P. USATINE and JENNIFER KREJCI-MANWARING CHAPTER OUTLINE Principles of Diagnosis, 740 General Management, 741 Skin Problems Beginning in Childhood, 742 Inflammatory Dermatologic Diseases, 747 Infectious Skin Diseases, 756 Infestations, 767 Hypersensitivity Reactions and Other Eruptions, 769 Skin Signs of Systemic Disease, 771 Benign Growths, 773 Premalignant and Malignant Skin Lesions, 775
ls /home/daytona/workspace/ 2>/dev/null || mkdir -p /home/daytona/workspace/derm…
mkdir -p /home/daytona/workspace/dermatology-ppt && ls /home/daytona/workspace/d…
~/dermatology-ppt/build.js
const pptxgen = require("pptxgenjs");
const pres = new pptxgen();
pres.layout = "LAYOUT_16x9";
pres.author = "Richard P. Usatine & Jennifer Krejci-Manwaring";
pres.title = "Dermatology";
// ── Color Palette ──────────────────────────────────────────────────
const C = {
skin: "F5EDE3", // warm cream background
deep: "1A2C42", // deep navy (dominant dark)
teal: "1F7A8C", // teal accent
rust: "C0392B", // rust red accent
amber: "E67E22", // amber highlight
white: "FFFFFF",
lightGray:"F0F4F8",
midGray: "8899AA",
gold: "D4A843",
};
// ── Helpers ────────────────────────────────────────────────────────
function darkSlide(slide) {
slide.background = { color: C.deep };
}
function skinSlide(slide) {
slide.background = { color: C.skin };
}
function lightSlide(slide) {
slide.background = { color: C.lightGray };
}
function addAccentBar(slide, color, y = 0, h = 0.08) {
slide.addShape(pres.ShapeType.rect, { x: 0, y, w: "100%", h, fill: { color } });
}
function sectionHeader(slide, sectionNum, title, subtitle, bgColor, accentColor) {
slide.background = { color: bgColor };
// Top accent stripe
slide.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: "100%", h: 0.12, fill: { color: accentColor } });
// Bottom accent stripe
slide.addShape(pres.ShapeType.rect, { x: 0, y: 5.5, w: "100%", h: 0.125, fill: { color: accentColor } });
// Large section number watermark
slide.addText(sectionNum, {
x: 7.5, y: 0.5, w: 2.5, h: 4.5,
fontSize: 140, color: accentColor, bold: true, align: "right",
transparency: 75, fontFace: "Georgia",
});
slide.addText(title, {
x: 0.5, y: 1.4, w: 7, h: 1.8,
fontSize: 38, bold: true, color: C.deep, fontFace: "Calibri", align: "left",
});
if (subtitle) {
slide.addText(subtitle, {
x: 0.5, y: 3.3, w: 7, h: 0.7,
fontSize: 16, color: C.teal, fontFace: "Calibri", align: "left", italic: true,
});
}
}
function contentSlide(slide, title, bullets, accentColor) {
lightSlide(slide);
// Left colored sidebar
slide.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 0.18, h: "100%", fill: { color: accentColor } });
// Top bar
slide.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: "100%", h: 0.1, fill: { color: accentColor } });
slide.addText(title, {
x: 0.35, y: 0.18, w: 9.4, h: 0.65,
fontSize: 22, bold: true, color: C.deep, fontFace: "Calibri", align: "left",
});
// Divider
slide.addShape(pres.ShapeType.line, { x: 0.35, y: 0.88, w: 9.3, h: 0, line: { color: accentColor, width: 1.5 } });
const items = bullets.map((b, i) => {
if (b.startsWith("__")) {
return { text: b.replace(/^__/, ""), options: { bold: true, color: accentColor, fontSize: 13, bullet: false, breakLine: true, indentLevel: 0 } };
}
return { text: b, options: { bullet: { type: "bullet" }, breakLine: true, fontSize: 12.5, color: "2C3E50", indentLevel: b.startsWith(" ") ? 1 : 0 } };
});
slide.addText(items, {
x: 0.45, y: 1.0, w: 9.2, h: 4.35,
fontFace: "Calibri", valign: "top", lineSpacingMultiple: 1.15,
});
}
function twoColSlide(slide, title, leftItems, rightItems, accentColor) {
lightSlide(slide);
slide.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: "100%", h: 0.1, fill: { color: accentColor } });
slide.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 0.18, h: "100%", fill: { color: accentColor } });
slide.addText(title, {
x: 0.35, y: 0.18, w: 9.4, h: 0.65,
fontSize: 22, bold: true, color: C.deep, fontFace: "Calibri",
});
slide.addShape(pres.ShapeType.line, { x: 0.35, y: 0.88, w: 9.3, h: 0, line: { color: accentColor, width: 1.5 } });
// Col divider
slide.addShape(pres.ShapeType.line, { x: 5.1, y: 1.0, w: 0, h: 4.2, line: { color: accentColor, width: 0.8, dashType: "dash" } });
const makeItems = (arr) => arr.map(b => ({
text: b, options: { bullet: { type: "bullet" }, breakLine: true, fontSize: 12, color: "2C3E50", indentLevel: b.startsWith(" ") ? 1 : 0 }
}));
slide.addText(makeItems(leftItems), { x: 0.45, y: 1.0, w: 4.5, h: 4.3, fontFace: "Calibri", valign: "top", lineSpacingMultiple: 1.2 });
slide.addText(makeItems(rightItems), { x: 5.25, y: 1.0, w: 4.5, h: 4.3, fontFace: "Calibri", valign: "top", lineSpacingMultiple: 1.2 });
}
function tableSlide(slide, title, headers, rows, accentColor) {
lightSlide(slide);
slide.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: "100%", h: 0.1, fill: { color: accentColor } });
slide.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 0.18, h: "100%", fill: { color: accentColor } });
slide.addText(title, {
x: 0.35, y: 0.18, w: 9.4, h: 0.65,
fontSize: 22, bold: true, color: C.deep, fontFace: "Calibri",
});
slide.addShape(pres.ShapeType.line, { x: 0.35, y: 0.88, w: 9.3, h: 0, line: { color: accentColor, width: 1.5 } });
const tableData = [
headers.map(h => ({ text: h, options: { bold: true, color: C.white, fill: accentColor, fontSize: 12, align: "center" } })),
...rows.map((row, ri) => row.map(cell => ({ text: cell, options: { fontSize: 11, fill: ri % 2 === 0 ? "FFFFFF" : "EEF4FA", color: "2C3E50", align: "left" } })))
];
slide.addTable(tableData, { x: 0.35, y: 1.0, w: 9.3, colW: Array(headers.length).fill(9.3 / headers.length), border: { pt: 0.5, color: "CCDDEE" }, autoPage: false });
}
// ══════════════════════════════════════════════════════════════════
// SLIDE 1 – TITLE
// ══════════════════════════════════════════════════════════════════
let s = pres.addSlide();
darkSlide(s);
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 0.3, h: "100%", fill: { color: C.teal } });
s.addShape(pres.ShapeType.rect, { x: 0, y: 4.9, w: "100%", h: 0.725, fill: { color: C.teal }, transparency: 40 });
// Large decorative circle
s.addShape(pres.ShapeType.ellipse, { x: 6.8, y: -1.0, w: 5.5, h: 5.5, fill: { color: C.teal }, line: { color: C.teal }, transparency: 85 });
s.addShape(pres.ShapeType.ellipse, { x: 7.5, y: 2.8, w: 3.5, h: 3.5, fill: { color: C.gold }, line: { color: C.gold }, transparency: 80 });
s.addText("DERMATOLOGY", {
x: 0.5, y: 0.9, w: 9, h: 1.4,
fontSize: 58, bold: true, color: C.white, fontFace: "Calibri", charSpacing: 8,
});
s.addText("Principles of Diagnosis · Management · Clinical Conditions", {
x: 0.5, y: 2.35, w: 8.5, h: 0.6,
fontSize: 16, color: C.gold, fontFace: "Calibri", italic: true, charSpacing: 1,
});
s.addShape(pres.ShapeType.line, { x: 0.5, y: 3.1, w: 5.5, h: 0, line: { color: C.teal, width: 2 } });
s.addText("Richard P. Usatine, MD · Jennifer Krejci-Manwaring, MD", {
x: 0.5, y: 3.3, w: 8.5, h: 0.45,
fontSize: 14, color: C.midGray, fontFace: "Calibri",
});
s.addText("Family Medicine | Dermatology | Chapter 33", {
x: 0.5, y: 3.75, w: 8.5, h: 0.4,
fontSize: 13, color: C.gold, fontFace: "Calibri",
});
s.addText("Source: Textbook of Family Medicine • 2026", {
x: 0.5, y: 5.0, w: 9, h: 0.35,
fontSize: 11, color: C.white, fontFace: "Calibri", transparency: 30,
});
// ══════════════════════════════════════════════════════════════════
// SLIDE 2 – CHAPTER OUTLINE
// ══════════════════════════════════════════════════════════════════
s = pres.addSlide();
darkSlide(s);
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: "100%", h: 0.12, fill: { color: C.teal } });
s.addShape(pres.ShapeType.rect, { x: 0, y: 5.5, w: "100%", h: 0.125, fill: { color: C.gold } });
s.addText("CHAPTER OUTLINE", {
x: 0.5, y: 0.2, w: 9, h: 0.65,
fontSize: 28, bold: true, color: C.white, fontFace: "Calibri", charSpacing: 4,
});
const sections = [
["01", "Principles of Diagnosis", "p. 740"],
["02", "General Management", "p. 741"],
["03", "Skin Problems Beginning in Childhood", "p. 742"],
["04", "Inflammatory Dermatologic Diseases", "p. 747"],
["05", "Infectious Skin Diseases", "p. 756"],
["06", "Infestations", "p. 767"],
["07", "Hypersensitivity Reactions & Other Eruptions", "p. 769"],
["08", "Skin Signs of Systemic Disease", "p. 771"],
["09", "Benign Growths", "p. 773"],
["10", "Premalignant & Malignant Skin Lesions", "p. 775"],
];
sections.forEach((sec, i) => {
const col = i < 5 ? 0 : 1;
const row = i < 5 ? i : i - 5;
const xBase = col === 0 ? 0.4 : 5.2;
const yBase = 1.05 + row * 0.87;
s.addShape(pres.ShapeType.rect, { x: xBase, y: yBase, w: 4.5, h: 0.72, fill: { color: "1E3A54" }, line: { color: C.teal, width: 0.5 } });
s.addText(sec[0], { x: xBase + 0.08, y: yBase + 0.08, w: 0.55, h: 0.55, fontSize: 15, bold: true, color: C.teal, fontFace: "Georgia", align: "center" });
s.addShape(pres.ShapeType.line, { x: xBase + 0.65, y: yBase + 0.1, w: 0, h: 0.52, line: { color: C.teal, width: 0.7 } });
s.addText(sec[1], { x: xBase + 0.75, y: yBase + 0.1, w: 3.0, h: 0.52, fontSize: 12.5, color: C.white, fontFace: "Calibri", valign: "middle" });
s.addText(sec[2], { x: xBase + 3.75, y: yBase + 0.1, w: 0.65, h: 0.52, fontSize: 10, color: C.gold, fontFace: "Calibri", align: "right", valign: "middle" });
});
// ══════════════════════════════════════════════════════════════════
// SLIDE 3 – SECTION 1 HEADER: Principles of Diagnosis
// ══════════════════════════════════════════════════════════════════
s = pres.addSlide();
sectionHeader(s, "01", "Principles of Diagnosis", "Systematic approach to skin lesion identification", C.skin, C.teal);
// ══════════════════════════════════════════════════════════════════
// SLIDE 4 – Morphology & Lesion Types
// ══════════════════════════════════════════════════════════════════
s = pres.addSlide();
twoColSlide(s, "Primary & Secondary Skin Lesions",
[
"PRIMARY LESIONS",
" Macule – flat, color change <1 cm",
" Patch – flat, color change >1 cm",
" Papule – raised, solid <1 cm",
" Plaque – raised, solid >1 cm",
" Nodule – raised, solid, deeper",
" Vesicle – fluid-filled blister <0.5 cm",
" Bulla – large blister >0.5 cm",
" Pustule – pus-filled lesion",
" Wheal – transient edematous papule",
],
[
"SECONDARY LESIONS",
" Scale – flaking of stratum corneum",
" Crust – dried serum/exudate",
" Erosion – superficial epithelial loss",
" Ulcer – full-thickness skin loss",
" Fissure – linear crack in skin",
" Scar – fibrous replacement tissue",
" Lichenification – thickened skin",
" Excoriation – scratch-induced erosion",
],
C.teal
);
// ══════════════════════════════════════════════════════════════════
// SLIDE 5 – Distribution & Morphology Tips
// ══════════════════════════════════════════════════════════════════
s = pres.addSlide();
contentSlide(s, "Diagnostic Approach: Key Principles", [
"1. DESCRIBE THE LESION MORPHOLOGY FIRST",
" Identify: primary lesion type, size, shape, color, border, surface",
" Avoid premature diagnosis — describe before naming",
"2. ASSESS DISTRIBUTION",
" Localized vs. generalized; sun-exposed vs. protected areas",
" Dermatomal (herpes zoster) vs. scattered (varicella)",
" Symmetrical (contact dermatitis) vs. random",
"3. CONSIDER ASSOCIATED FEATURES",
" Pruritus, pain, systemic symptoms, fever",
" Onset, duration, triggers (drugs, foods, sun, stress)",
"4. FITZPATRICK SKIN TYPE MATTERS",
" Type I–II: highest risk for skin cancer (UV damage)",
" Type V–VI: keloid tendency; post-inflammatory hyperpigmentation common",
"5. USE DERMOSCOPY WHEN AVAILABLE",
" Improves diagnostic accuracy for pigmented lesions by 10–27%",
], C.teal);
// ══════════════════════════════════════════════════════════════════
// SLIDE 6 – Fitzpatrick Scale Table
// ══════════════════════════════════════════════════════════════════
s = pres.addSlide();
tableSlide(s, "Fitzpatrick Skin Type Classification",
["Type", "Complexion", "Sun Response", "Skin Cancer Risk"],
[
["I", "Very white", "Always burns, never tans", "Highest"],
["II", "White", "Burns easily, tans minimally", "Very High"],
["III", "White to olive", "Sometimes burns, slowly tans", "High"],
["IV", "Brown", "Burns minimally, always tans", "Moderate"],
["V", "Dark brown", "Rarely burns, tans well", "Low"],
["VI", "Black", "Never burns, deeply pigmented", "Lowest"],
],
C.teal
);
// ══════════════════════════════════════════════════════════════════
// SLIDE 7 – SECTION 2 HEADER: General Management
// ══════════════════════════════════════════════════════════════════
s = pres.addSlide();
sectionHeader(s, "02", "General Management", "Treatment principles in dermatologic disease", C.skin, C.rust);
// ══════════════════════════════════════════════════════════════════
// SLIDE 8 – General Management Content
// ══════════════════════════════════════════════════════════════════
s = pres.addSlide();
contentSlide(s, "General Management Principles", [
"TOPICAL THERAPY",
" Choose vehicle based on location & condition: ointments (dry/scaly), creams (moist), gels (oily/hairy areas)",
" Low-potency steroids: face, intertriginous areas, children",
" High-potency steroids: thick plaques on trunk/extremities",
" Avoid fluorinated steroids on face — risk of atrophy, telangiectasia",
"PROCEDURAL APPROACHES",
" Cryotherapy: benign lesions, warts, actinic keratoses",
" Curettage & electrodesiccation: seborrheic keratoses, BCCs",
" Mohs micrographic surgery: highest cure rate for NMSC",
"SYSTEMIC THERAPY",
" Antibiotics, antivirals, antifungals as indicated",
" Immunosuppressants (methotrexate, cyclosporine) for severe inflammatory disease",
" Biologics (dupilumab, TNF-α inhibitors): targeted therapy for psoriasis, atopic dermatitis",
"PHOTOPROTECTION",
" SPF ≥30 broad-spectrum sunscreen; UVA + UVB protection",
], C.rust);
// ══════════════════════════════════════════════════════════════════
// SLIDE 9 – SECTION 3 HEADER: Skin Problems in Childhood
// ══════════════════════════════════════════════════════════════════
s = pres.addSlide();
sectionHeader(s, "03", "Skin Problems Beginning in Childhood", "Atopic dermatitis, acne, and pediatric dermatoses", C.skin, C.amber);
// ══════════════════════════════════════════════════════════════════
// SLIDE 10 – Atopic Dermatitis
// ══════════════════════════════════════════════════════════════════
s = pres.addSlide();
contentSlide(s, "Atopic Dermatitis (Eczema)", [
"EPIDEMIOLOGY",
" Most common chronic skin disease in children; affects 10–20% of children, 1–3% adults",
" Atopic triad: eczema + asthma + allergic rhinitis",
"PATHOPHYSIOLOGY",
" Filaggrin gene mutations → impaired skin barrier → IgE sensitization",
" Th2-skewed immune response; elevated IgE levels",
"CLINICAL FEATURES",
" Infants: red weeping patches on cheeks, scalp, extensor surfaces",
" Children/adults: flexural lichenified plaques (antecubital, popliteal fossae)",
" Key feature: intense pruritus — 'the itch that rashes'",
"MANAGEMENT",
" Emollients: cornerstone of therapy; apply immediately after bathing",
" Topical corticosteroids: first-line for flares",
" Topical calcineurin inhibitors (tacrolimus, pimecrolimus): steroid-sparing",
" Dupilumab (IL-4/IL-13 inhibitor): for moderate-to-severe disease ≥6 months",
], C.amber);
// ══════════════════════════════════════════════════════════════════
// SLIDE 11 – Acne Vulgaris
// ══════════════════════════════════════════════════════════════════
s = pres.addSlide();
twoColSlide(s, "Acne Vulgaris",
[
"PATHOGENESIS",
" 1. Follicular hyperkeratinization",
" 2. Excess sebum production (androgens)",
" 3. C. acnes colonization",
" 4. Inflammatory cascade",
"LESION TYPES",
" Non-inflammatory: open comedones (blackheads), closed comedones (whiteheads)",
" Inflammatory: papules, pustules, nodules, cysts",
"GRADING",
" Mild, moderate, severe / nodulocystic",
],
[
"TREATMENT LADDER",
" Mild: topical retinoids ± topical antibiotics (BPO combination)",
" Moderate: oral antibiotics (doxycycline, minocycline) + topical retinoid",
" Severe: oral isotretinoin (0.5–1 mg/kg/day x 5–6 months)",
"SPECIAL NOTES",
" Isotretinoin: iPLEDGE program required (teratogenic)",
" Combination BPO + antibiotic reduces resistance",
" Hormonal therapy (OCP, spironolactone) for women",
" Avoid excessive washing — worsens dryness",
],
C.amber
);
// ══════════════════════════════════════════════════════════════════
// SLIDE 12 – Other Childhood Dermatoses
// ══════════════════════════════════════════════════════════════════
s = pres.addSlide();
contentSlide(s, "Other Pediatric Skin Conditions", [
"SEBORRHEIC DERMATITIS",
" 'Cradle cap' in infants; greasy, yellow scales on scalp, eyebrows, nasolabial folds",
" Caused by Malassezia yeast; responds to antifungal shampoos (ketoconazole 2%)",
"DIAPER DERMATITIS",
" Irritant contact dermatitis; spares skin folds (vs. candidal — involves folds)",
" Treatment: barrier ointments (zinc oxide), frequent changes, antifungals if candidal",
"IMPETIGO",
" S. aureus or S. pyogenes; 'honey-colored' crusts — most common bacterial skin infection in children",
" Topical mupirocin (localized); oral cephalexin or amoxicillin-clavulanate (widespread)",
"MOLLUSCUM CONTAGIOSUM",
" Poxvirus; pearly dome-shaped papules with central umbilication",
" Often self-limiting; curettage or cantharidin for troublesome lesions",
"WARTS (VERRUCA VULGARIS)",
" HPV (types 1, 2, 4); rough hyperkeratotic papules; plantar warts (verruca plantaris)",
" Cryotherapy, salicylic acid; immunocompetent patients usually self-resolve",
], C.amber);
// ══════════════════════════════════════════════════════════════════
// SLIDE 13 – SECTION 4 HEADER: Inflammatory Dermatologic Diseases
// ══════════════════════════════════════════════════════════════════
s = pres.addSlide();
sectionHeader(s, "04", "Inflammatory Dermatologic Diseases", "Psoriasis, rosacea, and other inflammatory conditions", C.skin, C.teal);
// ══════════════════════════════════════════════════════════════════
// SLIDE 14 – Psoriasis
// ══════════════════════════════════════════════════════════════════
s = pres.addSlide();
contentSlide(s, "Psoriasis", [
"EPIDEMIOLOGY & PATHOPHYSIOLOGY",
" Affects 2–3% of the population; T-cell mediated (Th17 pathway); IL-17, IL-23 key cytokines",
" Genetic (HLA-Cw6); triggers: stress, infection, medications (lithium, β-blockers, NSAIDs)",
"CLINICAL VARIANTS",
" Plaque psoriasis (80%): well-demarcated, salmon-red plaques with silvery scale; extensor surfaces, scalp",
" Guttate: teardrop papules; post-streptococcal; common in children",
" Pustular: sterile pustules; can be life-threatening (von Zumbusch)",
" Erythrodermic: >90% BSA; medical emergency",
" Nail psoriasis: pitting, onycholysis, oil-drop sign, subungual hyperkeratosis",
" Psoriatic arthritis: 5–30%; asymmetric oligoarthritis; dactylitis; enthesitis",
"AUSPITZ SIGN & KOEBNER PHENOMENON",
" Auspitz: pinpoint bleeding on scale removal; Koebner: lesions at sites of trauma",
"TREATMENT",
" Mild: topical steroids + vitamin D analogues (calcipotriene)",
" Moderate-severe: phototherapy (nbUVB), methotrexate, biologics (TNF-α, IL-17, IL-23 inhibitors)",
], C.teal);
// ══════════════════════════════════════════════════════════════════
// SLIDE 15 – Rosacea & Other Inflammatory
// ══════════════════════════════════════════════════════════════════
s = pres.addSlide();
twoColSlide(s, "Rosacea & Lichen Planus",
[
"ROSACEA",
" Chronic facial condition; central face",
" Triggers: heat, spicy foods, alcohol, UV",
" Subtypes:",
" 1. Erythematotelangiectatic: flushing, erythema",
" 2. Papulopustular: acne-like (no comedones)",
" 3. Phymatous: rhinophyma (thickened nose)",
" 4. Ocular: blepharitis, keratitis",
" Treatment:",
" Topical: metronidazole, azelaic acid, ivermectin",
" Systemic: doxycycline 40 mg modified-release",
" Rhinophyma: laser or surgical debulking",
],
[
"LICHEN PLANUS",
" 6 P's: Pruritic, Purple, Polygonal, Planar, Papules, Plaques",
" Wickham's striae: lacy white network on surface",
" Sites: wrists, ankles, oral mucosa, genitalia",
" Oral LP: may be premalignant",
" Pathology: band-like lymphocytic infiltrate at dermal-epidermal junction",
" Treatment: potent topical steroids; systemic steroids for severe/widespread disease",
"",
"CONTACT DERMATITIS",
" Irritant (80%): soaps, detergents — no prior sensitization needed",
" Allergic (20%): Type IV hypersensitivity; patch testing for diagnosis",
" Common allergens: nickel, latex, poison ivy (urushiol)",
],
C.teal
);
// ══════════════════════════════════════════════════════════════════
// SLIDE 16 – SECTION 5 HEADER: Infectious Skin Diseases
// ══════════════════════════════════════════════════════════════════
s = pres.addSlide();
sectionHeader(s, "05", "Infectious Skin Diseases", "Bacterial, fungal, and viral dermatoses", C.skin, C.rust);
// ══════════════════════════════════════════════════════════════════
// SLIDE 17 – Bacterial Skin Infections
// ══════════════════════════════════════════════════════════════════
s = pres.addSlide();
contentSlide(s, "Bacterial Skin Infections", [
"CELLULITIS & ERYSIPELAS",
" Cellulitis: S. aureus/Strep; non-elevated border; deep dermis/subcutaneous",
" Erysipelas: Group A Strep; sharply demarcated, raised, bright red; superficial dermis",
" Treatment: dicloxacillin/cephalexin; MRSA coverage if purulent (TMP-SMX, doxycycline)",
"FOLLICULITIS / FURUNCLE / CARBUNCLE",
" Folliculitis: superficial follicular pustules; S. aureus most common",
" Furuncle (boil): deep follicular abscess; incision & drainage primary treatment",
" Carbuncle: coalescing furuncles; more systemic involvement; I&D + antibiotics",
"NECROTIZING FASCIITIS",
" Life-threatening surgical emergency; rapid spread along fascial planes",
" Type I (polymicrobial) vs. Type II (Group A Strep — 'flesh-eating')",
" Hard wooden feel on palpation; skin may look deceptively normal early",
" Treatment: immediate surgical debridement + broad-spectrum IV antibiotics",
"METHICILLIN-RESISTANT S. AUREUS (MRSA)",
" CA-MRSA: USA300 clone; skin and soft tissue infections most common presentation",
" Preferred oral agents: TMP-SMX DS, doxycycline, clindamycin (D-zone test for inducible resistance)",
], C.rust);
// ══════════════════════════════════════════════════════════════════
// SLIDE 18 – Fungal & Viral Infections
// ══════════════════════════════════════════════════════════════════
s = pres.addSlide();
twoColSlide(s, "Fungal & Viral Skin Infections",
[
"DERMATOPHYTOSES (TINEA)",
" Tinea capitis: scalp ringworm; oral griseofulvin (topicals inadequate)",
" Tinea corporis: ring-shaped plaque with central clearing; topical azoles",
" Tinea pedis (athlete's foot): interdigital maceration; clotrimazole",
" Tinea unguium (onychomycosis): nail; oral terbinafine ×6–12 weeks",
" Tinea versicolor: Malassezia; hypo/hyperpigmented patches; selenium sulfide shampoo",
"CANDIDIASIS",
" Intertriginous: satellite lesions are pathognomonic",
" Oral thrush: white plaques that scrape off",
" Topical nystatin or azoles; systemic fluconazole for resistant cases",
],
[
"HERPES SIMPLEX (HSV)",
" HSV-1: oral; HSV-2: genital (usually)",
" Grouped vesicles on erythematous base → painful ulcers",
" Tx: acyclovir, valacyclovir (suppressive for recurrent episodes)",
"HERPES ZOSTER (SHINGLES)",
" VZV reactivation; dermatomal distribution",
" Prodrome: burning pain → vesicular rash",
" PHN: most feared complication (esp. >60 yrs)",
" Tx: valacyclovir 1g TID ×7 days (within 72 hr of onset)",
" Prevention: Shingrix vaccine (RZV) ≥50 yrs",
"VERRUCAE (WARTS) — see Childhood section",
"PITYRIASIS ROSEA",
" Herald patch → Christmas tree distribution",
" Associated with HHV-6/7; self-limiting 6–8 weeks",
],
C.rust
);
// ══════════════════════════════════════════════════════════════════
// SLIDE 19 – SECTION 6 HEADER: Infestations
// ══════════════════════════════════════════════════════════════════
s = pres.addSlide();
sectionHeader(s, "06", "Infestations", "Scabies, pediculosis, and other infestations", C.skin, C.amber);
// ══════════════════════════════════════════════════════════════════
// SLIDE 20 – Infestations Content
// ══════════════════════════════════════════════════════════════════
s = pres.addSlide();
twoColSlide(s, "Scabies & Pediculosis",
[
"SCABIES",
" Sarcoptes scabiei mite; female burrows into stratum corneum",
" Intense pruritus — worse at night (hallmark)",
" Sites: web spaces, wrists, areolae, genitalia, waistband area",
" Burrows: thin, linear, serpiginous tracts",
" Norwegian (crusted) scabies: hyperkeratotic plaques; immunocompromised; highly contagious",
" Diagnosis: skin scraping + microscopy for mites/eggs/feces",
" Treatment: permethrin 5% cream (whole body, leave overnight) — first-line",
" Alternative: oral ivermectin 200 mcg/kg ×2 doses (2 weeks apart)",
" All household contacts treated simultaneously",
" Wash all clothing/bedding in hot water",
],
[
"PEDICULOSIS (LICE)",
" P. humanus capitis: head lice; nits firmly attached to hair shafts",
" P. pubis: pubic lice (crabs); STI; check for other STIs",
" P. humanus corporis: body lice; vector for typhus, relapsing fever",
" Treatment: permethrin 1% (capitis), malathion, benzyl alcohol",
" Wet combing: mechanical removal of nits",
" Lindane: third-line only (neurotoxicity risk)",
"",
"LARVA MIGRANS",
" Cutaneous larva migrans: hookworm larvae (Ancylostoma); serpiginous advancing tract",
" Treatment: albendazole or ivermectin",
"",
"MYIASIS",
" Fly larvae infestation; botfly most common in travelers",
" Occlusion technique (petroleum jelly) to expel larvae",
],
C.amber
);
// ══════════════════════════════════════════════════════════════════
// SLIDE 21 – SECTION 7 HEADER: Hypersensitivity Reactions
// ══════════════════════════════════════════════════════════════════
s = pres.addSlide();
sectionHeader(s, "07", "Hypersensitivity Reactions\n& Other Eruptions", "Urticaria, drug reactions, and erythema multiforme", C.skin, C.teal);
// ══════════════════════════════════════════════════════════════════
// SLIDE 22 – Urticaria & Drug Reactions
// ══════════════════════════════════════════════════════════════════
s = pres.addSlide();
contentSlide(s, "Urticaria, Angioedema & Drug Eruptions", [
"URTICARIA (HIVES)",
" Transient wheals (<24 hr/lesion) + pruritus; can be acute (<6 wks) or chronic (>6 wks)",
" IgE-mediated (Type I) or non-immune (NSAIDs, ACE inhibitors, codeine)",
" Treatment: non-sedating antihistamines (cetirizine); omalizumab for chronic refractory",
"ANGIOEDEMA",
" Deep dermis/subcutaneous edema; airway involvement = emergency",
" Hereditary angioedema (C1 inhibitor deficiency): no urticaria; bradykinin-mediated",
" ACE inhibitor-induced: bradykinin mechanism; switch to ARB",
"DRUG REACTIONS",
" Exanthematous (maculopapular): most common type; aminopenicillins, sulfonamides",
" Fixed drug eruption: same site with each exposure; dusky-violet plaque → hyperpigmentation",
" DRESS (Drug Reaction with Eosinophilia and Systemic Symptoms): fever, lymphadenopathy, organ involvement; aromatic anticonvulsants, allopurinol, sulfonamides",
" SJS / TEN (Stevens-Johnson / Toxic Epidermal Necrolysis):",
" SJS: <10% BSA detachment; TEN: >30% BSA; SCORTEN score for prognosis",
" Stop offending drug immediately; burn unit care; IVIG ± cyclosporine",
], C.teal);
// ══════════════════════════════════════════════════════════════════
// SLIDE 23 – Erythema Multiforme
// ══════════════════════════════════════════════════════════════════
s = pres.addSlide();
contentSlide(s, "Erythema Multiforme & Photodermatoses", [
"ERYTHEMA MULTIFORME (EM)",
" Target lesions (three concentric zones): dark center + pale inner ring + red outer ring",
" Most common trigger: HSV-1 (recurrent oral herpes) — 'post-herpetic EM'",
" Also: Mycoplasma pneumoniae, drugs",
" Self-limiting; suppressive acyclovir for HSV-triggered recurrent EM",
"PHOTODERMATOSES",
" Polymorphous light eruption (PMLE): most common; papulovesicular rash on sun-exposed areas",
" Phototoxic reactions: exaggerated sunburn-like response; no prior sensitization (e.g., doxycycline, amiodarone)",
" Photoallergic reactions: Type IV delayed hypersensitivity; requires prior sensitization",
"PITYRIASIS ROSEA (repeated for context)",
" Herald patch (2–5 cm) precedes rash by 1–2 weeks",
" Secondary eruption: Christmas tree pattern on trunk",
" Reassurance; antihistamines for itch; acyclovir may shorten course",
"STASIS DERMATITIS",
" Chronic venous insufficiency; medial malleolus; lipodermatosclerosis in chronic cases",
" Compression stockings essential; low-potency topical steroids for itch",
], C.teal);
// ══════════════════════════════════════════════════════════════════
// SLIDE 24 – SECTION 8 HEADER: Skin Signs of Systemic Disease
// ══════════════════════════════════════════════════════════════════
s = pres.addSlide();
sectionHeader(s, "08", "Skin Signs of Systemic Disease", "Cutaneous manifestations of internal medicine", C.skin, C.rust);
// ══════════════════════════════════════════════════════════════════
// SLIDE 25 – Systemic Disease Cutaneous Manifestations
// ══════════════════════════════════════════════════════════════════
s = pres.addSlide();
tableSlide(s, "Cutaneous Signs of Systemic Disease",
["Disease/System", "Skin Manifestation", "Key Features"],
[
["Diabetes mellitus", "Necrobiosis lipoidica, acanthosis nigricans, diabetic dermopathy", "Shin spots; insulin resistance marker"],
["Lupus erythematosus", "Malar 'butterfly' rash, discoid lupus, photosensitivity", "Spares nasolabial folds; anti-dsDNA"],
["Sarcoidosis", "Lupus pernio, papules, plaques, erythema nodosum", "Non-caseating granulomas"],
["Thyroid disease", "Pretibial myxedema (hyperthyroid), dry/coarse skin (hypothyroid)", "Graves: non-pitting orange-peel texture"],
["Liver disease", "Jaundice, spider angiomas, palmar erythema, pruritus, xanthelasma", "Caput medusae in portal HTN"],
["Vasculitis", "Palpable purpura, livedo reticularis, ulceration", "Non-blanching; IgA vasculitis in children"],
["Malignancy", "Acanthosis nigricans, dermatomyositis, Sweet's syndrome", "Paraneoplastic phenomena"],
["HIV/AIDS", "Seborrheic dermatitis, molluscum, Kaposi sarcoma, recurrent HSV/VZV", "CD4-dependent severity"],
],
C.rust
);
// ══════════════════════════════════════════════════════════════════
// SLIDE 26 – SECTION 9 HEADER: Benign Growths
// ══════════════════════════════════════════════════════════════════
s = pres.addSlide();
sectionHeader(s, "09", "Benign Growths", "Nevi, seborrheic keratosis, cysts, and vascular lesions", C.skin, C.amber);
// ══════════════════════════════════════════════════════════════════
// SLIDE 27 – Benign Growths Content
// ══════════════════════════════════════════════════════════════════
s = pres.addSlide();
twoColSlide(s, "Common Benign Growths",
[
"SEBORRHEIC KERATOSIS",
" Keratinocyte origin; increases with age",
" 'Stuck-on' appearance; varied colors (tan–black)",
" Leser-Trélat sign: sudden eruption → GI malignancy",
" Treatment: curettage, cryotherapy (cosmetic)",
"",
"MELANOCYTIC NEVI (MOLES)",
" Junctional: flat, at dermo-epidermal junction (premalignant potential)",
" Intradermal: raised, flesh-colored; benign",
" Compound: mixed features",
" Blue nevus: Spitz variant; benign",
" Dysplastic nevus: atypical features; increased melanoma risk",
"",
"DERMATOFIBROMA",
" Firm, hyperpigmented papule, usually on legs",
" Dimple sign positive (pinching invaginates lesion)",
" Benign; reassurance only",
],
[
"EPIDERMOID CYST",
" Most common cutaneous cyst; derived from follicular infundibulum",
" Punctum often visible; cheese-like contents",
" Excision when inflamed or cosmetically bothersome",
"",
"LIPOMA",
" Soft, mobile, encapsulated adipose tumor",
" Doughy consistency; non-tender; no treatment needed unless symptomatic",
"",
"VASCULAR LESIONS",
" Cherry angiomas: Campbell de Morgan spots; benign; increase with age",
" Spider angiomas: associated with liver disease or pregnancy",
" Hemangiomas: strawberry hemangioma; involutes by age 7–10; propranolol for problematic cases",
" Pyogenic granuloma: rapidly growing red vascular papule; bleeds easily; curettage or laser",
"",
"KELOID vs. HYPERTROPHIC SCAR",
" Keloid: extends beyond wound margins; higher risk in darker skin types",
" Hypertrophic: stays within wound; more likely to regress",
],
C.amber
);
// ══════════════════════════════════════════════════════════════════
// SLIDE 28 – SECTION 10 HEADER: Malignant Skin Lesions
// ══════════════════════════════════════════════════════════════════
s = pres.addSlide();
sectionHeader(s, "10", "Premalignant & Malignant\nSkin Lesions", "BCC, SCC, melanoma, and actinic keratosis", C.deep, C.rust);
// ══════════════════════════════════════════════════════════════════
// SLIDE 29 – Actinic Keratosis & BCC
// ══════════════════════════════════════════════════════════════════
s = pres.addSlide();
twoColSlide(s, "Premalignant & Basal Cell Carcinoma",
[
"ACTINIC KERATOSIS (AK)",
" Small lesions of epidermal proliferation; sun-exposed areas",
" ~1% risk of progression to SCC",
" Rough, scaly papule on erythematous base; 'sandpaper feel'",
" Treatment: cryotherapy, 5-fluorouracil, imiquimod, PDT",
"",
"BASAL CELL CARCINOMA (BCC)",
" Most common skin malignancy in adults",
" Strong UV association; rarely metastasizes",
" Subtypes:",
" Nodular (most common): pearly papule with rolled border + telangiectasias",
" Superficial: pink scaly patch; trunk/shoulders",
" Sclerosing (morpheaform): ill-defined; worst prognosis; skip lesions via neurotropism",
" Basosquamous: squamous differentiation; higher aggression",
" Treatment: Mohs (recurrent, sclerosing, face); excision; topical imiquimod (superficial)",
],
[
"SQUAMOUS CELL CARCINOMA (SCC)",
" 2nd most common; UV + radiation burn scars",
" Bowen disease: SCC in situ; 5% progress to invasive",
" Marjolin ulcer: aggressive SCC in scar tissue",
" Well-differentiated: keratin pearls, intercellular bridges; cytokeratin positive",
" Poorly differentiated: few keratin pearls; wider excision margins (1 cm)",
" May cause nodal disease + distant metastases",
" Treatment: Mohs or wide local excision",
"",
"MOHS MICROGRAPHIC SURGERY",
" Maximum cure rate for NMSC",
" Maximum preservation of normal tissue",
" Indications:",
" - Recurrent BCC",
" - Sclerosing BCC",
" - Poorly differentiated SCC",
" - Functional/cosmetic areas (eyelid, nose, ear)",
],
C.rust
);
// ══════════════════════════════════════════════════════════════════
// SLIDE 30 – Melanoma
// ══════════════════════════════════════════════════════════════════
s = pres.addSlide();
contentSlide(s, "Melanoma", [
"EPIDEMIOLOGY",
" 3rd most common cutaneous malignancy; incidence rising 5% annually",
" Risk factors: UV exposure, >50 nevi, large congenital nevi, family history, fair skin",
"THE ABCDE CRITERIA",
" A – Asymmetry B – Border irregularity C – Color variation D – Diameter >6 mm E – Evolution (change over time)",
"SUBTYPES",
" Superficial spreading (70%): most common; radial growth phase; usually from preexisting nevi",
" Nodular (15–30%): early vertical growth; worst prognosis at presentation",
" Lentigo maligna (4–15%): melanoma in situ (Hutchinson freckle); sun-damaged skin of elderly",
" Lentigo maligna melanoma: dermal violation of lentigo maligna",
" Desmoplastic (2%): neurotropic; high local recurrence",
" Acral lentiginous: palms, soles, subungual; overrepresented in darker skin types",
"HISTOLOGICAL MARKERS",
" S-100, Melan-A, HMB-45 (most specific — antibody vs. melanoma antigen)",
"STAGING & TREATMENT",
" Breslow thickness: most important prognostic factor",
" Wide excision margins based on Breslow; SLNB if >0.8 mm",
" Adjuvant: BRAF inhibitors (vemurafenib), checkpoint inhibitors (pembrolizumab, nivolumab)",
], C.rust);
// ══════════════════════════════════════════════════════════════════
// SLIDE 31 – Summary / Key Takeaways
// ══════════════════════════════════════════════════════════════════
s = pres.addSlide();
darkSlide(s);
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: "100%", h: 0.12, fill: { color: C.gold } });
s.addShape(pres.ShapeType.rect, { x: 0, y: 5.5, w: "100%", h: 0.125, fill: { color: C.teal } });
s.addText("KEY TAKEAWAYS", {
x: 0.5, y: 0.2, w: 9, h: 0.65,
fontSize: 26, bold: true, color: C.white, fontFace: "Calibri", charSpacing: 4,
});
const takeaways = [
["01 Describe first", "Morphology before diagnosis — lesion type, distribution, associated symptoms"],
["02 Skin type matters", "Fitzpatrick I–II: highest skin cancer risk; darker types: keloid + PIH tendency"],
["03 Atopic triad", "Eczema + asthma + rhinitis; filaggrin mutations central to pathophysiology"],
["04 Psoriasis beyond skin", "5–30% develop psoriatic arthritis; IL-17/IL-23 pathway is treatment target"],
["05 MRSA rising", "TMP-SMX or doxycycline for CA-MRSA; I&D is primary for abscesses"],
["06 Scabies: treat all contacts", "Permethrin 5% cream; ivermectin alternative; pruritus may persist 2–4 weeks post-treatment"],
["07 SJS/TEN = emergency", "Stop causative drug immediately; burn unit; SCORTEN score guides prognosis"],
["08 Skin as a window", "Malar rash → SLE; spider angiomas → liver disease; palpable purpura → vasculitis"],
["09 Melanoma ABCDE", "Evolution (E) is the single most important warning sign; Breslow thickness = prognosis"],
["10 Mohs surgery", "Highest cure rate for BCC/SCC in high-risk locations; tissue-sparing technique"],
];
takeaways.forEach((item, i) => {
const col = i < 5 ? 0 : 1;
const row = i < 5 ? i : i - 5;
const xBase = col === 0 ? 0.35 : 5.2;
const yBase = 1.0 + row * 0.9;
s.addShape(pres.ShapeType.rect, { x: xBase, y: yBase, w: 4.6, h: 0.78, fill: { color: "1E3A54" }, line: { color: i < 5 ? C.teal : C.gold, width: 0.6 } });
s.addText(item[0], { x: xBase + 0.1, y: yBase + 0.05, w: 1.5, h: 0.3, fontSize: 10, bold: true, color: i < 5 ? C.teal : C.gold, fontFace: "Calibri" });
s.addText(item[1], { x: xBase + 0.1, y: yBase + 0.35, w: 4.3, h: 0.38, fontSize: 10.5, color: C.white, fontFace: "Calibri", wrap: true });
});
// ══════════════════════════════════════════════════════════════════
// SLIDE 32 – References / End Slide
// ══════════════════════════════════════════════════════════════════
s = pres.addSlide();
darkSlide(s);
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 0.3, h: "100%", fill: { color: C.teal } });
s.addShape(pres.ShapeType.ellipse, { x: 7.0, y: 1.0, w: 4.5, h: 4.5, fill: { color: C.teal }, line: { color: C.teal }, transparency: 88 });
s.addText("REFERENCES &\nFURTHER READING", {
x: 0.5, y: 0.5, w: 6.5, h: 1.3,
fontSize: 32, bold: true, color: C.white, fontFace: "Calibri",
});
const refs = [
"Usatine RP, Krejci-Manwaring J. Dermatology. In: Textbook of Family Medicine. Elsevier.",
"Fitzpatrick TB et al. Fitzpatrick's Color Atlas and Synopsis of Clinical Dermatology. McGraw-Hill.",
"Habif TP. Clinical Dermatology: A Color Guide to Diagnosis and Therapy. Elsevier.",
"American Academy of Dermatology (AAD) Clinical Practice Guidelines. aad.org",
"Wolff K et al. Fitzpatrick's Dermatology in General Medicine. McGraw-Hill.",
"Bolognia JL, Jorizzo JL, Schaffer JV. Dermatology. Elsevier.",
"UpToDate – Dermatology sections (current clinical guidance).",
];
s.addText(refs.map((r, i) => ({ text: `${i + 1}. ${r}`, options: { breakLine: true, bullet: false, fontSize: 12, color: i % 2 === 0 ? C.white : C.midGray } })),
{ x: 0.5, y: 1.9, w: 9, h: 3.3, fontFace: "Calibri", valign: "top", lineSpacingMultiple: 1.35 }
);
s.addShape(pres.ShapeType.line, { x: 0.5, y: 5.25, w: 9, h: 0, line: { color: C.teal, width: 1 } });
s.addText("Prepared for educational purposes · Usatine & Krejci-Manwaring · 2026", {
x: 0.5, y: 5.32, w: 9, h: 0.3,
fontSize: 10, color: C.midGray, fontFace: "Calibri", align: "center",
});
// ══════════════════════════════════════════════════════════════════
// SAVE
// ══════════════════════════════════════════════════════════════════
pres.writeFile({ fileName: "/home/daytona/workspace/dermatology-ppt/Dermatology_Usatine_Krejci.pptx" })
.then(() => console.log("✅ Saved: /home/daytona/workspace/dermatology-ppt/Dermatology_Usatine_Krejci.pptx"))
.catch(err => { console.error("❌ Error:", err); process.exit(1); });
cd /home/daytona/workspace/dermatology-ppt && node build.js 2>&1
ls -lh /home/daytona/workspace/dermatology-ppt/Dermatology_Usatine_Krejci.pptx
Dermatology Usatine Krejci
Presentation · PPTX
| # | Slides | Content |
|---|---|---|
| Title | 1 | Full title slide with authors & chapter reference |
| Outline | 1 | Visual chapter map with all 10 sections + page numbers |
| 01 | 3 | Principles of Diagnosis — lesion morphology, primary/secondary lesions, Fitzpatrick scale table |
| 02 | 1 | General Management — topical therapy, procedures, systemic, photoprotection |
| 03 | 3 | Childhood Dermatoses — atopic dermatitis, acne, impetigo, molluscum, warts |
| 04 | 2 | Inflammatory Diseases — psoriasis (full detail), rosacea, lichen planus, contact dermatitis |
| 05 | 2 | Infectious Skin Diseases — bacterial (cellulitis, MRSA, NF), fungal & viral (tinea, herpes, zoster) |
| 06 | 1 | Infestations — scabies (permethrin/ivermectin), pediculosis, larva migrans |
| 07 | 2 | Hypersensitivity — urticaria, angioedema, drug reactions, SJS/TEN, EM, photodermatoses |
| 08 | 1 | Skin Signs of Systemic Disease — table covering DM, lupus, sarcoid, thyroid, liver, vasculitis, HIV |
| 09 | 1 | Benign Growths — seborrheic keratosis, nevi, cysts, lipomas, vascular lesions, keloids |
| 10 | 3 | Premalignant & Malignant — AK, BCC subtypes, SCC, Mohs surgery, melanoma ABCDE + staging |
| Summary | 1 | 10 key takeaways |
| References | 1 | 7 authoritative references |
Search for clinical images of melanoma subtypes
melanoma subtypes clinical images superficial spreading nodular lentigo maligna acral
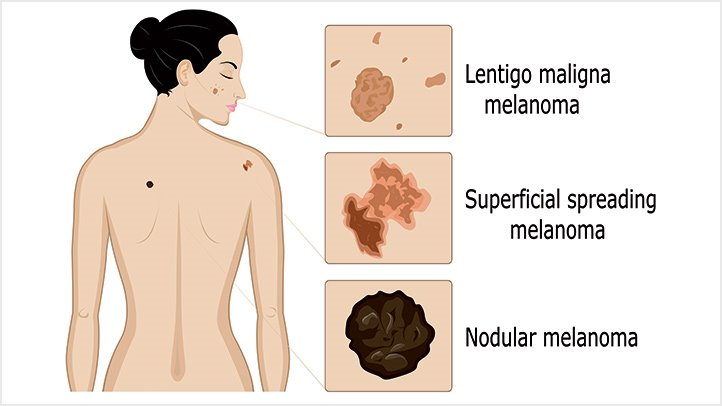
Clinical Images: Melanoma Subtypes
Anatomical Overview — Body Distribution
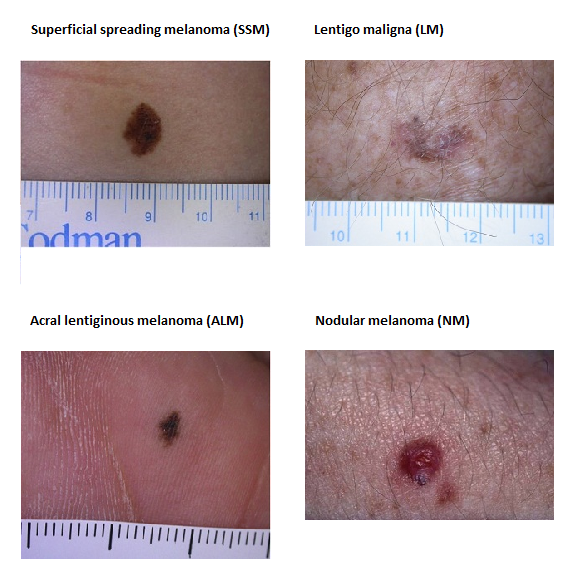
Side-by-Side Clinical Photo Comparison (4 Major Subtypes)
6-Subtype Clinical Panel (Including Rare Variants)

- Superficial Spreading Melanoma - multicolored, irregular border; the most common subtype (55-70%)
- Nodular Melanoma - raised blue-black dome; early lesions may mimic benign lesions
- Lentigo Maligna Melanoma - mottled brown, irregular flat lesion; elderly patients, facial skin
- Acral Lentiginous Melanoma - dark asymmetric plaque on volar skin; disproportionately common in darker-skinned individuals
- Subungual Melanoma - black-brown nail pigmentation with nail plate destruction
- Amelanotic Melanoma - pink/flesh-colored; most dangerous due to lack of pigment causing diagnostic delay
Textbook Figure 116-2 — Fitzpatrick's Dermatology (All Clinical Subtypes)

- A, B - Superficial spreading melanoma; panel A shows extensive central regression (depigmented central zone)
- C - Ulcerated amelanotic nodular melanoma (exophytic, non-pigmented mass)
- D - Pigmented nodular melanoma (blue-black dome)
- E - Lentigo maligna melanoma (flat, mottled brown patch in photodamaged background)
- F - Acral lentiginous melanoma on the sole with typical tan-brown discoloration
SSM — Clinical + Dermoscopy + Histology (H&E + Melan-A IHC)
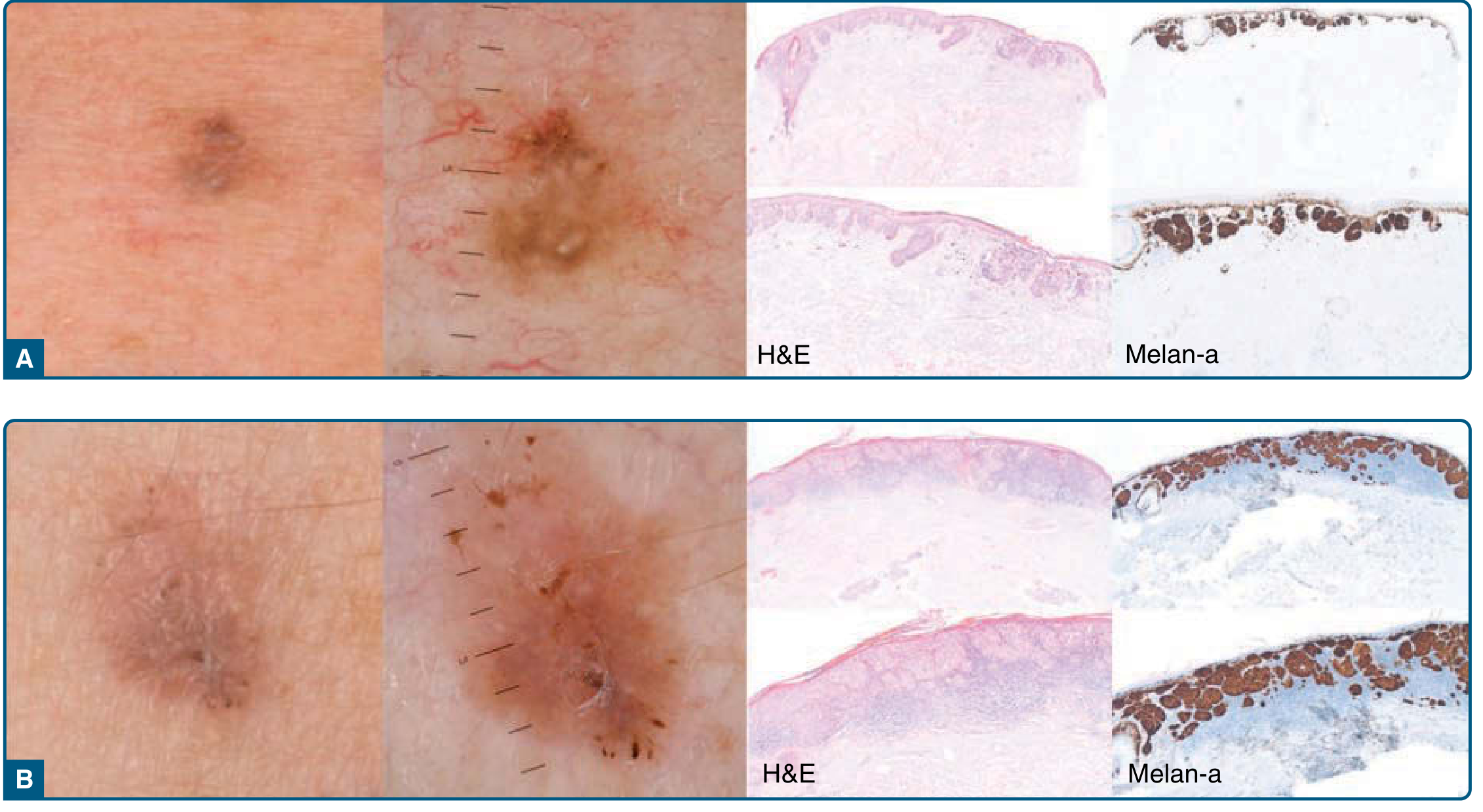
- Clinical view (naked eye) - subtle irregular pigmented patch
- Dermoscopy - atypical pigment network, regression structures, irregular dots/globules
- H&E histology - atypical melanocytes along the dermo-epidermal junction
- Melan-A immunostaining - confirms melanocytic origin (brown chromogen positive cells at DEJ)
Summary Table — Key Distinguishing Features
| Subtype | Frequency | Typical Site | Growth Pattern | Key Hallmark |
|---|---|---|---|---|
| Superficial spreading | 55-70% | Trunk (M), legs (F) | Radial first, then vertical | Multicolor, irregular flat patch |
| Nodular | 15-30% | Any site | Vertical from onset | Blue-black dome; no radial phase; fastest growing |
| Lentigo maligna | 10-15% | Face/head/neck | Radial (prolonged, years) | Slow-growing freckle on photodamaged skin, elderly |
| Acral lentiginous | <5% (US) | Palms, soles, nails | Radial then vertical | Overrepresented in Asian/African populations |
| Desmoplastic | ~2% | Head/neck | Variable | Neurotropic; high local recurrence; NF1 mutations (93%) |
| Amelanotic | 2-20% | Any | Variable | Pink/flesh-colored; most often misdiagnosed; late detection |
| Subungual | Rare | Nails (great toe, thumb) | Variable | Hutchinson sign (periungual pigment) is a red flag |
Breslow thickness remains the single most important prognostic factor across all subtypes, regardless of histological type. Nodular melanoma accounts for ~40% of melanoma deaths despite being the second most common subtype, due to its rapid vertical growth phase. - Fitzpatrick's Dermatology; PMC review of melanoma subtypes