Functional MRI - 20 marks
Reading File
Finding Sources
Searching the Web
functional MRI fMRI principles BOLD signal clinical applications 20 marks
Finding Sources
Searching PubMed
"functional MRI" BOLD signal principles applications
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
I now have thorough content from authoritative textbooks. Let me compose the complete 20-mark answer.
Functional MRI (fMRI)
1. Introduction
Functional MRI (fMRI) is a non-invasive neuroimaging technique that uses a standard MRI scanner to map brain activity in real time by detecting localised changes in cerebral blood oxygenation. Since its development in the early 1990s, it has become the dominant tool for non-invasive functional brain mapping in both research and clinical settings. - Adams and Victor's Principles of Neurology, 12th Edition
2. Physical Basis - The BOLD Effect
The cornerstone of fMRI is the Blood Oxygen Level-Dependent (BOLD) signal, first described by Ogawa and colleagues in 1990.
Neurovascular coupling chain:
- A neuronal task increases local synaptic activity in the relevant cortical region.
- This triggers a local rise in metabolic demand, prompting an almost immediate localised elevation of cerebral blood flow (CBF) to that region.
- The blood flow increase is disproportionately large - it overcompensates for the actual oxygen extracted by the neurons.
- The result is a local increase in the ratio of oxyhaemoglobin (oxyHb) to deoxyhaemoglobin (deoxyHb) in the capillary bed of that region.
Why deoxyHb matters magnetically:
- OxyHb is diamagnetic - it does not distort the local magnetic field.
- DeoxyHb is paramagnetic - it causes local field inhomogeneity, accelerating T2* (and T2) signal decay and thereby reducing MRI signal.
- When neuronal activity increases, deoxyHb falls locally → T2* signal increases slightly (typically ~1% at 1.5 T, larger at higher field strengths).
- This small signal increment is the BOLD signal. - Grainger & Allison's Diagnostic Radiology
The BOLD response evolves over 10-15 seconds following a change in neuronal activity, reflecting the delayed hemodynamic response function (HRF). - Adams and Victor's Principles of Neurology
3. MRI Acquisition Method
- fMRI uses a standard MRI scanner - no exogenous contrast agent is required.
- Sequences used are gradient-echo echo-planar imaging (GRE-EPI), which are extremely sensitive to T2* contrast and allow rapid whole-brain volumetric coverage (one volume every 1-3 seconds).
- Higher static field strengths (3 T, 7 T) produce greater BOLD contrast due to increased susceptibility effects and signal-to-noise ratio.
- The BOLD signal at any voxel is compared between a task/active condition and a rest/baseline condition, and the statistical difference is colour-mapped onto a structural MRI to produce a functional activation map.
4. Experimental Paradigm Design
Two main designs are used:
| Design | Description | Advantages |
|---|---|---|
| Block design | Task and rest alternated in ~20-30 s blocks | High statistical power; simple; best for pre-surgical mapping |
| Event-related design | Brief individual stimuli presented; responses averaged | Allows examination of single trials; more flexible; better temporal resolution |
The paradigm is tailored to the function being mapped: finger-tapping for motor cortex, word-reading tasks for language areas, flickering checkerboard for visual cortex, etc.
5. BOLD fMRI Image
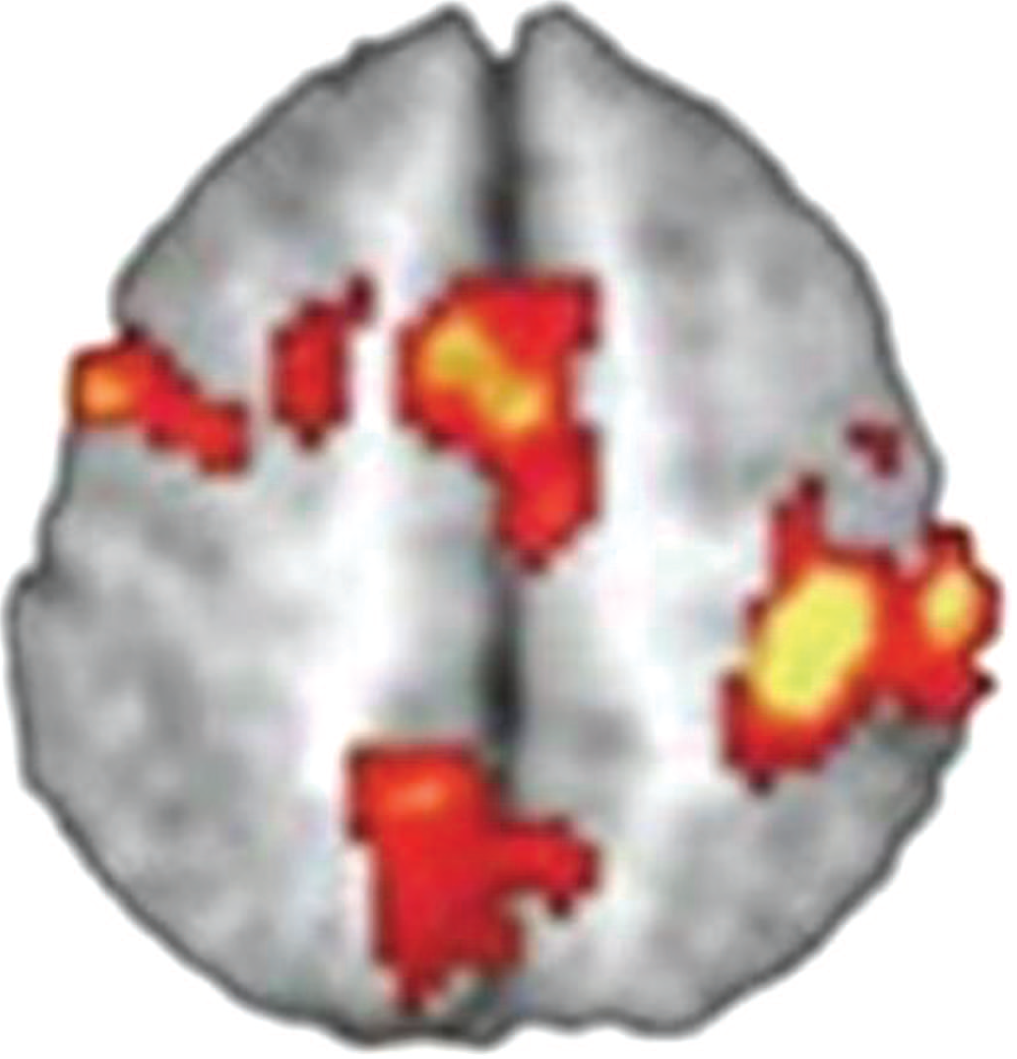
Figure: BOLD fMRI. Colour-coded areas of increased BOLD signal (yellow = maximum activation, red = lesser activation) are superimposed on a grayscale structural axial MRI, corresponding to regions of heightened neuronal activity. - Adams and Victor's Principles of Neurology, 12th Edition
6. Resting-State fMRI
Beyond task-based paradigms, resting-state fMRI (rs-fMRI) measures spontaneous low-frequency (~0.01-0.1 Hz) BOLD fluctuations while the subject does nothing. Correlated fluctuations between brain regions define resting-state networks (RSNs), such as the default mode network (DMN). Resting-state brain activity is reduced in patients with Alzheimer's disease compared with controls. However, rs-fMRI currently remains primarily a research tool due to reduced test-retest reliability. - Grainger & Allison's Diagnostic Radiology
7. Clinical Applications
A. Pre-surgical Brain Mapping (Primary Clinical Use)
The most established clinical application is preoperative cortical mapping before neurosurgery for:
- Brain tumours - fMRI maps eloquent cortex (motor, language, visual areas) adjacent to the tumour, guiding the surgical approach to avoid post-operative deficits.
- Arteriovenous malformations (AVMs) - identifies the spatial relationship between the AVM and functional cortex.
- Epilepsy surgery - localises the language centre and determines hemispheric language dominance. fMRI has largely replaced the invasive Wada test (intracarotid sodium amobarbital injection) for this purpose.
The image below shows fMRI combined with DTI tractography in a patient with a large left frontal AVM. Broca's area (arrow) is immediately posterior to the AVM, and strong left language dominance is confirmed:
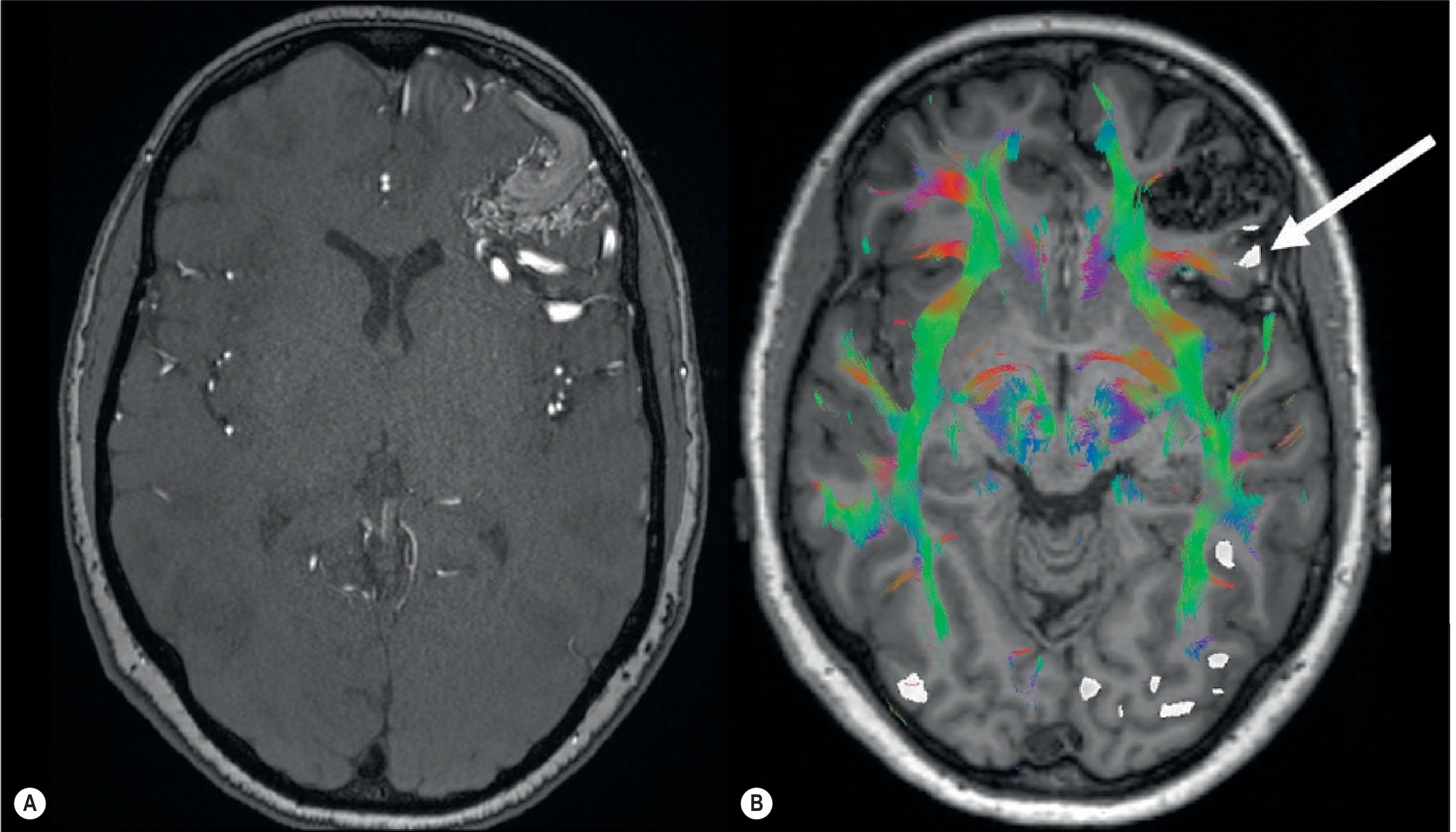
Fig. 53.35 - Grainger & Allison's Diagnostic Radiology: T1 MPRAGE with MR tractography and language-task fMRI shows distorted white matter tracts and Broca's area (arrow) immediately posterior to a left frontal AVM.
B. Cognitive Neuroscience Research
fMRI is the workhorse of cognitive neuroscience, used to study:
- Memory encoding and retrieval
- Attention, decision-making, and executive function
- Language processing (Broca's and Wernicke's areas)
- Sensory processing (somatosensory, visual, auditory cortices)
- Neural plasticity and reorganisation after injury
C. Connectome and Resting-State Network Analysis
fMRI paired with connectome maps is used to visualise task-associated and resting-state network activation. This has applications in understanding disorders such as schizophrenia, depression, and autism. - Adams and Victor's Principles of Neurology
D. Cerebrovascular Reactivity Mapping
By inducing hypercapnia (breath-holding or CO₂ inhalation), fMRI can map cerebrovascular reserve. Brain regions failing to show BOLD signal rise have impaired vascular reactivity, useful in moyamoya disease and atherosclerosis assessment. - ASFNR
8. Integration with Other Techniques
- DTI/MR tractography - fMRI activation maps are co-registered with white matter tractography to provide combined functional and structural connectivity maps (as shown above). This is standard for pre-surgical planning.
- EEG-fMRI - simultaneous acquisition combines high temporal resolution (EEG) with high spatial resolution (fMRI), particularly for epileptic focus localisation.
- PET vs. fMRI - FDG-PET measures glucose metabolism; BOLD fMRI measures relative oxygenation changes. fMRI has superior spatial resolution, no radiation, and superior temporal resolution compared with PET.
9. Limitations
| Limitation | Detail |
|---|---|
| Indirect measure | BOLD signal reflects haemodynamics, not neuronal firing directly; it is a surrogate of neuronal activity |
| Temporal resolution | ~1-2 seconds; sluggish compared to EEG/MEG due to HRF lag (10-15 s) |
| Signal magnitude | BOLD signal is small (~1% at 1.5 T); susceptible to motion, physiological noise (cardiac, respiratory), and magnetic susceptibility artefacts |
| Spatial resolution | Typically 2-3 mm voxels; adequate but limited compared to invasive electrocorticography |
| Neurovascular uncoupling | Pathological states (large AVMs, tumours, stroke) can disrupt the vascular response, giving false-negative maps |
| Individual calibration | Quantitative inter-individual comparison is difficult; limits diagnostic use in individual neuropsychiatric patients |
| Cost and access | Requires MRI infrastructure and specialised analysis software |
10. Comparison with Other Functional Modalities
| Feature | BOLD fMRI | FDG-PET | SPECT | EEG/MEG |
|---|---|---|---|---|
| Spatial resolution | ~2-3 mm | ~4-6 mm | ~8-10 mm | Poor (EEG); moderate (MEG) |
| Temporal resolution | ~1-2 s | Minutes | Minutes | Milliseconds |
| Radiation | None | Yes | Yes | None |
| Contrast agent | None | Yes | Yes | None |
| Measures | Oxygenation (indirect) | Glucose metabolism | CBF | Electrical activity |
11. Advances and Future Directions
- Ultra-high field MRI (7 T) - provides higher spatial resolution and greater statistical significance of BOLD maps.
- Multiband / multiecho sequences - improve raw fMRI data quality by reducing venous signal contamination.
- Acquisition standardisation - efforts to enable quantitative, inter-subject comparisons, potentially allowing fMRI to diagnose neuropsychiatric disorders at the individual level.
- Resting-state fMRI - ongoing investigation for clinical biomarkers in dementia, depression, and schizophrenia. - ASFNR
Summary
fMRI is a non-invasive, non-ionising technique that exploits the BOLD effect to map brain function. Its physical basis is the paramagnetic property of deoxyhaemoglobin: neuronal activity reduces local deoxyHb, increasing the T2* MRI signal. Using GRE-EPI sequences, whole-brain functional maps are acquired rapidly and overlaid on structural images. Clinically, its primary role is presurgical mapping of motor, language, and visual cortex in patients with brain tumours, AVMs, and epilepsy. Combined with DTI tractography, it provides a powerful tool for planning safe neurosurgical corridors. Research applications span the full breadth of cognitive neuroscience, with resting-state analysis emerging as a future clinical biomarker platform.
Sources: Grainger & Allison's Diagnostic Radiology; Adams and Victor's Principles of Neurology, 12th Ed; Neuroanatomy through Clinical Cases, 3rd Ed; Bradley and Daroff's Neurology in Clinical Practice; PMC review on fMRI principles
This is a shared conversation. Sign in to Orris to start your own chat.