Mediastinal anatomy and applied anatomy from fishman and murray full details for md exams 10 marks
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Reading File
I now have comprehensive material from both textbooks. Let me compile the full detailed answer for MD exams.
Mediastinal Anatomy and Applied Anatomy
From Fishman's Pulmonary Diseases & Disorders and Murray & Nadel's Textbook of Respiratory Medicine
1. DEFINITION AND BOUNDARIES
The mediastinum is the potential space between the two pleural cavities. Its boundaries are:
| Wall | Structure |
|---|---|
| Anterior | Sternum |
| Posterior | Vertebral column |
| Superior | Thoracic inlet |
| Inferior | Diaphragm |
| Lateral (bilateral) | Mediastinal pleural reflections |
"The major mediastinal structures are the heart and great vessels, the trachea and main bronchi, and the esophagus, all closely related to one another and connected by loose connective tissue." - Fishman's Pulmonary Diseases and Disorders
Important anatomical feature: The mediastinum communicates freely with both the neck (via fascial planes of the deep cervical fascia) and the retroperitoneum. This continuity allows air, infection, or hemorrhage to disseminate widely.
2. COMPARTMENTS OF THE MEDIASTINUM
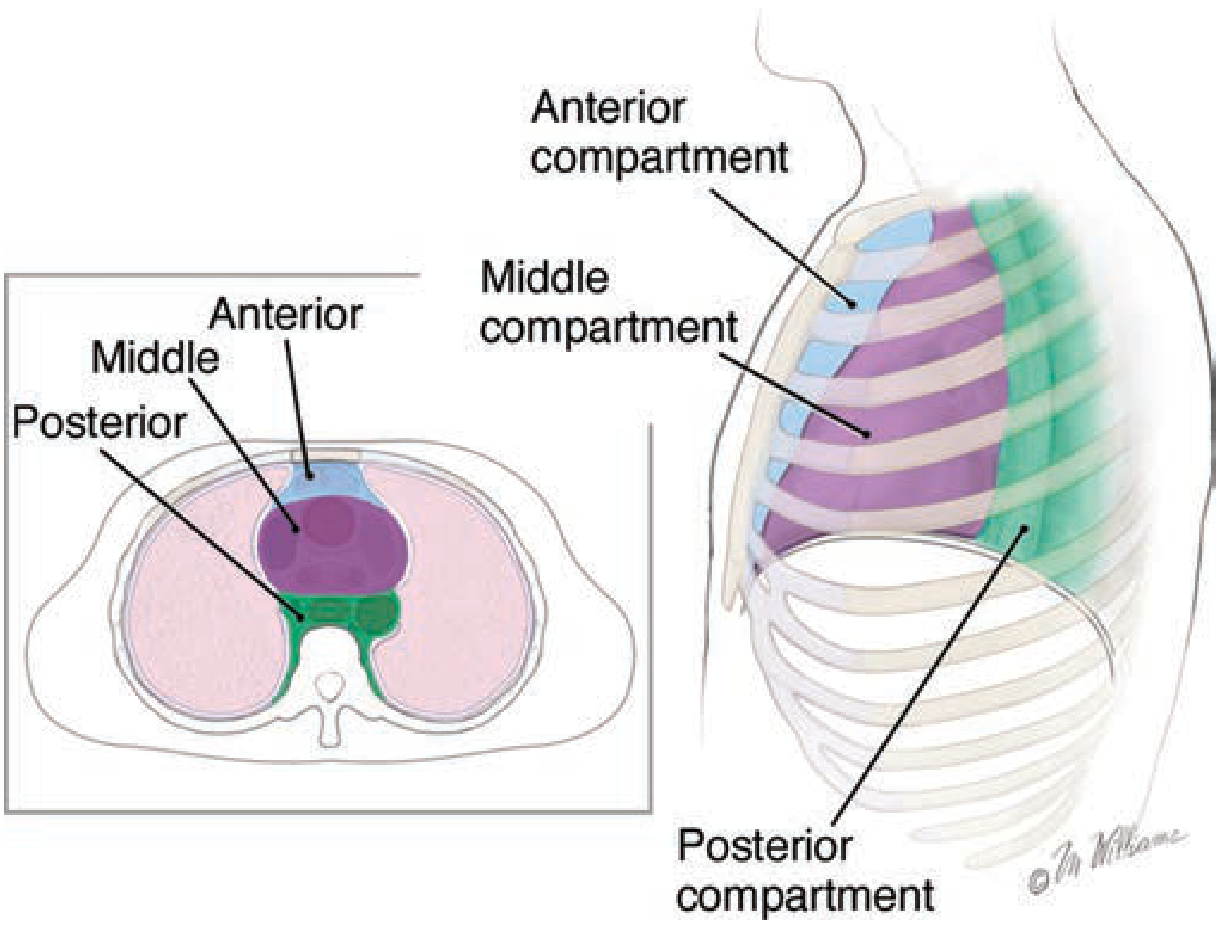
Figure 80-2 from Fishman's: Three-compartment model - anterior, middle, and posterior
The most widely accepted model is the Shields three-compartment subdivision (1972), which is both anatomically sensible and surgically practical. All three compartments extend from the thoracic inlet to the diaphragm.
A. Anterior Compartment (Prevascular)
- Boundaries: Posteriorly by the sternum; posteriorly bounded by the anterior surface of the pericardium and great vessels
- Contents:
- Thymus gland (most important)
- Pericardial fat / fatty tissue
- Lymphatic tissue and lymph nodes
- Internal mammary arteries and veins
- Any substernal extension of thyroid or parathyroid glands
B. Middle Compartment (Visceral)
- Boundaries: From the posterior limit of the anterior compartment to the anterior surface of the vertebral column
- Contents:
- Heart and pericardium
- Trachea and main bronchi
- Esophagus
- Ascending and transverse aorta; aortic arch and its major branches
- Superior vena cava (SVC) and innominate veins
- Pulmonary arteries and hila
- Phrenic nerve and upper vagus nerve
- Multiple lymph node groups
- (In newer CT-based ITMIG classification: also descending aorta, azygos/hemiazygos veins, thoracic duct)
C. Posterior Compartment (Paravertebral Sulcus)
- Boundaries: From the anterior surface of the vertebral column to the anterior surface of the paravertebral ribs
- Contents:
- Azygos and hemiazygos veins
- Thoracic duct
- Sympathetic trunk and chain
- Intercostal nerves
- Lower vagus nerve
- Descending aorta (traditional classification)
- Structures emerging from the spinal canal
TABLE: Contents of Mediastinal Compartments (Fishman's Table 80-1)
| Anterior | Middle (Visceral) | Posterior |
|---|---|---|
| Thymus gland | Pericardium | Azygos and hemiazygos veins |
| Pericardial fat | Heart | Thoracic duct |
| Lymph nodes | Trachea and main bronchus | Sympathetic trunk |
| Esophagus | Intercostal nerves | |
| Aorta | ||
| Phrenic and vagus nerves | ||
| Lymph nodes |
3. UPDATED CT-BASED CLASSIFICATION (ITMIG)
The International Thymic Malignancy Interest Group (ITMIG) revised the compartment model based on axial CT, defining:
- Prevascular = anterior (everything anterior to pericardium; bounded by sternum, first rib, and imaginary curve following anterior heart border)
- Visceral = middle (pericardium anteriorly; a posterior line 1 cm behind anterior margin of each vertebral body)
- Paravertebral = posterior (posterior to visceral compartment; bounded by vertical line at lateral margin of transverse processes)
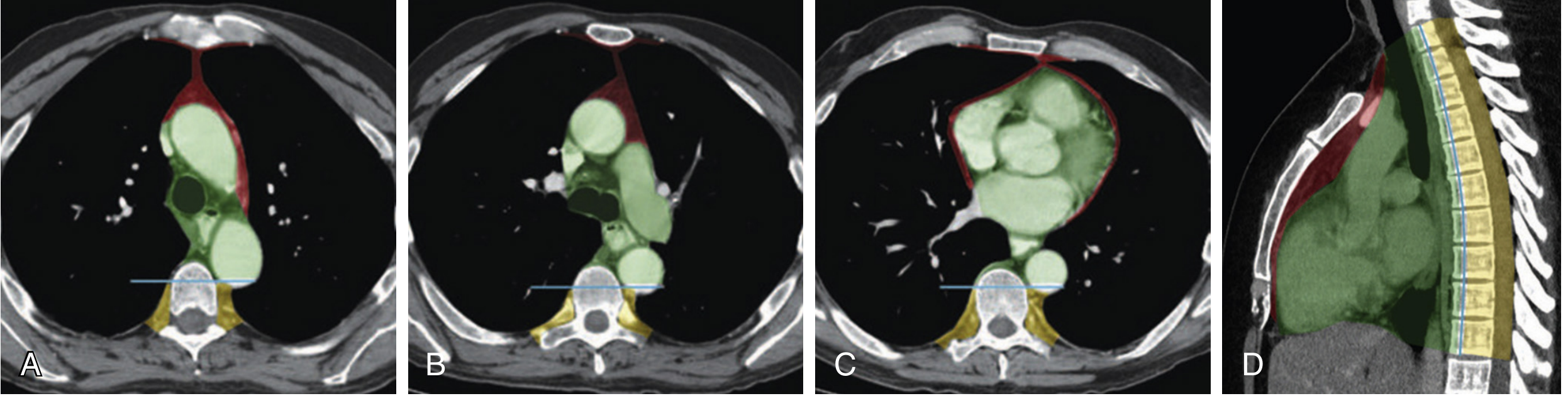
Murray & Nadel Fig. 115.1: CT-based mediastinal compartments at multiple axial levels and sagittal view
4. MEDIASTINAL LYMPHATICS
The mediastinal lymphatic system is complex and interconnected. There are no predictable boundaries; the mediastinum is covered in a dense network of lymphatic vessels and lymph nodes.
Naruke lymph node map (1978) is the standard:
- Stations with single-digit numbers (1-9) = true mediastinal lymph nodes
- Stations with two-digit numbers (10 and above) = within the pleural sac (N2 disease in lung cancer staging are all double-digit)
Clinically important lymph node groups:
- Superior mediastinal nodes (station 1-4): paratracheal, right and left upper and lower paratracheal
- Aortopulmonary nodes (stations 5-6): subaortic, para-aortic
- Inferior mediastinal nodes (stations 7-9): subcarinal (station 7), paraesophageal (station 8), inferior pulmonary ligament (station 9)
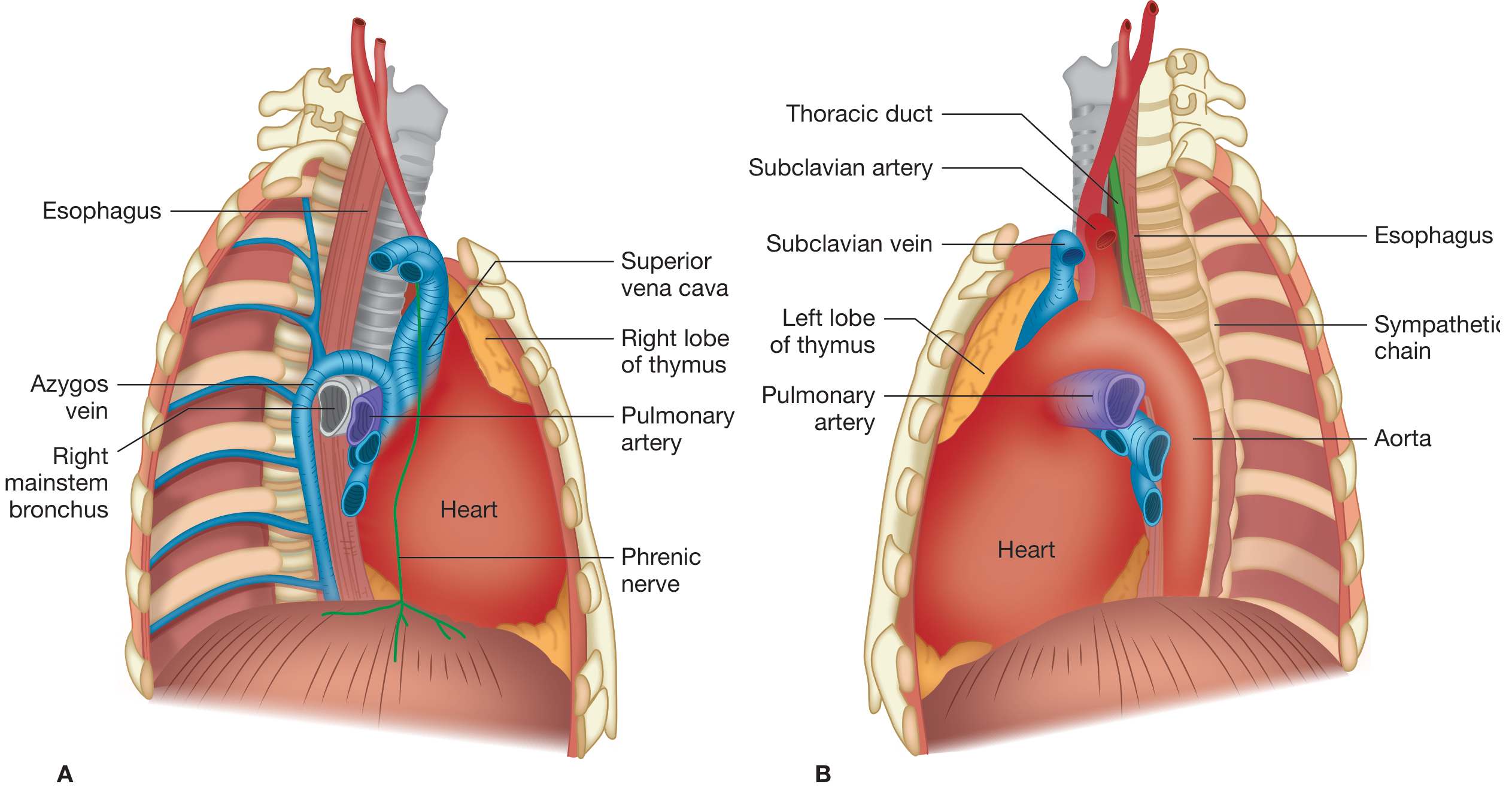
Fishman's Fig. 80-1: A. Right thoracotomy view (esophagus, azygos vein, SVC, right mainstem bronchus, phrenic nerve). B. Left thoracotomy view (thoracic duct, subclavian vessels, sympathetic chain, aorta)
5. FASCIAL PLANES AND COMMUNICATIONS - KEY APPLIED ANATOMY
This is high-yield for exam and clinical practice:
The deep layer of the deep cervical fascia ensheaths the trachea and esophagus as they descend into the mediastinum, creating a visceral space. This space:
- Extends into the hilum of the lung
- Merges with bronchovascular sheaths surrounding terminal bronchioles, arteries, and veins
- The bronchovascular sheath is continuous with the pericardium
Clinical significance:
- Air, pus, or blood can disseminate from the mediastinum to the neck or retroperitoneum via these fascial planes
- Alveolar rupture → air enters perivascular interstitium → dissects proximally within bronchovascular sheath → reaches mediastinum (Macklin mechanism, 1944)
- From mediastinum: air can enter pericardial space (pneumopericardium), dissect along adventitia of great vessels, or decompress into cervical/subcutaneous/retroperitoneal spaces
- The pericardial sac is the only true anatomic compartment of the mediastinum and forms a strong barrier to infection
6. APPLIED ANATOMY - CLINICAL CORRELATIONS
A. Superior Vena Cava (SVC) Syndrome
- The SVC is thin-walled with low intravascular pressure - vulnerable to extrinsic compression
- Any middle mediastinal mass can compress the SVC
- Features: Dilation of collateral veins in upper thorax and neck; facial, neck, and upper torso edema and plethora; neurologic symptoms (headache, disturbed consciousness, visual distortion)
- Common causes: Bronchogenic carcinoma and lymphoma are most frequent; fibrosing mediastinitis for long-standing SVC syndrome
B. Nerve Compression Syndromes
| Nerve | Location in Mediastinum | Effect of Compression |
|---|---|---|
| Recurrent laryngeal nerve | Left side loops under aortic arch | Hoarseness |
| Phrenic nerve | Middle mediastinum (anterolateral) | Diaphragmatic paralysis, dyspnea |
| Vagus nerve | Middle/posterior mediastinum | Tachycardia, autonomic effects |
| Sympathetic chain | Posterior mediastinum/paravertebral | Horner syndrome (ptosis, miosis, anhidrosis, enophthalmos) |
| Spinal cord | Posterior compartment | Cord compression symptoms |
C. Mediastinal Mass - Compartment-Based Differential Diagnosis
A key clinical application: the compartment in which a mass arises strongly predicts its nature.
| Compartment | Most Common Masses ("4 T's") |
|---|---|
| Anterior | Thymoma, Teratoma (germ cell tumors), Thyroid (substernal goiter), Terrible lymphoma |
| Middle | Lymphoma, Bronchogenic cysts, Pericardial cysts, Vascular (aortic aneurysm), Tracheal tumors, Sarcoidosis/granuloma |
| Posterior | Neurogenic tumors (most common in children), Esophageal lesions, Thoracic spine lesions, Meningocele |
Epidemiology (combined series of 3017 adults):
- Thymomas and thymic cysts: 26.5% (most common)
- Neurogenic tumors: 20.2%
- Germ cell tumors: 13.8%
- Lymphomas: 12.7%
- Foregut cysts: 10.3%
- In children: neurogenic tumors are most common (41%)
"About 80% of asymptomatic masses are benign, whereas more than half of those that produce symptoms are malignant." - Murray & Nadel
D. Pneumomediastinum (Mediastinal Emphysema)
- Accumulation of air in mediastinum
- Spontaneous pneumomediastinum incidence: 22 cases per 1,000,000 emergency department visits
- Presentation: Substernal pain (often pleuritic, radiating to neck or back), dyspnea, dysphagia, dysphonia; Hamman sign (crunching/clicking sound over precordium synchronous with heartbeat)
- Radiology: Thin radiolucent strip along mediastinal fascial plane, most commonly along the left heart border; CT more sensitive
- Differentiate from esophageal perforation: Older age, higher WBC, pleural effusion on imaging (54% vs 0%), history of instrumentation or severe retching
Etiology of Pneumomediastinum:
- Upper respiratory tract: head/neck infections, facial fractures, laryngeal trauma (intubation), dental procedures
- Lower respiratory tract: trauma, bronchoscopy
- Lung: mechanical ventilation (Valsalva/elevated airway pressure), spontaneous
- Esophagus: perforation (Boerhaave syndrome), instrumentation
- Gastrointestinal: perforated viscus
E. Acute Mediastinitis
- Most common cause: Esophageal perforation or descending cervical infection
- Spreads rapidly via fascial planes connecting neck, mediastinum, and retroperitoneum
- Presents with fever, chest pain, dysphagia, and rapidly progressive sepsis
- High mortality without prompt surgical drainage
F. CT Imaging Features and Differential Diagnosis (Murray & Nadel Table 115.1)
| CT Feature | Likely Etiology |
|---|---|
| Fat density | Mediastinal lipomatosis, thymolipoma, teratoma |
| Calcification (rim) | Cystic thymoma, thyroid adenoma, aneurysm, teratoma |
| Calcification (central) | Goiter, teratoma, treated lymphoma, sarcoidosis |
| Teeth or bone in mass | Teratoma (pathognomonic) |
| Air-fluid level | Esophageal disease, abscess, developmental cyst |
| SVC obstruction | Bronchogenic carcinoma, lymphoma, fibrosing mediastinitis |
| Bone/rib erosion | Metastatic disease, neurogenic tumor, meningocele, aneurysm |
| Intensely enhancing | Vascular abnormality, paraganglioma, Castleman disease, thyroid mass |
7. SUMMARY TABLE FOR QUICK REVISION
| Feature | Key Point |
|---|---|
| Boundaries | Sternum (ant), vertebra (post), thoracic inlet (sup), diaphragm (inf) |
| Compartments | Anterior, Middle, Visceral, Posterior (paravertebral) |
| True anatomic compartment | Pericardial sac only |
| Communicates with | Neck (via deep cervical fascia) and retroperitoneum |
| Most common adult mediastinal mass | Thymoma (anterior) |
| Most common pediatric mediastinal mass | Neurogenic tumor (posterior) |
| 4 T's of anterior mediastinum | Thymoma, Teratoma, Thyroid, Terrible lymphoma |
| SVC syndrome cause | Middle mediastinal mass compressing thin-walled, low-pressure SVC |
| Hamman sign | Crunching sound over precordium = pneumomediastinum |
| Horner syndrome | Posterior mediastinal mass compressing sympathetic chain |
| Air spread mechanism | Macklin effect: alveolar rupture → bronchovascular sheath → mediastinum |
| Naruke node stations 1-9 | True mediastinal nodes |
| Naruke node stations ≥10 | Hilar/intrapulmonary (within pleural sac) |
Sources:
- Fishman's Pulmonary Diseases and Disorders, 2-Volume Set (Ch. 80 - Mediastinum: Anatomy, Pneumomediastinum; Ch. 82 - Mediastinal Neoplasms)
- Murray & Nadel's Textbook of Respiratory Medicine, 2-Volume (Ch. 115 - Mediastinal Disease)
This is a shared conversation. Sign in to Orris to start your own chat.