PHYSICAL EXAMINATION
LOCAL EXAMINATION
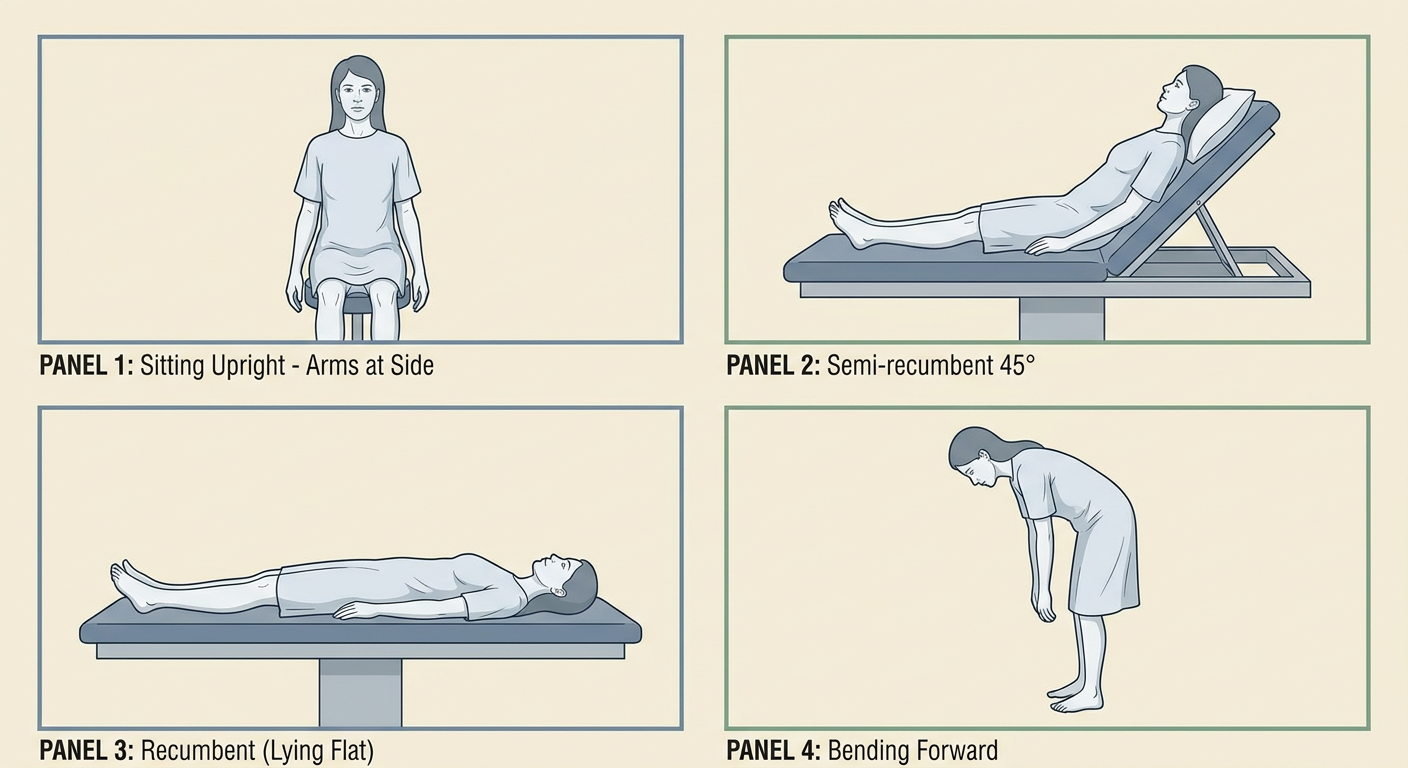
The patient must be stripped to the waist to expose completely both the breasts before inspection is commenced. There must be adequate privacy so that the patient can be relaxed. The examining area must be well lighted so that subtle changes in the skin can be identified. The examination of breast is performed mainly with the patient in sitting posture. This gives more information regarding the level of the nipples (Fig. 30.1), a lump and palpation of the axillary lymph nodes. Examination may also be performed in semirecumbent (45°) position. This position is a good compromise between lying flat which makes the breasts flatten out and fall sideways, and sitting upright which
makes the breasts pendulous and bulky. Examination can also be performed in the recumbent one can examine the patient in bending forward position which gives information regarding retraction of the nipple. Always compare both the breasts in inspection.
A. INSPECTION
above her head when the lump or dimple may be more marked. (iii) with the hands on her hips This is carried out: (1) with the arms by the side of the body, (ii) with the arms raised straight pressing and relaxing as the surgeon commands when abnormal movement of the nipple or exaggeration of skin dimples may be evident and lastly (iv) with the patient bending forwards from the waist so that the breasts fall away from the body. Any failure of one nipple to fall away from the chest indicates abnormal fibrosis behind the nipple. Inspection of the whole breast should be done systematically.
1. Breasts: Both the breasts are inspected in their entirety and the following points are noted-(i) Position-whether displaced in any direction. (ii) Size and shape-whether larger or smaller than its fellow (Fig. 30.2). Sometimes males breast becomes enlarged-the condition is known as gynecomastia, (iii) Any puckering or dimpling? In scirrhous carcinoma the breast may be shrunken and drawn in towards the growth. Dimpling of the skin may be made prominent by lifting the breast gently upwards (Fig. 30.3). In presence of a swelling or an ulcer determine its position (in relation to four quadrants of the breast), size, shape and surface.
2. Skin over the breast: (i) Color and texture: In acute mastitis the skin becomes red, warm and edematous. Similar picture may be seen very rarely in acute mastitis carcinomatosa (acute lactational carcinoma). (ii) Engorged veins. Presence of engorged veins is commonly seen in large soft fibroadenoma (cystosarcoma phyllodes) and in rapidly growing sarcoma. Engorged veins may also be seen when there is presence of acute lactational mastitis with huge breast abscess. (iii) Dimple, retraction or puckering is often noticed in scirrhous carcinoma of the breast (Figs. 30.4 and 30.5). (iv) Peau d' orange is a classical sign in case of carcinoma of the breast (Fig. 30.6). This is due to blockage of subcuticular lymphatics with edema of the skin which deepens the mouths of the sweat glands
and hair follicles giving rise to the typical 'orange peel' appearance. (v) Nodules may be observed in the breast which are often metastatic (vi) Ulceration and fungation: There may be ulceration in any part of the skin of the breast which are examined according to Chapter 4. Fungation of the skin is a late feature of advanced carcinoma of the breast due to infiltration of the skin by the growth (Fig. 30.7). Fungation may also occur in case of large soft fibroadenoma or in a rapidly-growing sarcoma due to the fact that the skin becomes atrophied at the site of maximum pressure over the huge swelling and ultimately gives way so that the growth fungates out. But in this case the skin is not infiltrated. This can be demonstrated by means of a probe which can be passed underneath the skin margin in this case, but this is not possible in case of a fungating carcinoma where the skin is infiltrated
Nipple: (1) Presence: Are both nipples present and symmetrical or one is retracted or destroyed. (ii) Its position: Compare the level of the nipples on both sides (Fig. 30.8). Vertical distance from the clavicle and horizontal distance from the midline should be considered. In carcinoma, nipple of the affected side is drawn up towards the lump. It should be remembered that inflammatory fibrosis may cause similar clevation of the nipple. This elevation of the nipple will be more marked if the patient is asked to raise both the hands above the head (Fig. 30.9). Nipple may be displaced away from the lump in case of fibroadenoma. Nipple may be destroyed when Paget's disease has almost eroded the nipple or a fungated carcinoma has destroyed the nipple. (iii) Number: Accessory nipples may be present besides the normal ones. These are usually found anywhere along the milk line (ridge) which extends from the axilla to the groin. Such accessory nipple has also been seen on the inner aspect of the thigh. Milk may discharge through these nipples also during lactation. (iv) Size and shape: Is it prominent, flattened or retracted? Prominence of the nipple may be due to an underlying swelling such as a cyst. Slight retractión may be seen since puberty. Recent retraction of the nipple with the onset of the present illness is very much significant. Most often it is due to carcinoma of the breast and occasionally due to chronic inflammation (Figs. 30.10 to 30.12). In Paget's disease, the nipple is completely destroyed, a red and flat ulcer being present in its place. (v) Surface: Look for cracks, fissures or eczema. (vi) Discharge if any: Note the character (see above). Is the discharge coming from the nipple or from its immediate neighborhood (mammary fistula)?
Fig. 30.8: Best method to demonstrate the levels of the nipples. Note slight elevated level on the right side affected by carcinoma
Fig. 30.9: Note how retraction of the nipple can be made more prominent by raising both hands above the head.
4. Areola: The normal areola is slightly corrugated and contains a few small nodules-Montgomery's glands. These glands become larger during pregnancy when these are known as Montgomery's tubercles. (i) Color: The skin of areola of young girl is pale pink, but it becomes slightly darker in adult life. It becomes brown during pregnancy. (ii) Size: It becomes larger in case of a huge swelling of soft fibroadenoma or sarcoma. Diminution of the size of the areola is sometimes noticed in scirrhous carcinoma. (iii) Surface and texture: Look for crack, fissure, ulcer, eczema, swelling or discharge. In Paget's disease, the areola becomes bright red in the early stage and is destroyed leaving a red weeping ulcer later on. It is useful to remember that eczema is usually a bilateral affection, whereas Paget's disease is purely unilateral. As mentioned earlier glands of Montgomery may become hypertrophied during pregnancy and lactation to produce small swellings here. This is not a pathological condition. Occasionally Montgomery's gland may be enlarged forming a
A
DHHO
retention cyst similar to a sebaceous cyst. Such cyst may
5. Arm and thorax: After completing inspection of the
breast a quick look at the arm of the affected side and the thoracic wall may be well informatory. Cancer en cuinasse,' i.e., multiple cancerous nodules and thicken infiltrated skin like a coat of armour may be seen in the arm and the thoracic wall. Brawny edema of the arm may be due to extensive neoplastic infiltration of the axillary lymph nodes. It is mainly due to lymphatic blockage. Edematous arm may also be seen after radical mastectomy. It is also a feature of lymphatic obstruction,
but infection may play a contributory role. 6. Axilla and supraclavicular fossa: These regions
should particularly be inspected for any swelling due to enlarged lymph nodes. The students must make a habit of inspecting these regions, so that he should never ignore these regions. Subsequently he has to palpate these regions.
the left breast. Fig. 30.12: Retraction of nipple with peau d' orange is clearly seen in a case of carcinoma of
7. The patient is asked to raise her arms above her head. This is the last part of inspection
and should not be missed. The change in the shape of the breast caused by lifting the arms often reveals lumps, puckering and distortion, not visible when the arms are by the sides. This action also reveals the lower surfaces of the breasts. If the submammary fold is still not visible, lift up the breast and inspect it. This may reveal a swelling which was missed so long, as also skin nodules (metastatic) or presence of any skin disease. In this position the clinician should inspect the anillae properly for swelling, skin puckering and ulceration. The shoulder movements are als noticed which may be affected by lymph node enlargement in the axilla.
Simplified