Describe the autopsy procedures in Annesthetic deaths, 10 marks FMT pg answer
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
The library does not contain a Forensic Medicine & Toxicology textbook. I've exhausted my database queries. I will now provide a comprehensive answer from my knowledge base, which covers standard FMT textbook content on this topic (as taught in Indian medical curricula - Reddy's/Pillay's FMT).
Autopsy Procedures in Anaesthetic Deaths (10 Marks - FMT)
Definition
An anaesthetic death is one in which death occurs during or immediately after the administration of an anaesthetic agent, whether due to the anaesthetic itself, its complications, or concurrent surgical/patient factors. These are medico-legally significant deaths requiring a thorough medicolegal autopsy.
Classification of Anaesthetic Deaths
Before describing autopsy procedures, the examiner must know that anaesthetic deaths are broadly classified as:
- Deaths due to the anaesthetic agent itself (e.g., drug overdose, idiosyncratic reaction, malignant hyperthermia)
- Deaths due to anaesthetic technique (e.g., failed intubation, aspiration, laryngospasm)
- Deaths due to concurrent disease (patient's pre-existing condition aggravated)
- Deaths due to surgical complications occurring under anaesthesia
General Considerations Before Autopsy
- Treat as a medicolegal case - the autopsy must be performed by a Forensic Medicine specialist or experienced pathologist.
- Collect all clinical records - anaesthetic chart, pre-operative assessment, drug charts, operation theatre records, and nursing notes.
- Note the anaesthetic agents used - general, regional, local, inhalational, or intravenous agents; their doses and timing.
- Note the sequence of events - when the patient lost consciousness, when collapse occurred, and resuscitative measures taken.
- External examination must be conducted before the internal examination.
External Examination
- General appearance - note pallor, cyanosis, or plethora of the body.
- Cyanosis - examine lips, fingernails, and toenails for central/peripheral cyanosis; central cyanosis suggests airway compromise or respiratory failure.
- Jaundice - may indicate hepatotoxicity (e.g., halothane hepatitis).
- Needle marks and puncture sites - locate all injection and infusion sites; number, site, and character must be recorded.
- Endotracheal tube/IV cannula - do NOT remove before autopsy; note position, patency, and kinking of the ET tube. An improperly placed ET tube (oesophageal intubation) is a critical finding.
- Injuries - examine for pressure sores, burns (from diathermy), or positional injuries from prolonged surgery.
- Dependent lividity (hypostasis) - note its colour and distribution; cherry-pink lividity may suggest CO/cyanide poisoning if certain volatile agents were used.
- Body weight - important for calculating whether correct doses were administered.
Internal Examination
1. Brain and Central Nervous System
- Examine for cerebral oedema, which is a common finding in anaesthetic deaths.
- Look for subarachnoid haemorrhage, pontine haemorrhage, or hypoxic-ischaemic encephalopathy.
- Histology: Neuronal eosinophilia with nuclear pyknosis (red neurons) is evidence of hypoxic injury.
2. Respiratory System (Critical in Anaesthetic Deaths)
- Larynx and trachea: Examine for laryngospasm signs (mucosal oedema, haemorrhage), foreign body, vomitus, or blood.
- Lungs: Weigh both lungs.
- Pulmonary oedema - frothy fluid from cut surface is classic; weigh lungs (normally ~300-400g each; in oedema may exceed 1000g each).
- Aspiration pneumonitis (Mendelson's syndrome) - food particles, bile-stained material in airways and lung parenchyma; common when patient was not kept fasting.
- Atelectasis and patchy collapse.
- Congestion - uniform dark-red, airless lung.
- Smell the lungs for volatile anaesthetic agents (ether, chloroform, halothane).
- Position of the ET tube - confirm tip lies in the trachea at or above the carina, NOT in the oesophagus or right main bronchus (right-sided atelectasis/left overinflation).
3. Cardiovascular System
- Heart weight - increased in hypertensive/ischaemic disease.
- Examine for coronary artery stenosis - cross-section coronaries every 3 mm; >75% stenosis indicates pre-existing disease.
- Look for myocardial infarction (recent or old) or contraction band necrosis (catecholamine surge).
- Cardiac arrhythmia deaths: No specific gross findings; histology is essential. Halothane sensitises the myocardium to catecholamines causing ventricular fibrillation.
- Examine the conduction system (AV node, bundle of His) histologically in suspected arrhythmia deaths.
4. Liver
- Look for hepatic necrosis - centrizonal necrosis is characteristic of halothane hepatitis (immune-mediated).
- Note colour - yellow (fatty change), pale (ischaemic), or mottled (nutmeg liver in congestion).
- Send tissue for histology.
5. Kidneys
- Examine for acute tubular necrosis (ATN) due to hypoperfusion or nephrotoxic agents (e.g., methoxyflurane).
- Note cortical pallor, tubular congestion.
6. Adrenal Glands
- Examine for haemorrhage (Waterhouse-Friderichsen syndrome) or depletion of lipid (stress response).
Special Investigations Mandatory in Anaesthetic Deaths
Toxicological Samples (Collected at Autopsy)
Collected before formalin fixation or embalming:
| Sample | Container | Purpose |
|---|---|---|
| Blood (from femoral/subclavian vein - NOT heart) | Fluoride oxalate tube | Drug levels of anaesthetic agents |
| Urine | Plain container | Drug screening |
| Vitreous humour | Plain syringe | Biochemical analysis (electrolytes, glucose) |
| Bile | Plain container | Accumulates lipophilic drugs |
| Liver (100g) | Plain/refrigerated | Halothane/volatile agent estimation |
| Lung tissue | Plain/refrigerated | Smell and volatile agent analysis |
| Gastric contents | Sealed jar | Aspiration material, unabsorbed drugs |
| Brain (100g) | Plain/refrigerated | Drug analysis |
| Injection site tissue | Formalin | Histology of drug infiltration |
Note: Blood must be taken from a peripheral vein (femoral), NOT the cardiac chambers - postmortem redistribution from the gut can falsely elevate drug levels from central samples.
Histological Samples
- Brain, lungs, liver, kidneys, heart, adrenals - all in 10% formalin.
- Special stains: Masson's trichrome (fibrosis), PAS (glycogen), Oil Red O (fat).
Microbiological Cultures
- If infection/sepsis is a contributing factor.
Specific Findings in Common Anaesthetic Deaths
| Cause | Key Autopsy Finding |
|---|---|
| Oesophageal intubation | ET tube in oesophagus; massive gastric distension; bilateral lung collapse |
| Aspiration (Mendelson's) | Food/bile in airways; haemorrhagic pneumonia; acidic gastric contents |
| Malignant hyperthermia | Muscle rigidity; rhabdomyolysis; haemorrhagic discolouration of muscles; raised CK on vitreous biochemistry |
| Halothane hepatitis | Centrizonal hepatic necrosis on histology |
| Succinylcholine apnoea | No gross findings; blood collected for pseudocholinesterase levels |
| Anaphylaxis | Laryngeal oedema; urticaria; pulmonary oedema; mast cell degranulation on histology; serum tryptase elevated |
| Hypoxia | Petechiae on serosal surfaces; pulmonary oedema; congested viscera |
| Air embolism | Frothy blood in right heart; open heart chambers under water (produces bubbles) |
Medicolegal Significance and Report
- The autopsy report must state whether death was due to anaesthesia, or anaesthesia was merely incidental to an underlying disease.
- The standard of care must be assessed - was the agent, dose, and technique appropriate?
- The anaesthetic chart should be scrutinised for documentation of vital signs, drug doses, and emergency measures.
- Classify the death as: avoidable, unavoidable, or unforeseeable.
- The report must be objective - it may be used in criminal proceedings (if negligence is alleged) or civil litigation.
Summary Points for 10-Mark Answer
- Treat as medicolegal autopsy; collect all hospital records before starting.
- Do NOT remove ET tube/IV lines before examination - their position is critical evidence.
- External examination: cyanosis, jaundice, injection sites, ET tube position.
- Respiratory system is the most important system to examine - aspiration, oedema, laryngospasm, ET tube placement.
- Cardiovascular system: coronary artery disease, conduction system histology.
- Liver: halothane hepatitis (centrizonal necrosis).
- Mandatory toxicology: peripheral venous blood, urine, vitreous, bile, liver, gastric contents.
- Histology from all major organs is mandatory.
- Special tests: serum tryptase (anaphylaxis), pseudocholinesterase levels (succinylcholine apnoea), CK (malignant hyperthermia).
- Report must address cause of death, standard of care, and medicolegal opinion.
Reference: Based on standard FMT textbook content as covered in Reddy's The Essentials of Forensic Medicine and Toxicology (32nd-34th editions) and Pillay's Forensic Medicine and Toxicology - the standard Indian FMT texts used in undergraduate and postgraduate examinations.
Note: The medical library in this system does not currently contain a Forensic Medicine & Toxicology textbook, so this answer is drawn from established FMT textbook knowledge. The content reflects the standard exam-oriented format expected for a 10-mark FMT question on anaesthetic deaths.
Discuss functional tumors of ovary , make an apt exam answer for 20 marks, for pg pathology exam
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the content and images needed for a complete, textbook-backed 20-mark PG pathology answer. Here it is:
Functional Tumors of the Ovary
PG Pathology - 20 Marks
Introduction and Definition
Functional (hormone-secreting) tumors of the ovary are a subset of sex cord-stromal tumors - neoplasms derived from the sex cords and ovarian stroma/mesenchyme that retain the capacity to elaborate steroid hormones (estrogens or androgens), thereby producing clinically recognizable endocrine syndromes. They account for 5-8% of all ovarian malignancies and are distinct from the more common epithelial tumors.
The principal cells of origin mirror the normal gonadal architecture:
- "Female" cells - granulosa cells and theca cells (estrogenic)
- "Male" cells - Sertoli cells and Leydig cells (androgenic)
Classification (WHO / Berek & Novak)
Sex Cord-Stromal and Steroid Cell Tumors
├── 1. Granulosa-Stromal Cell Tumors
│ ├── A. Granulosa cell tumor (Adult / Juvenile)
│ └── B. Thecoma-Fibroma group
│ ├── Thecoma (estrogenic)
│ ├── Fibroma (non-functional)
│ └── Unclassified
├── 2. Androblastomas / Sertoli-Leydig Cell Tumors
│ ├── Well-differentiated (Sertoli cell, Sertoli-Leydig, Leydig/hilus cell)
│ ├── Moderately differentiated
│ ├── Poorly differentiated (sarcomatoid)
│ └── With heterologous elements
├── 3. Gynandroblastoma
├── 4. Sex cord tumor with annular tubules (SCTAT)
├── 5. Sex cord-stromal tumors, unclassified
└── 6. Steroid cell tumors
├── Stromal luteoma
├── Leydig cell tumor (hilus cell tumor)
└── Steroid cell tumor, NOS
A. Granulosa Cell Tumor (GCT)
Incidence and Types
- Most common malignant sex cord-stromal tumor; 2-5% of all ovarian malignancies.
- Granulosa-stromal tumors as a group = 70% of sex cord-stromal tumors.
- Two subtypes:
- Adult GCT (AGCT): 95% of cases; postmenopausal women predominantly.
- Juvenile GCT (JGCT): 5% of cases; children and women <30 years.
- Bilateral in only 2% of patients.
Molecular Pathology
- FOXL2 somatic mutation (C134W) is present in up to 97% of adult GCTs - the single most important molecular marker. FOXL2 is a transcription factor required for normal granulosa cell development. This mutation is NOT seen in juvenile GCT.
- DICER1 mutations are associated with Sertoli-Leydig tumors (not GCT).
Gross Pathology
- Range from a few mm to >20 cm diameter.
- Smooth, lobulated surface; rarely bilateral.
- Cut surface: solid portions are granular, trabeculated, yellow or gray-yellow.
- Cystic areas with hemorrhage are common (spontaneous rupture can cause acute abdomen).
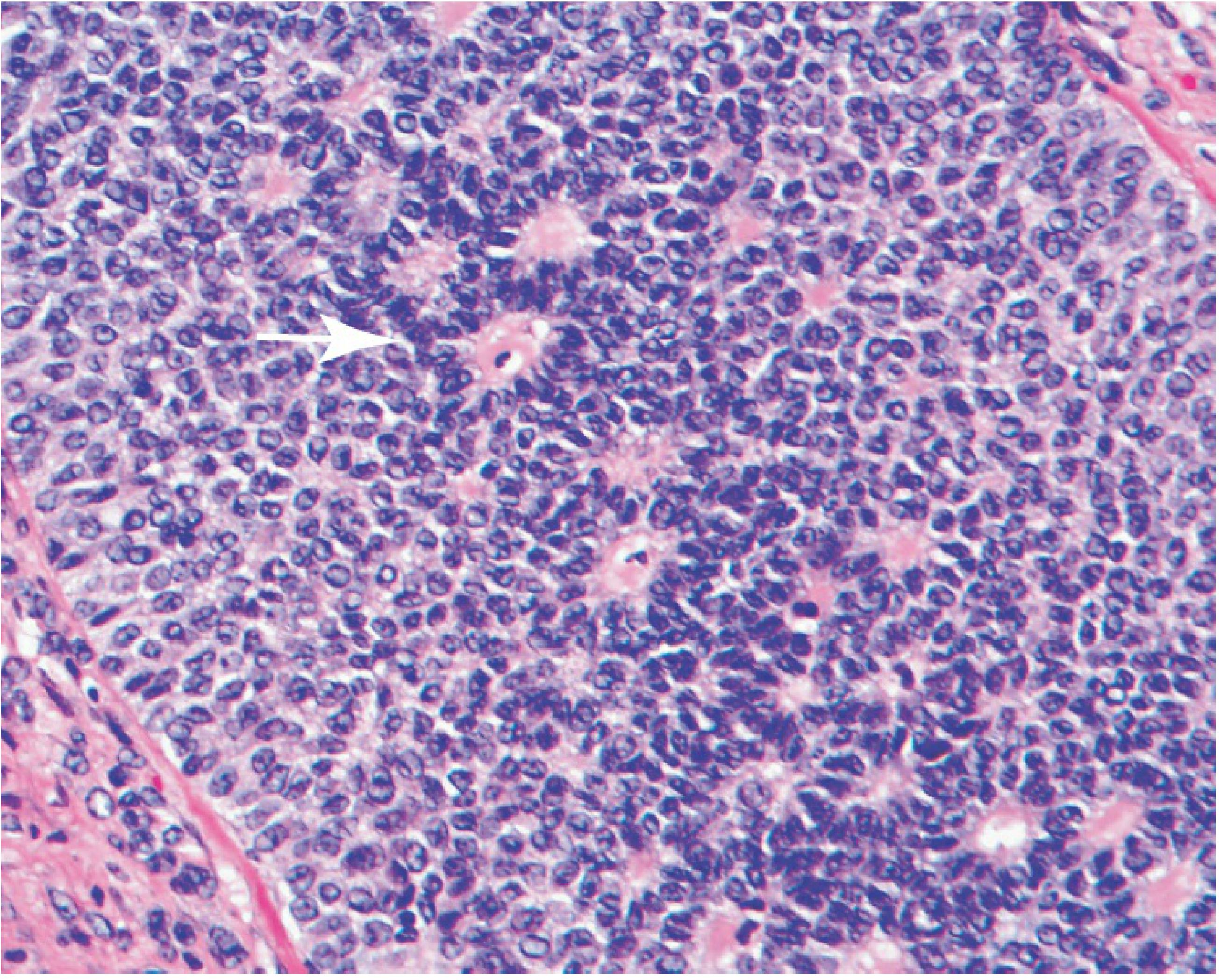
Microscopic Pathology
Adult GCT features:
- Cells are round/oval with scant cytoplasm.
- Nuclei: pale, finely granular chromatin with characteristic "coffee-bean" longitudinal nuclear grooves - pathognomonic.
- Mitotic figures may be present; numerous mitoses suggest poorly differentiated/sarcomatoid variant.
- Histological patterns (from well to poorly differentiated):
- Microfollicular (most common) - small clusters/rosettes around a central cavity
- Macrofollicular
- Trabecular/insular
- Solid-trabecular
- Diffuse/sarcomatoid (least differentiated, worst prognosis)
- Call-Exner bodies: small clusters of granulosa cells arranged around a central space filled with eosinophilic material resembling primordial follicles - pathognomonic of GCT.
Juvenile GCT features (contrast with adult):
- Rounder, more hyperchromatic nuclei (vs. pale grooved nuclei in AGCT)
- Numerous mitotic figures
- Large irregular follicle spaces - macrofollicular
- Luteinized cells common
- No FOXL2 mutation
Hormonal Activity and Clinical Features
- ~70% secrete estrogen or androgens.
- Inhibin (peptide hormone): secreted by granulosa cells; inhibin B more frequently elevated than inhibin A. Inhibin levels precede clinical recurrence by ~12 months - used as a tumor marker for monitoring.
- Anti-Mullerian Hormone (AMH): elevated in 75% preoperatively; >90% sensitivity for detecting recurrence.
- Estrogenic effects:
- Premenopausal: menstrual irregularities, secondary amenorrhea, cystic endometrial hyperplasia.
- Postmenopausal: abnormal uterine bleeding (most common presenting symptom).
- Endometrial hyperplasia in 25-50% of cases.
- Concurrent endometrial carcinoma in at least 5% - must always be excluded.
- In children: isosexual precocious puberty (JGCT).
Staging and Prognosis
- 90% present as stage I - excellent prognosis.
- 10-year survival ~90%; 20-year survival drops to 75%.
- Late recurrences 5 to 30 years after initial diagnosis are characteristic (hematogenous spread to lungs, liver, brain).
- DNA ploidy is an independent prognostic factor; diploid tumors have ~96% 10-year PFS.
- Poorly differentiated (diffuse/sarcomatoid) type has worse prognosis.
Treatment
- Surgery: Primary treatment. Unilateral salpingo-oophorectomy (USO) for stage IA in women of reproductive age (bilateral in only 2%). TAH+BSO for perimenopausal/postmenopausal women. Endometrial biopsy mandatory.
- Radiotherapy: No proven adjuvant role; pelvic irradiation may palliate isolated pelvic recurrences.
- Chemotherapy: BEP (Bleomycin-Etoposide-Cisplatin) or Carboplatin+Paclitaxel for stage III/IV or recurrent disease.
- Hormonal therapy: ~30% express estrogen receptors; nearly 100% express progesterone receptors. Progestins, GnRH agonists, and aromatase inhibitors used in recurrent/metastatic disease.
B. Thecoma
- Composed of theca cells; usually unilateral, solid, benign.
- Occur predominantly in postmenopausal women.
- Gross: firm, solid, yellow (due to lipid-rich theca cells).
- Micro: plump, lipid-laden spindle cells in sheets; reticulin fibres surround individual cells (unlike fibroma, where bundles are separated).
- Functionally active: secrete estrogens - cause endometrial hyperplasia and postmenopausal bleeding.
- Malignant thecoma is extremely rare; signs, management, and outcome similar to GCT.
C. Sertoli-Leydig Cell Tumors (Androblastoma)
Incidence
- Extremely rare: <0.2% of ovarian cancers.
- Peak incidence: third and fourth decades; 75% in women <40 years.
- Most are low-grade malignancies; poorly differentiated types behave more aggressively.
- Bilateral in <1% of cases.
Molecular Pathology
- Associated with somatic DICER1 gene mutations (also seen in pleuropulmonary blastoma and other pediatric tumors).
Gross Pathology
- Usually unilateral; small to medium-sized.
- Solid or lobulated; yellow-orange in color (due to Leydig cell lipid content).
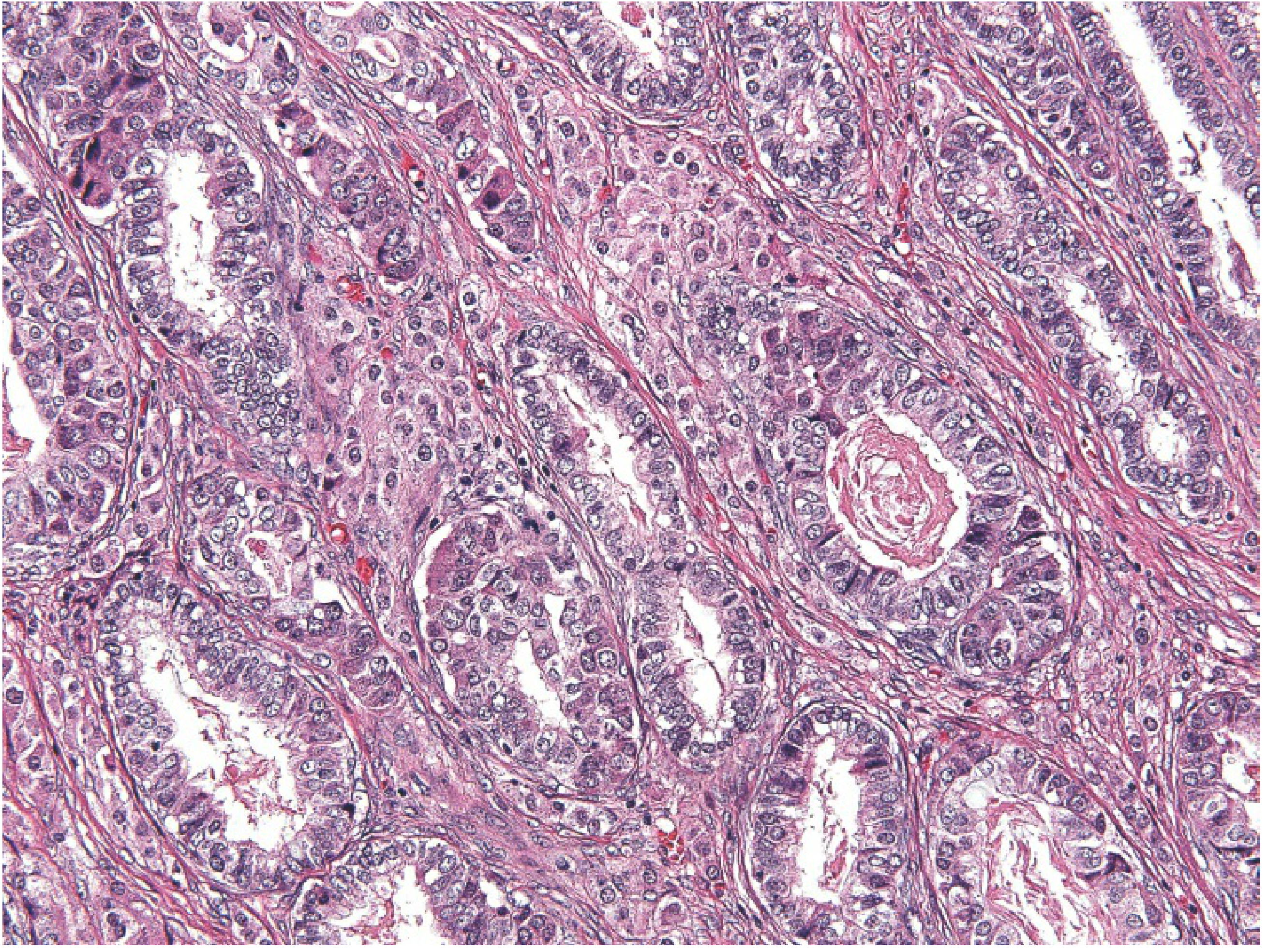
Microscopic Pathology
- Variable patterns depending on differentiation:
- Well-differentiated: Hollow or solid tubules lined by Sertoli cells with interstitial Leydig cells.
- Moderately differentiated: Immature sex cord elements + Leydig cells.
- Poorly differentiated (sarcomatoid): Spindle cells with primitive sex cord elements.
- With heterologous elements: Mucinous epithelium, cartilage, or skeletal muscle elements.
- Key feature: Leydig cells appear as aggregates of eosinophilic cells in the stroma adjacent to Sertoli cell tubules.
Hormonal Activity and Clinical Features
- Tumors typically produce androgens.
- Virilization in 70-85% of patients: oligomenorrhea → amenorrhea, breast atrophy, acne, hirsutism, clitoromegaly, voice deepening, receding hairline.
- Biochemistry: elevated testosterone and androstenedione; normal or mildly elevated DHEA-S.
- Rarely: estrogenic manifestations (isosexual precocity, irregular/postmenopausal bleeding).
Treatment and Prognosis
- Surgical: USO for young women (bilateral <1%); TAH+BSO for older patients.
- Chemotherapy (VAC regimen) and radiotherapy for persistent/metastatic disease (limited data).
- 5-year survival: 70-90%; recurrences after 5 years are uncommon.
- Prognosis worsens with poorly differentiated histology.
D. Steroid Cell Tumors
A group of uncommon tumors whose cells resemble steroid-secreting cells (lutein cells, Leydig cells, adrenal cortical cells):
| Type | Feature |
|---|---|
| Stromal luteoma | Small, benign; in postmenopausal stroma; may produce estrogens |
| Leydig cell / Hilus cell tumor | Small, benign; contain Reinke's crystalloids (pathognomonic); cause virilization |
| Steroid cell tumor, NOS | Larger; higher malignant potential; may secrete cortisol (Cushing's) |
E. Gynandroblastoma and SCTAT
- Gynandroblastoma: Rare; contains both granulosa-stromal and Sertoli-Leydig elements; may produce both estrogens and androgens.
- Sex cord tumor with annular tubules (SCTAT): Associated with Peutz-Jeghers syndrome (PJS) in ~30% of cases; contains ring-shaped tubules; may be bilateral and multifocal in PJS patients.
Immunohistochemistry Summary
| Marker | GCT | Sertoli-Leydig | Thecoma |
|---|---|---|---|
| Inhibin | + | + | + |
| Calretinin | + | + | + |
| SF-1 | + | + | + |
| FOXL2 (mutation) | + (AGCT) | - | - |
| EMA/CK | - | - | - |
Inhibin, calretinin, and SF-1 positivity with EMA/CK negativity help distinguish sex cord-stromal tumors from carcinomas - a critical diagnostic point.
Differential Diagnosis
| Tumor | Distinguishing Feature |
|---|---|
| Endometrioid carcinoma | EMA+, inhibin-, glandular pattern |
| Small cell carcinoma (hypercalcemic type) | SMARCA4 loss; young patients; hypercalcemia |
| Metastatic carcinoid | Clinical history; chromogranin+, inhibin- |
| Undifferentiated carcinoma | EMA+, CK+, inhibin- |
Key Exam Points (Quick Recall)
- Sex cord-stromal tumors = 5-8% of all ovarian malignancies.
- GCT = most common malignant sex cord-stromal tumor; FOXL2 mutation in 97% of AGCT.
- Call-Exner bodies + coffee-bean nuclei = GCT hallmarks.
- Inhibin and AMH are tumor markers for GCT.
- GCT: 90% stage I; late recurrences (up to 30 years) are characteristic.
- Sertoli-Leydig = androgenic; DICER1 mutation; virilization in 70-85%.
- Thecoma = benign, estrogenic, postmenopausal, yellow lipid-rich cells.
- Hilus cell tumor = Reinke's crystalloids; virilization.
- SCTAT + Peutz-Jeghers syndrome.
- IHC: inhibin+ / calretinin+ / EMA- distinguishes from carcinoma.
Sources: Berek & Novak's Gynecology (pp. 2398-2405); Robbins & Kumar Basic Pathology (Ovarian Tumors section); Schwartz's Principles of Surgery, 11e.
This is a shared conversation. Sign in to Orris to start your own chat.