Here is a detailed, fully illustrated guide to Floating Knee injury:
Floating Knee Injury - Comprehensive Overview
1. Definition
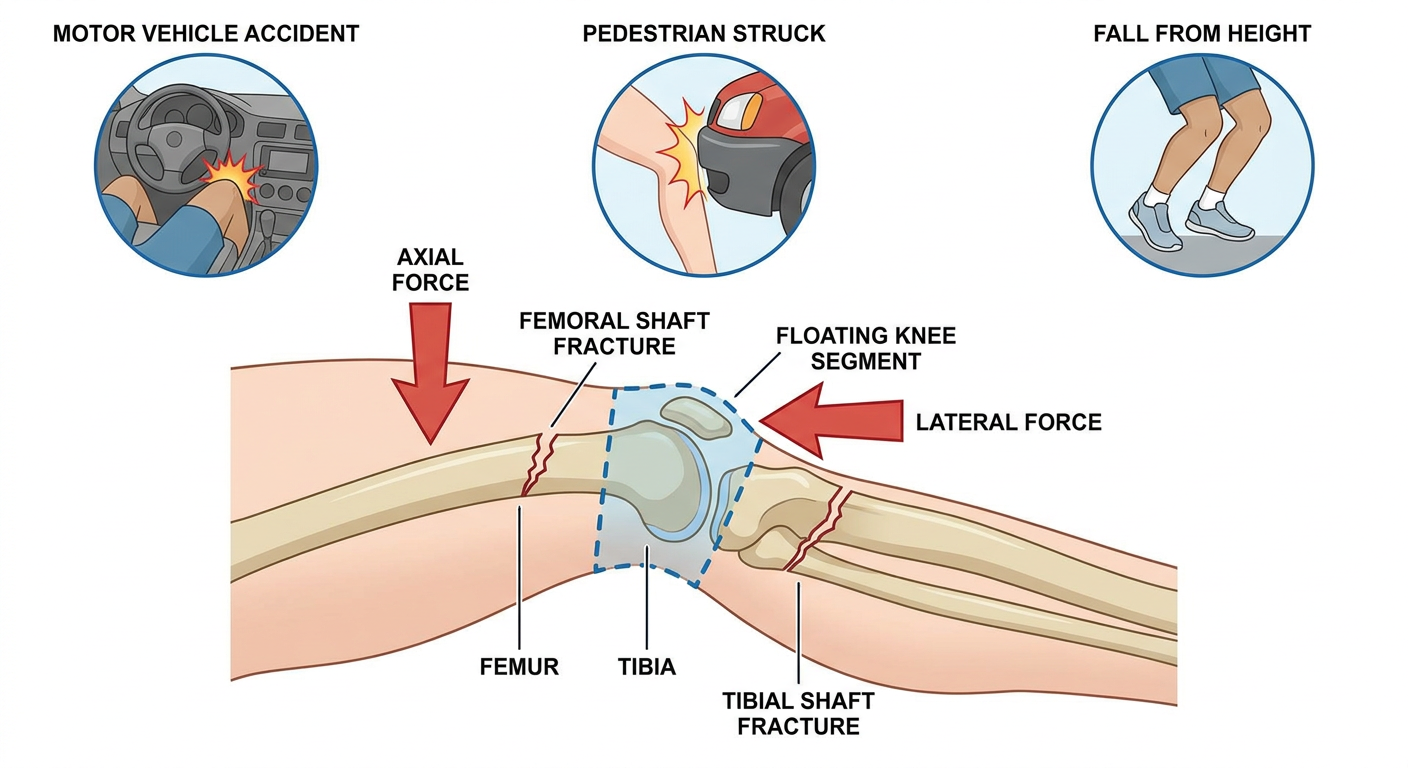
"Floating knee" describes the flail knee joint segment resulting from simultaneous fractures of the ipsilateral femur and tibia. The knee appears to "float" because it has lost its bony connections to both the proximal (pelvis/hip) and distal (ankle/foot) skeleton. This is also called a "flail knee" injury.
The knee joint itself is not necessarily fractured - the defining feature is fractures in BOTH long bones on the same side, isolating the knee segment.
- Campbell's Operative Orthopaedics 15th Ed 2026
2. Etiology
Floating knee is almost exclusively a high-energy polytrauma injury. The mean Injury Severity Score (ISS) is reported at >16.
Mechanisms of Injury
| Mechanism | Proportion |
|---|
| Road traffic accidents (RTA) | ~92-93% (most common) |
| Motorcycle/cyclist vs. auto | High proportion within RTA |
| Pedestrian vs. auto | Common |
| Falls from height | ~2-5% |
| Industrial/agricultural accidents | ~5-7% |
The typical scenario involves a bimodal force application: a direct axial force drives through the limb while a lateral or rotational force simultaneously fractures the second bone. In a dashboard injury, the flexed knee receives a posteriorly directed force that fractures the distal femur while the foot remains planted, fracturing the tibia.
Demographics
- Age: Most common in young adults (range 16-68 years, average ~29.6 years)
- Sex: Strong male predominance - M:F ratio approximately 7:1
- Pediatric floating knee injuries are uncommon and are classified separately (Letts-Vincent system)
3. Classification Systems
A. Blake and McBryde Classification (1975) - The Original
This was the first formal description (1975), classifying injuries based on the site of fracture in each bone:
- Type I: Fractures in both diaphyses (shaft-only fractures)
- Type II: At least one fracture involves the metaphysis or articular surface near the knee joint
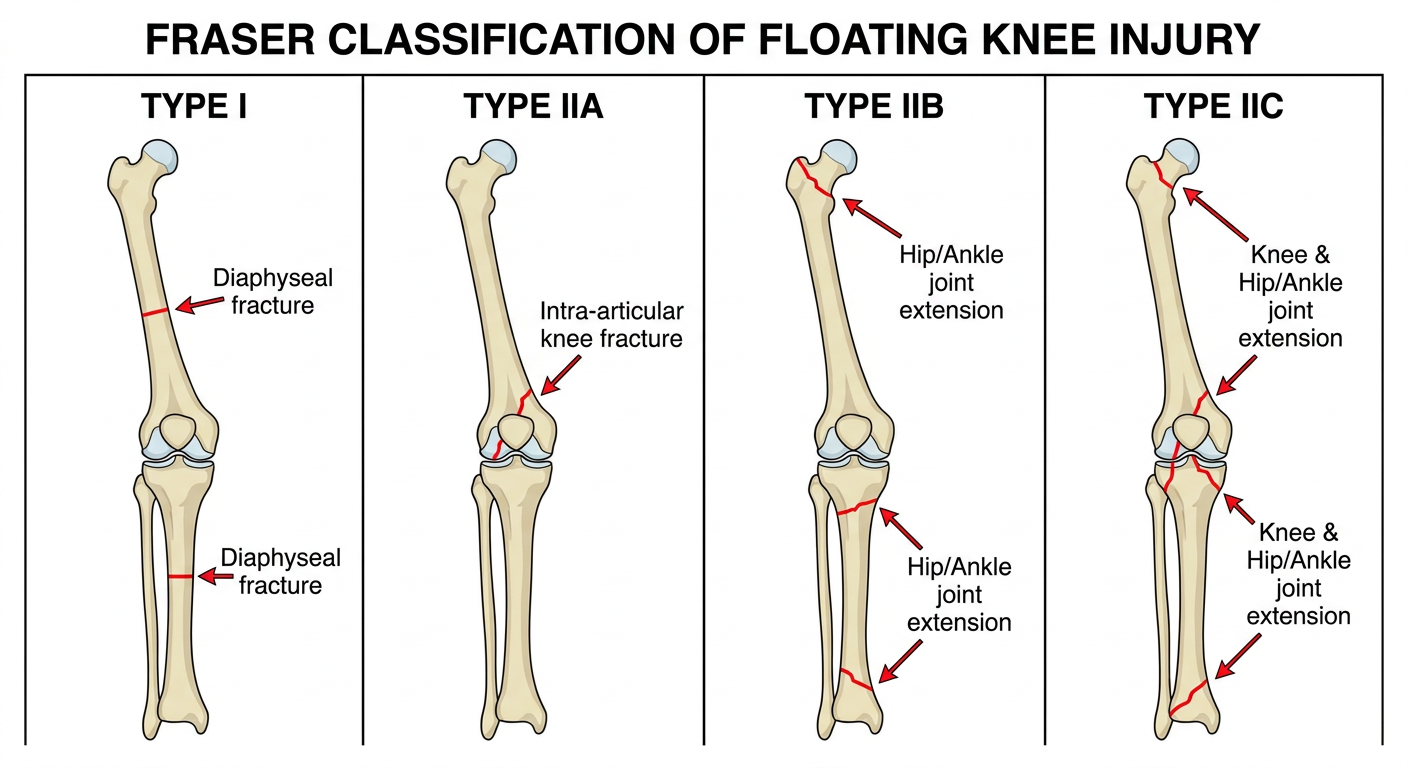
B. Fraser Classification (1978) - Most Widely Used
Fraser et al. further refined Type II into subtypes based on articular involvement. This remains the standard clinical classification:
| Type | Description | Key Features |
|---|
| Type I | Fractures of BOTH femoral and tibial diaphyses | Extra-articular; no joint involvement; best prognosis |
| Type IIA | One or both fractures involve the knee joint | Intra-articular at knee (distal femur or proximal tibia); worse prognosis |
| Type IIB | One fracture extends into hip or ankle joint | Proximal femur or distal tibia/fibula articular involvement |
| Type IIC | Fractures involve BOTH the knee AND another joint (hip or ankle) | Most severe; multiple articular surfaces; worst prognosis |
Type I is most common (~57%), followed by Type IIA (~18%), Type IIB (~15%), and Type IIC (~10%).
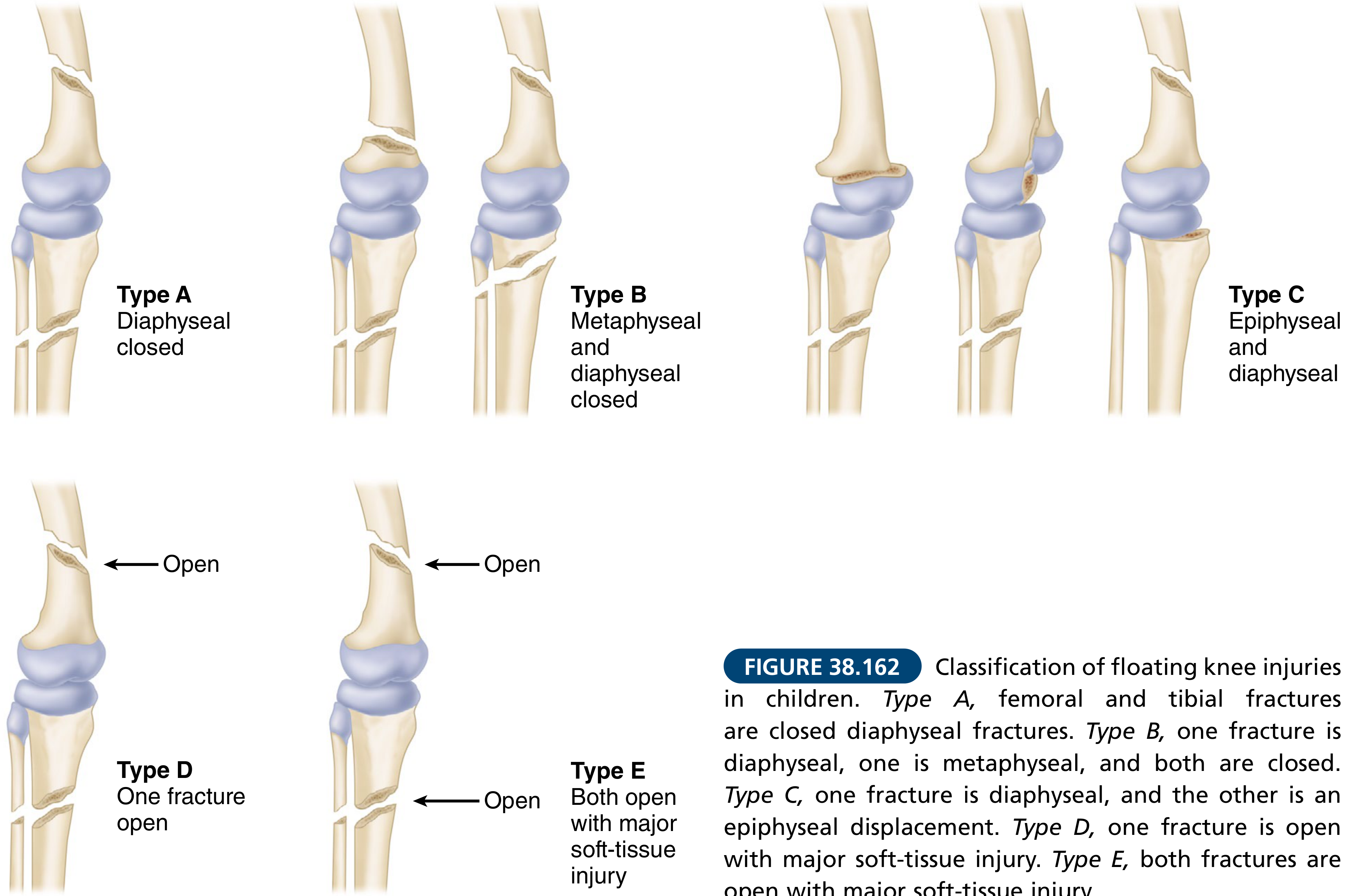
C. Letts-Vincent Classification (Pediatric)
Used for children. Classifies by fracture location AND open/closed status:
Classification of floating knee injuries in children. Type A: closed diaphyseal fractures in both bones. Type B: one diaphyseal, one metaphyseal - both closed. Type C: one diaphyseal, other epiphyseal displacement. Type D: one fracture open with major soft-tissue injury. Type E: both fractures open with major soft-tissue injury.
(Campbell's Operative Orthopaedics 15th Ed 2026, Fig. 38.162)
4. Mechanism of Injury (Biomechanics)
The floating knee arises from two simultaneous high-energy forces:
- Axial loading - compressive force transmitted through the limb (e.g., foot-pedal impact or fall landing)
- Bending/torsional force - lateral, rotational, or angular force creating fracture at a second level
The knee joint becomes the "isolated segment" between the two fracture sites. With both supporting bony columns disrupted, the knee has no structural stability - it can move abnormally in all planes (hence "floating").
Specific scenarios:
- Dashboard injury: Knee flexed at impact; the femur drives posteriorly (proximal fracture) while tibia resists at the ankle (distal fracture)
- Pedestrian impact: Direct blow to mid-femur + secondary tibial fracture from ground reaction force
- Motorcycle accident: High-speed rotational + axial forces fracturing both bones simultaneously
5. Associated Injuries
Floating knee is a marker of severe polytrauma. Associated injuries are divided into systemic and local.
Systemic (Life-Threatening) Injuries
| System | Injury | Approximate Rate |
|---|
| Head | Traumatic brain injury (TBI) | Common; may complicate anesthesia planning |
| Chest | Rib fractures, hemopneumothorax, pulmonary contusion | 41% (rib fractures) |
| Abdomen | Solid organ injury (liver, spleen) | Variable |
| Spine | Vertebral fractures | ~43% (highest associated injury) |
Local Limb Injuries
| Injury | Rate |
|---|
| Open fractures | 57-62% (very high) |
| Vascular injury (popliteal artery) | ~21% |
| Ligamentous instability (ACL, PCL, collaterals) | ~30% of cases |
| Compartment syndrome | Significant risk |
| Peroneal nerve injury | Variable |
| Meniscal tears | Associated with Type IIA |
| Fat embolism syndrome | Post-fracture complication |
| Deep vein thrombosis (DVT) | Post-stabilization risk |
Knee ligamentous instability is reported in almost one-third of cases. ACL/PCL injuries are often missed at initial presentation because examination is difficult with unstable fractures. - Rockwood and Green's Fractures in Adults 10th Ed 2025
6. Signs and Symptoms
History
- High-energy mechanism (RTA, fall from height)
- Severe pain in the thigh and leg
- Inability to bear weight
- May be unconscious or have altered sensorium (TBI)
Physical Examination
General:
- Signs of polytrauma/hemorrhagic shock (tachycardia, hypotension)
- Signs of head injury
Local examination:
| Finding | Significance |
|---|
| Gross deformity, shortening, angulation of thigh and leg | Fracture displacement |
| Abnormal mobility of the knee in all planes - the "floating" sign | Pathognomonic |
| Swelling, bruising, ecchymosis over thigh and leg | Hematoma formation |
| Tenderness over fracture sites | |
| Absent or diminished pulses (popliteal, dorsalis pedis) | Vascular injury - emergency |
| Skin wounds, exposed bone | Open fracture (high rate ~57-62%) |
| Tense compartments in thigh or leg | Compartment syndrome |
| Paresthesia/weakness in foot | Peroneal or tibial nerve injury |
| Knee ligament laxity (Lachman, varus/valgus stress) | May be masked by fracture instability |
The "Floating" Sign: When the limb is lifted at the foot, the entire knee segment moves independently of both the thigh and leg - the most characteristic clinical finding.
7. Investigations
Primary Survey
- ATLS protocol: Airway, Breathing, Circulation
- Hemorrhagic shock assessment
Imaging
Plain Radiographs (First Line)
- Minimum: AP and lateral views of the entire femur and tibia including hip and knee and ankle joints
- Must image the joint above and below each fracture
- Identifies fracture level, pattern, displacement, and any intra-articular extension
CT Scan
- Mandatory for intra-articular fractures (Type II Fraser)
- Tibial plateau, distal femur, pilon fractures need CT for surgical planning
- CT angiography if vascular injury suspected
MRI
- For ligamentous injuries (ACL, PCL, menisci) - usually deferred until after fracture stabilization
- Useful in pre-operative planning for Type IIA
Vascular Studies
- Ankle-brachial index (ABI): ABI <0.9 warrants CT angiography or formal angiography
- Popliteal artery injury (21% rate) is a surgical emergency
Laboratory
- FBC, coagulation profile, group and crossmatch
- Metabolic panel (renal function, electrolytes)
- Blood gas (lactic acidosis indicating shock)
- Injury Severity Score (ISS) calculation
8. Treatment
Treatment Goals
- Life-saving resuscitation (ATLS priority)
- Restore vascular supply if compromised
- Stabilize fractures to control hemorrhage and pain
- Prevent complications (compartment syndrome, infection, DVT)
- Restore limb alignment and joint function
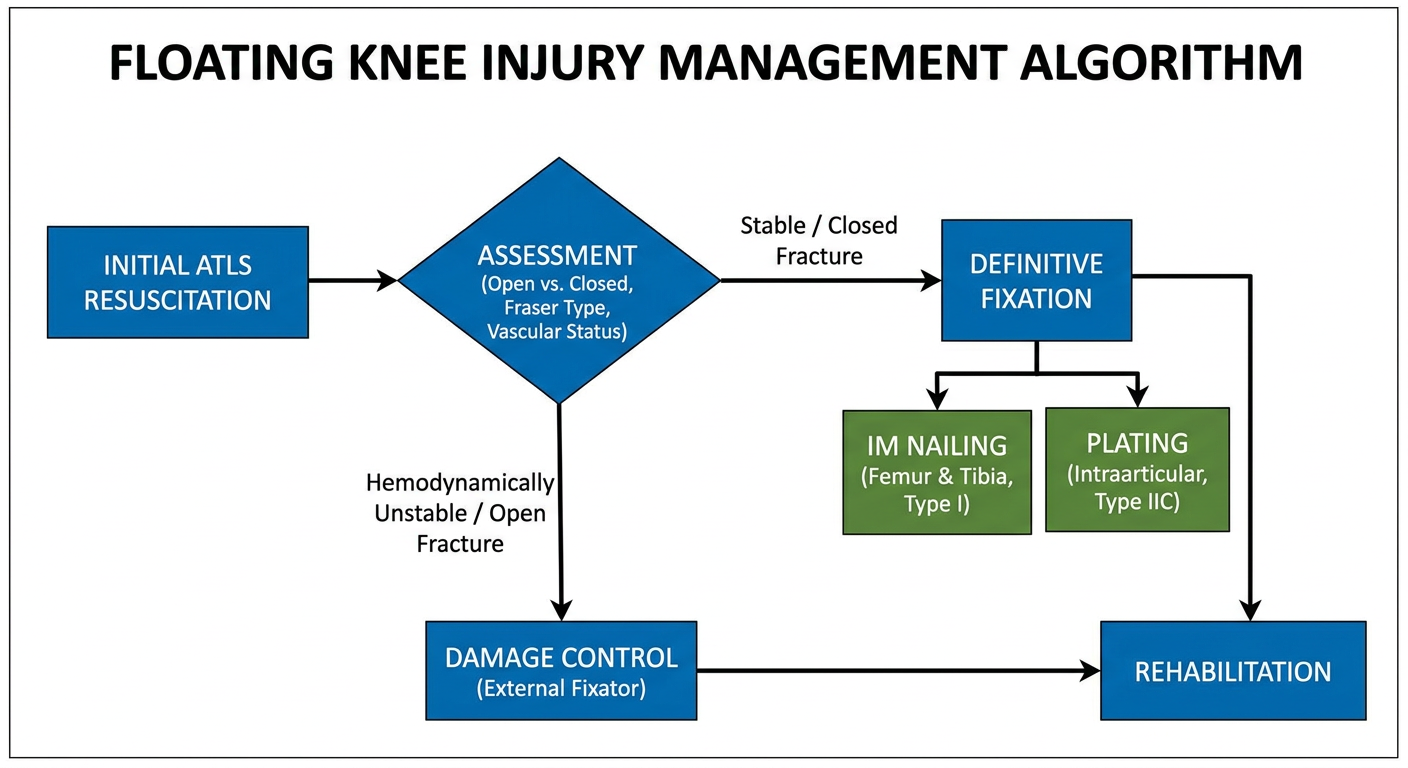
Phase 1: Emergency/Initial Management (Damage Control Orthopaedics)
In hemodynamically unstable patients or those with open fractures and severe soft-tissue injury:
Damage Control Orthopaedics (DCO):
- Temporary external fixation of both femur and tibia
- Controls hemorrhage and pain
- Allows ICU resuscitation and management of systemic injuries
- Planned conversion to definitive fixation at 5-10 days (average 8.7 days in studies)
Vascular emergencies:
- Popliteal artery injury requires urgent surgical repair or bypass
- Fasciotomy for compartment syndrome (4-compartment leg decompression)
Phase 2: Definitive Surgical Fixation
Fraser Type I (Diaphyseal, Extra-Articular) - Gold Standard Treatment
Simultaneous Intramedullary (IM) Nailing of Both Bones - preferred method
| Aspect | Detail |
|---|
| Femur | Antegrade femoral IM nail (preferred) or retrograde femoral nail |
| Tibia | Antegrade tibial IM nail |
| Retrograde femoral nail advantage | Allows fixation of both bones through same anterior knee approach |
| Result | Good to excellent results achieved in majority of patients |
- Rockwood and Green's 10th Ed 2025: "Good to excellent results can be achieved when both fractures are treated with IM nailing."
Fraser Type IIA (Intra-articular at Knee)
- Plating preferred for intra-articular femoral condyle or tibial plateau fractures
- Allows simultaneous management of associated soft tissue injuries (meniscal tears)
- Locking plates (MIPO technique - Minimally Invasive Plate Osteosynthesis) increasingly used
- IM nail may still be used for diaphyseal component; articular fracture addressed with screws/plate
Fraser Type IIB/IIC (Multiple Articular Involvement)
- Most complex; requires individualized surgical planning
- Combination of IM nailing + plating
- May require staged procedures
- Highest complication rate; poorest prognosis
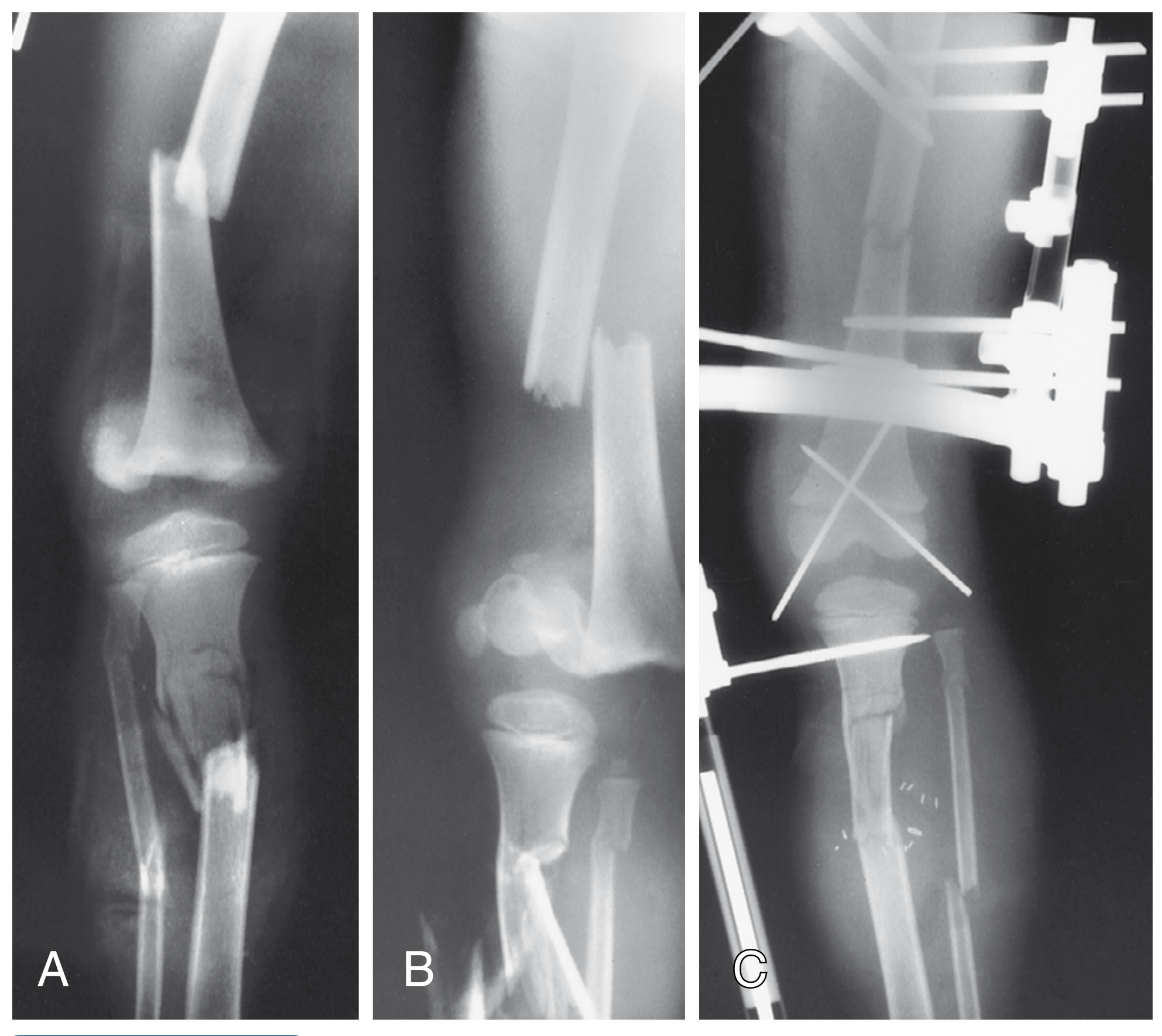
Radiograph: Floating Knee with External Fixation and Fixation
A: AP radiograph showing ipsilateral femoral and tibial fractures (floating knee). B: Lateral view. C: Post-operative with external fixator applied for damage control.
(Campbell's Operative Orthopaedics 15th Ed 2026)
Non-Operative Treatment
- Reserved for children <10 years with closed Type A fractures (Letts-Vincent)
- Traction + cast immobilization
- Contraindicated in adults - high complication rate
Phase 3: Wound Management (Open Fractures)
57-62% of floating knees are open fractures. Management follows:
- Emergency debridement and irrigation within 6-8 hours (sooner for contaminated wounds)
- Temporary external fixation (Gustilo-Anderson classification guides urgency)
- Wound closure/coverage - primary closure if clean; delayed primary closure or flap coverage for contaminated/degloving injuries
- Antibiotics - first-generation cephalosporin ± aminoglycoside ± penicillin (soil contamination)
Phase 4: Rehabilitation
- Early weight bearing as tolerated after stable fixation
- Physiotherapy for knee range of motion
- Management of ligamentous injuries (ACL/PCL reconstruction) typically deferred 6-8 weeks post-fracture stabilization
- DVT prophylaxis (LMWH)
- Continuous monitoring for non-union, malunion, infection
9. Complications
Early
- Hemorrhagic shock
- Popliteal artery injury (21%)
- Compartment syndrome
- Fat embolism
- Sepsis (open fractures)
- Pulmonary embolism
Late
| Complication | Notes |
|---|
| Limb-length discrepancy | Especially in children (growth disturbance) |
| Angular deformity/malunion | Malalignment of femur or tibia |
| Knee instability | Unrecognized ligamentous injury |
| Stiffness | Knee or ankle range-of-motion loss |
| Non-union | Higher risk with open fractures/infection |
| Osteomyelitis | Especially in open fractures |
| Amputation | In severe vascular injury or osteomyelitis |
| DVT/PE | |
| Post-traumatic arthritis | With intra-articular involvement |
10. Prognosis
- Fraser Type I (IM nailing): Good to excellent results in majority of patients
- Fraser Type II: Significantly worse; intra-articular involvement (especially IIC) carries highest complication rate
- Pediatric (<10 years): 93% good-to-excellent results with modern fixation
- Pediatric (>10 years): Higher complication rate; up to 50% poor results historically (limb-length discrepancy, angular deformity, ligamentous instability)
- Risk factors for poor outcome: intra-articular involvement, severe open tibia fracture, vascular injury, age >60 years
Summary Table
| Feature | Detail |
|---|
| Definition | Ipsilateral femur + tibia fractures → "floating" knee segment |
| Most common cause | RTA (~93%) |
| Key classification | Fraser (adults): Type I, IIA, IIB, IIC |
| Most common type | Fraser Type I (~57%) |
| Worst prognosis | Fraser Type IIC |
| Open fracture rate | 57-62% |
| Vascular injury rate | 21% |
| Ligamentous injury rate | ~30% |
| Gold standard treatment | Simultaneous IM nailing of both bones |
| Pediatric treatment | External fixation → IM nail or plate; conservative <10 yrs |
Sources:
- Campbell's Operative Orthopaedics 15th Ed 2026
- Rockwood and Green's Fractures in Adults 10th Ed 2025
- Fraser RD, Hunter GA, Waddell JP. Ipsilateral fracture of the femur and tibia. J Bone Joint Surg Br. 1978
- StatPearls: Floating Knee (NBK537096)
- Open Orthopaedics Journal: Management of the Floating Knee in Polytrauma Patients