Why their is stooping in Parkinson’s and frontal gaits
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
I now have comprehensive material from the textbooks. Let me compile the full answer.
Stooped Posture in Parkinson's Disease
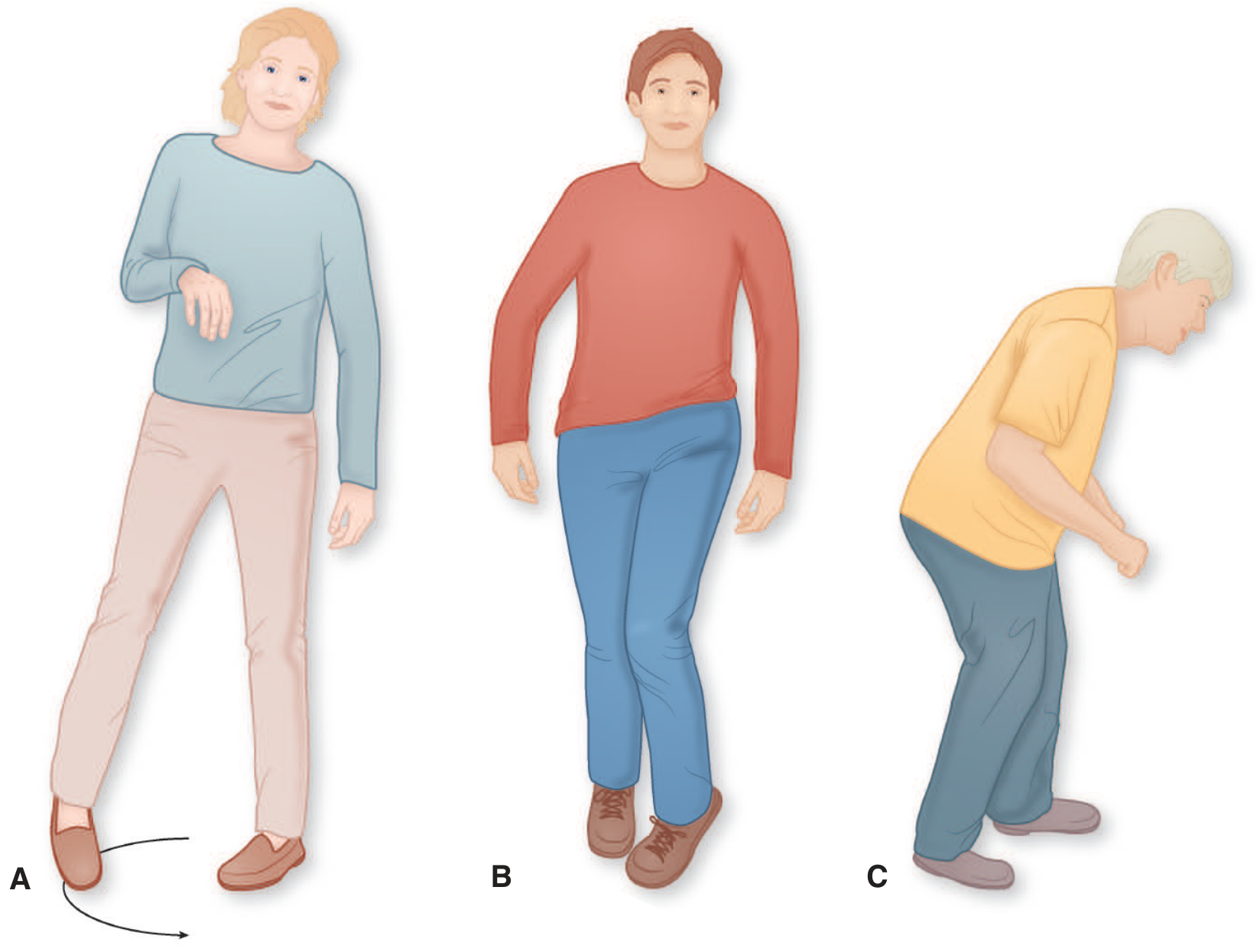
Figure 6-2C (Adams & Victor): Parkinsonian gait with forward position of the upper torso, flexion of the neck and elbows, and short-stepped shuffling gait.
Why Does Stooping Occur in Parkinson's?
Stooping (forward flexed posture) in Parkinson's disease (PD) results from a combination of several interrelated mechanisms:
1. Basal Ganglia Dysfunction - Loss of Postural Tone Regulation
The basal ganglia (specifically the dopamine-depleted substantia nigra pars compacta projecting to the striatum) normally regulate postural tone and the automatic maintenance of an upright stance. With dopamine deficiency:
- Righting reflexes fail - the normal ability to auto-correct posture against gravity is impaired
- General attitude of flexion develops across the whole body (neck, trunk, elbows, knees)
- The person cannot generate adequate extensor postural tone to keep the trunk upright
2. Rigidity Predominantly Affecting Flexors
Parkinsonian rigidity (lead-pipe or cogwheel) tends to be more pronounced in flexor muscle groups than extensors. This muscular imbalance progressively pulls the trunk forward and flexes the neck and limbs.
3. Faulty Postural Responses
As Adams & Victor's states: "With disorders of the basal ganglia, the posture of the body and the postural responses to perturbations in equilibrium are faulty." When the body deviates even slightly forward, corrective righting reflexes that would normally bring the trunk back to vertical are insufficient. The patient, instead of correcting, continues to lean further forward.
4. How Stooping Leads to Festination
The stooped trunk shifts the center of gravity forward. Once walking begins, the upper body advances ahead of the lower limbs, and to prevent falling:
- Steps become increasingly rapid and short (festination - from Latin festinare, "to hasten")
- The patient may break into a near-run, unable to stop, risking collisions or falls
- The arms are carried flexed and ahead, with absent arm swing
- The legs are stiff and bent, barely clearing the floor (shuffling)
In summary for PD: stooping = dopamine deficiency → failed basal ganglia postural control → flexion attitude → impaired righting reflexes → forward center of gravity shift → festinating shuffling gait.
Stooping in Frontal Gait (Frontal Lobe Disorder of Gait)
Frontal gait - also called "frontal lobe apraxia of gait," "marche à petit pas," or "magnetic gait" - produces a different but superficially similar picture.
Why Stooping / Flexed Posture Occurs Here
1. Disruption of Cortical-Basal Ganglionic Integration
Frontal gait arises from disease of the medial frontal lobes and their connections with the basal ganglia. This severs the cortical integration of the essential elements of stance and locomotion that are acquired in infancy. As Adams & Victor states, it is not a true apraxia (walking is instinctual, not a learned skill) but rather a "loss of integration at the cortical and basal ganglionic levels" of stance and locomotion.
2. Classic Posture
- Patients assume a posture of slight flexion with feet placed wider than normal (to compensate for instability)
- Steps are small, shuffling, and hesitant - identical in appearance to lower-half parkinsonism
- Arm swing may be preserved (key differentiator from PD), helping distinguish the two
3. Progressive Loss of Gait Initiation
The disorder progresses:
- Early: Difficulty initiating, hesitation at doorways ("gait ignition failure")
- Intermediate: Short shuffling steps, turning requires many tiny pivot steps, needs support from walls or companions
- Advanced: Feet appear "glued to the floor" (magnetic gait) - patients can lift heels but toes seem to grab the floor; they can still move legs voluntarily (draw figures with feet, do heel-shin test) but cannot walk
- End-stage: Falls backward helplessly; eventually cannot stand or even sit unsupported
4. Underlying Lesions
Causes include:
- Bilateral medial frontal cortex dysfunction (most common mechanism)
- Subcortical white matter ischemia (Binswanger disease / "arteriosclerotic parkinsonism")
- Normal pressure hydrocephalus (NPH)
- Large frontal neoplasms (meningioma, glioma)
- Alzheimer disease (advanced)
Key Differences Between Parkinson's Stooping vs. Frontal Gait Stooping
| Feature | Parkinson's Gait | Frontal Gait |
|---|---|---|
| Arm swing | Absent/reduced | Often preserved |
| Upper limb signs | Tremor, rigidity, bradykinesia | Usually absent |
| Stooping cause | Dopamine loss, flexor rigidity | Medial frontal-basal ganglionic disconnection |
| Festination | Present (classic) | Absent or minimal |
| "Feet glued" | Can occur (freezing) | Prominent (magnetic gait) |
| Improvement with cues | Sometimes | Often improves with external cadence |
| Response to levodopa | Yes (idiopathic PD) | Minimal or absent |
| Associated cognitive changes | Late in PD | Often early dementia |
| Cause | Substantia nigra degeneration | Frontal/white matter pathology |
Sources: Adams and Victor's Principles of Neurology, 12th Edition, pp. 137-142; Localization in Clinical Neurology, 8e, p. 59-61.
Clock drawing in neurology dementia case with its interpretation and importance
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
I now have a real clinical clock drawing from a patient with right parietal infarction showing left-sided neglect, plus rich textbook content. Let me compile the comprehensive answer.
Clock Drawing Test (CDT) in Neurology and Dementia
What Is the Clock Drawing Test?
The Clock Drawing Test (CDT) is one of the most widely used bedside cognitive screening tools in neurology. The patient is asked to:
- Draw a circle (the clock face)
- Fill in all 12 numbers in their correct positions
- Draw hands to show a specified time - classically "10 past 11" (or "11:10")
It takes less than 2 minutes to administer and requires no equipment other than paper and a pen.
Why is the CDT Clinically Important?
The CDT is not a test of memory - it is a window into multiple cognitive domains simultaneously:
| Cognitive Domain Tested | What the Task Requires |
|---|---|
| Executive function | Planning, organizing, and sequencing a complex task |
| Visuospatial ability | Correctly spacing numbers around a circle |
| Semantic memory | Knowing what a clock looks like |
| Abstract thinking | Converting a verbal time command ("10 past 11") into a visual representation |
| Attention / concentration | Sustaining effort through the task |
| Constructional praxis | Motor coordination to draw the figure accurately |
| Hemineglect | Whether one side of the clock face is ignored |
As Kaplan & Sadock's notes: "The MMSE has limitations in evaluating executive function. The Clock Drawing Test can be used instead to evaluate executive function."
Neuroanatomical Basis of CDT Errors
The CDT is sensitive because it requires the integrated function of multiple cortical regions:
- Right parietal lobe - visuospatial organization and spatial layout of numbers
- Left parietal lobe - praxis (knowing how to draw, use tools), calculation (placing numbers correctly)
- Frontal lobes - executive planning, sequencing, inhibiting the "pull" to write 10 and 11 as hands (executive error)
- Temporal lobe - semantic knowledge of what a clock looks like
A Real Clinical Example
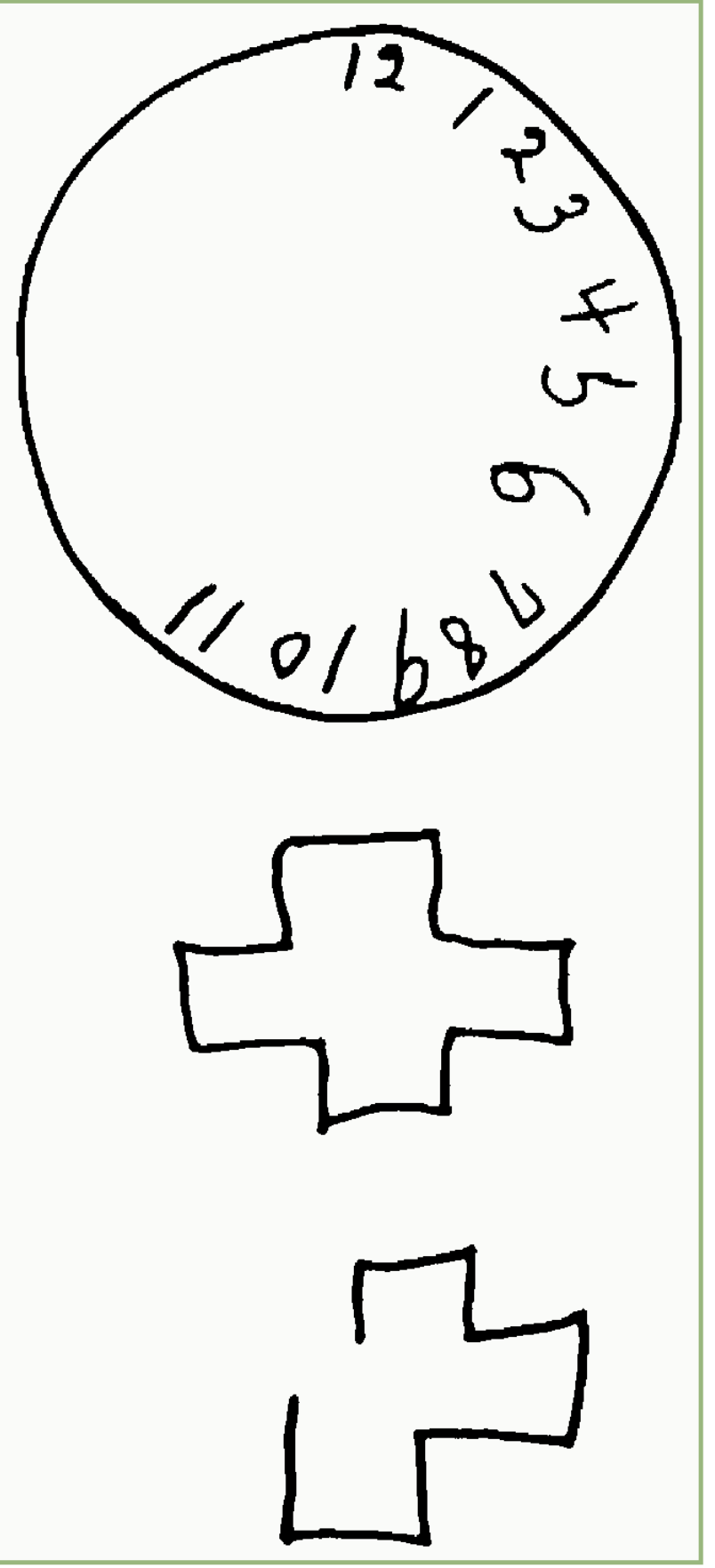
Fig. 7.3 from Bradley and Daroff's Neurology in Clinical Practice: Spontaneous clock drawing and copying of a cross by a patient with a RIGHT parietal infarction. The patient had only mild hemiparesis but dense left hemianopia and left-sided neglect. Notice: ALL numbers (12 through 11) are crowded into the right half of the clock face - the left side is completely empty. The cross copy below also shows the same left hemineglect - the right-sided elements are intact but the left arm of the cross is omitted or distorted.
Interpreting CDT Errors - What Each Error Tells You
1. Visuospatial Errors (Right Parietal Lesion / Alzheimer's)
- Numbers placed asymmetrically or bunched together
- Numbers placed outside the circle
- Poor spacing ("12, 1, 2, 3" all in the top right)
- The clock circle itself is distorted
2. Hemispatial Neglect (Right Parietal / Right Hemisphere Stroke)
- All numbers crowded into one half (as in the clinical image above)
- The left half is blank or has only a few numbers
- Hands drawn only to the right side
3. Executive / Frontal Errors
- "10 after 11" error - the most classic frontal error: instead of drawing the minute hand to the "2" (which represents 10 minutes), the patient writes the numeral "10" next to the "11" on the clock face, because the literal numbers 10 and 11 are "pulled" by the verbal instruction. This is a stimulus-bound response failure (loss of abstract set)
- Perseveration - repeating numbers beyond 12
- Starting over multiple times
- Inability to initiate the task at all
4. Memory / Semantic Errors (Moderate-Severe Dementia)
- Drawing something that does not resemble a clock at all
- Placing non-clock content inside the circle
- Blank face - patient cannot access the semantic concept of a clock
Scoring Systems
Several scoring systems exist; the most widely used clinically is the Mini-Cog scoring (used in the Mini-Cog rapid screen):
| Score | Criteria |
|---|---|
| 2 points (Normal) | All numbers placed in correct sequence and approximately correct position (12, 3, 6, 9 in anchor positions); no missing or duplicate numbers; hands pointing to 11 and 2 (showing 11:10) |
| 0 points (Abnormal) | Any significant error in number placement OR inability/refusal to draw the clock |
Note: Hand length is NOT scored in the Mini-Cog system.
In the Mini-Cog total score (0-5 points):
- Clock Draw: 0 or 2 points
- Three-word recall: 0-3 points
- Cut-off of <3 is validated for dementia screening
- Cut-off of <4 is used when greater sensitivity is needed
CDT in Specific Dementia Types
| Dementia Type | Typical CDT Error Pattern |
|---|---|
| Alzheimer's disease (early) | Mild visuospatial errors; numbers slightly misplaced; hands may be wrong |
| Alzheimer's (moderate) | Numbers crowded, misplaced; hands absent or wrong; clock face distorted |
| Vascular dementia / Frontal | Executive errors prominent; "10/11 literal pull" error; perseveration |
| Right hemisphere stroke | Left hemineglect - all numbers in right half of face |
| Lewy body dementia | Severe visuospatial errors early (even before memory problems) |
| Frontotemporal dementia | Executive errors; perseveration; stimulus-bound responses |
| Normal aging | Clock generally intact; minor spacing issues only |
CDT vs. Other Screening Tools
| Tool | Time | Executive Function | Memory | Visuospatial | Overall Sensitivity for MCI |
|---|---|---|---|---|---|
| MMSE | ~10 min | Poor | Moderate | Limited | Lower (misses MCI) |
| MoCA | ~10 min | Good | Good | Good | Higher (better for MCI) |
| CDT alone | 1-2 min | Good | No | Good | Moderate |
| Mini-Cog (CDT + 3-word recall) | ~3 min | Moderate | Good | Moderate | Good for rapid screening |
As Adams & Victor states: the CDT is one of the "visual-spatial-constructional tasks" that forms an integral part of the bedside neurological mental status examination, alongside line bisection, cube copying, and intersecting pentagons - because it localizes lesions affecting higher cortical functions, just as motor examination localizes pyramidal lesions.
Key Teaching Points for a Dementia Case
- The CDT is not just a memory test - it tests executive function, visuospatial ability, and praxis simultaneously
- A normal MMSE does NOT rule out early dementia - the CDT catches executive and visuospatial deficits that MMSE misses
- The "10 past 11" time instruction is specifically chosen because it exploits a common executive error: the patient may be "pulled" by the numbers 10 and 11 in the instruction
- Hemineglect produces a characteristic pattern: all numbers crowded to one side - a right hemisphere (usually right parietal) lesion
- In Lewy body dementia, CDT errors may appear early when memory is still relatively intact - it is one of the features supporting the diagnosis
- The CDT must be interpreted in context of education and handedness
Sources: Bradley and Daroff's Neurology in Clinical Practice, p. 3095-3100; Adams and Victor's Principles of Neurology, 12th Edition, p. 488; Kaplan & Sadock's Comprehensive Textbook of Psychiatry, p. 12501; Morgan and Mikhail's Clinical Anesthesiology, 7e, p. 1731-1732.
This is a shared conversation. Sign in to Orris to start your own chat.