Pathology and medicine combined in exam preparation on cardiovascular system. Make simple pattern combo crush it..made easy memory aids , flow chart in pathophysiology..
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Excellent! I have all the key content and diagrams. Now let me compile the full cardiovascular exam prep guide.
🫀 CARDIOVASCULAR SYSTEM - EXAM CRUSH GUIDE
Pathology + Medicine Combined | Pattern-Based Memory Aids + Flowcharts
🗺️ THE BIG PICTURE MAP (Start Here)
RISK FACTORS
(HTN, DM, Smoking, Hyperlipidemia, Family Hx)
↓
ATHEROSCLEROSIS
(Endothelial Injury → Foam Cells → Plaque)
↓
┌─────────┬──────────┬─────────┐
↓ ↓ ↓ ↓
IHD STROKE PAD ANEURYSM
(angina,MI) (TIA,CVA) (claudication) (aorta)
↓
MYOCARDIAL INFARCTION
↓
HEART FAILURE / ARRHYTHMIAS / SUDDEN DEATH
⚡ MODULE 1 — ATHEROSCLEROSIS
Pathophysiology Flowchart (Robbins Basic Pathology)
ENDOTHELIAL INJURY (HTN, oxidized LDL, smoking, toxins)
↓
Increased permeability → LDL enters intima
↓
Monocytes migrate in → become MACROPHAGES
↓
Macrophages engulf oxidized LDL → FOAM CELLS
↓
Fatty streak (earliest visible lesion — reversible)
↓
SMC migration from media → Intima
SMC proliferation + ECM synthesis
↓
FIBROUS PLAQUE (lipid core + fibrous cap)
↓
Calcification, Necrosis, Inflammation
↓
COMPLICATED PLAQUE
├── Stable: gradual stenosis → Stable angina
└── Unstable: PLAQUE RUPTURE → Thrombosis → ACS/MI
Memory Aid - "FOAM":
Fatty streak → Oxidized LDL eaten → Atheroma forms → Macrophages become foam cells
Key Exam Facts:
- Plaque rupture (NOT stenosis) = most common cause of MI
- Fibrous cap is thin at shoulder regions = rupture-prone
- Stable plaque = thick cap, calcified, less lipid
- Vulnerable plaque = thin cap, large lipid core, lots of macrophages
❤️ MODULE 2 — CARDIAC HYPERTROPHY → HEART FAILURE
Pathophysiology Flowchart (Robbins Cotran & Kumar)
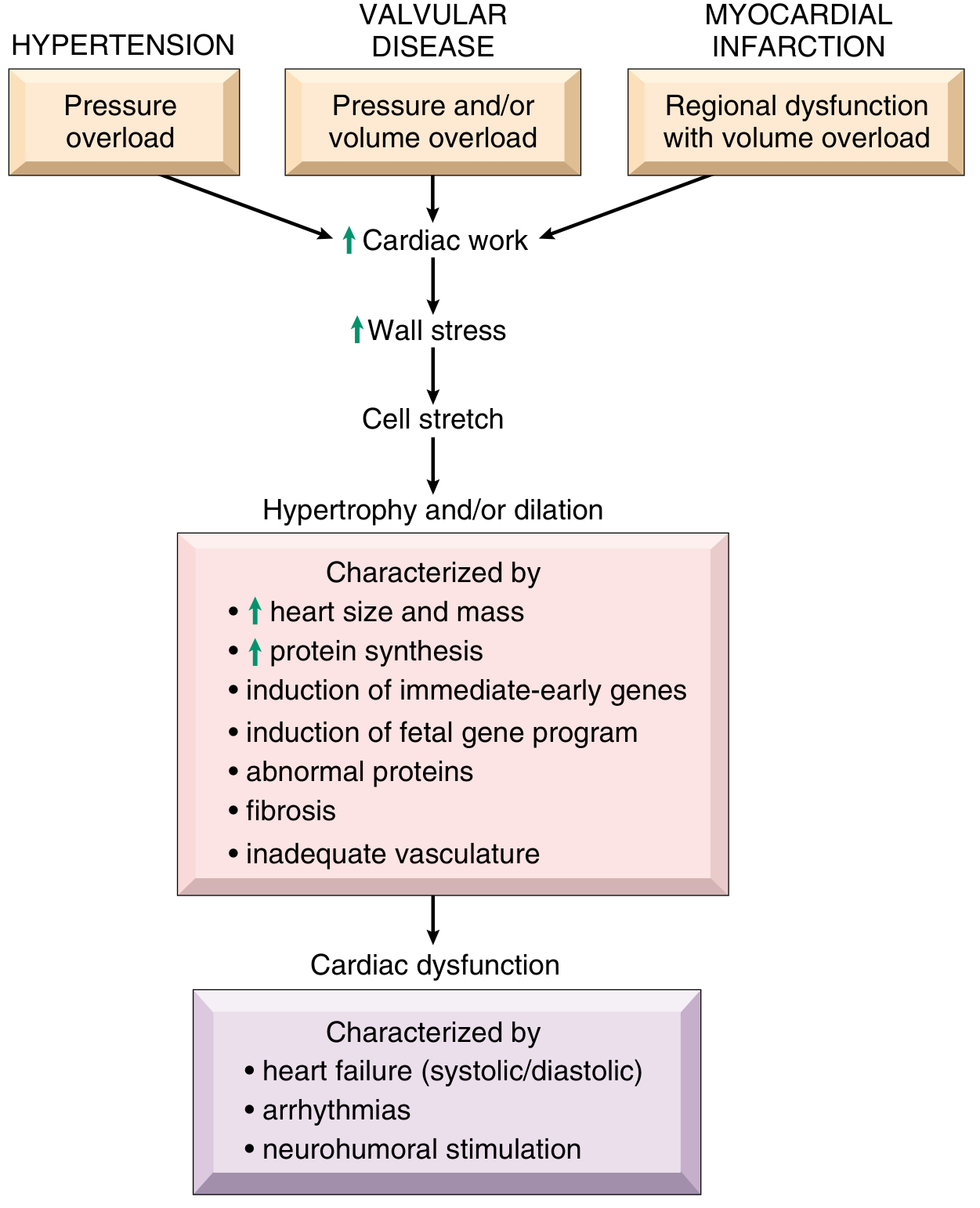
Pattern Memory - "PVC" Types of Hypertrophy:
| Type | Cause | Pattern | Shape |
|---|---|---|---|
| Pressure overload | HTN, Aortic Stenosis | Sarcomeres in PARALLEL | Concentric (thick wall) |
| Volume overload | AR, MR, VSD | Sarcomeres in SERIES | Eccentric (dilated) |
| Cardiomyopathy (HCM) | Genetic (MYH7) | Asymmetric septal | Outflow obstruction |
Mnemonic: "Parallel = Pressure = Plump walls"
Mnemonic: "Series = Stretch = Saggy dilated"
🔄 MODULE 3 — HEART FAILURE VICIOUS CYCLE
Compensatory Response Flowchart (Katzung Pharmacology)
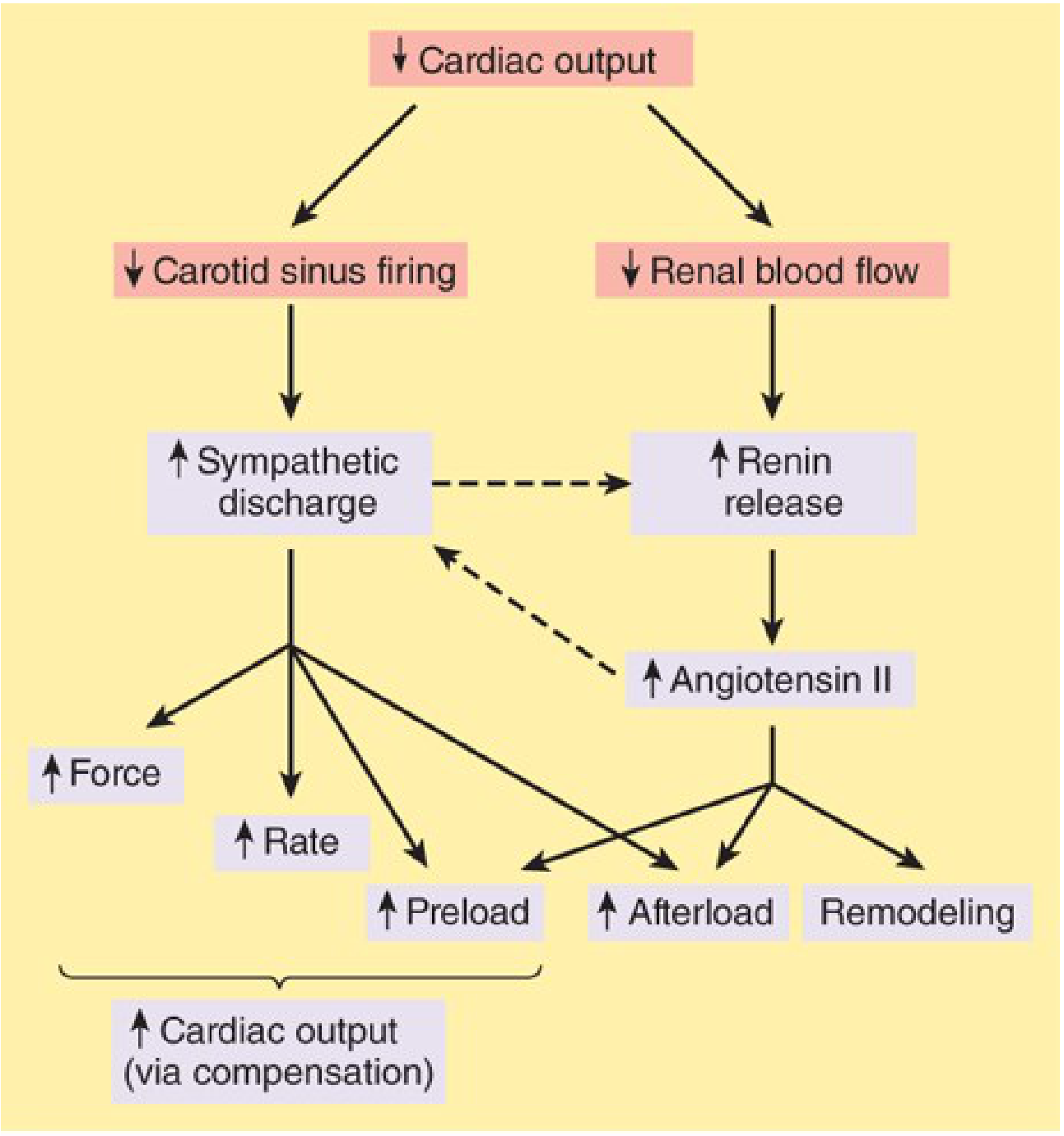
The Vicious Spiral (MUST KNOW)
↓ Cardiac Output
↙ ↘
↓ Baroreceptor ↓ Renal blood flow
firing
↓ ↓
↑ SNS discharge ↑ Renin → ↑ Ang II → ↑ Aldosterone
↓ ↓
↑ HR, contractility ↑ Na+/H₂O retention
↓ ↓
↑ PRELOAD + ↑ AFTERLOAD
↓
MORE ↓ Cardiac Output ← VICIOUS CYCLE
↓
Remodeling (fibrosis, hypertrophy → dysfunction)
Memory Aid - "RAAS BAD in HF":
Renin-Angiotensin-Aldosterone-System causes vasoconstriction + fluid retention → worsens HF. Drugs that block RAAS (ACEi, ARB, MRA) break the cycle.
Left vs Right Heart Failure - "BACK UP" Pattern
| LEFT HF | RIGHT HF | |
|---|---|---|
| Fluid backs up into | LUNGS (pulmonary edema) | BODY (peripheral edema) |
| Symptoms | Dyspnea, orthopnea, PND, pink frothy sputum | Leg edema, JVD, hepatomegaly, ascites |
| Lung finding | Crackles, "hemosiderin-laden macrophages" (heart failure cells) | Pleural effusion (bilateral) |
| Common causes | IHD, HTN, Aortic/Mitral disease | Left HF (most common!), PE, RV infarct, COPD |
| BNP | Elevated | Elevated |
Mnemonic: "Left = Lungs drown; Right = Rest of body drowns"
💥 MODULE 4 — MYOCARDIAL INFARCTION
Time-Based Pathology (The Classic Exam Sequence)
| Time | Gross | Microscopy | Key Feature |
|---|---|---|---|
| 0-6 hrs | Normal (may be pale) | Normal (EM: wavy fibers) | No change on H&E |
| 6-24 hrs | Pale/dark mottling | Coagulative necrosis begins; wavy fibers; pyknosis | Neutrophil infiltration starts |
| 1-3 days | Yellow-pale center | Neutrophils (peak day 2-3) | Most neutrophils = most necrosis |
| 3-7 days | Yellow, soft (rupture risk!) | Macrophages phagocytose necrotic tissue | HIGHEST rupture risk = day 3-7 |
| 1-3 weeks | Red-grey border | Granulation tissue (vascular, fibroblasts) | Red = vascular granulation |
| >6 weeks | White scar | Dense collagen scar | Completed healing |
Mnemonic - "No Change, Neutrophils Munch, Macrophages Clear, Granulation Grows, Scar Sets"
MI Complications - "DRESSLER + PUMP"
| Timing | Complication | Key Detail |
|---|---|---|
| Immediate (0-24h) | Arrhythmias (VF) | #1 cause of death in first hour |
| Days 1-3 | Cardiogenic shock | Pump failure, >40% LV lost |
| Days 3-7 | Free wall rupture → tamponade | Softening (macrophages), sudden death |
| Days 3-7 | Papillary muscle rupture → acute MR | Sudden pulmonary edema, holosystolic murmur |
| Days 3-7 | VSD (septal rupture) | Harsh holosystolic murmur, step-up in RV O₂ |
| Days 1-14 | Mural thrombus → emboli | On endocardium of infarcted zone |
| Weeks | Dressler syndrome | Autoimmune pericarditis (fever, pleurisy, 2-10 weeks post-MI) |
| Months | Ventricular aneurysm | Persistent ST elevation, paradoxical wall motion |
🌡️ MODULE 5 — SYSTOLIC vs DIASTOLIC HF
Quick Pattern Table:
| Feature | HFrEF (Systolic) | HFpEF (Diastolic) |
|---|---|---|
| EF | <40% | ≥50% |
| Defect | Pump can't squeeze (↓ contractility) | Pump can't relax (↑ stiffness) |
| Causes | MI, dilated CMP, myocarditis | HTN, HCM, old age, DM |
| Histology | Dilated thin wall | Thick wall (concentric hypertrophy) |
| Response to inotropes | YES | NO (may worsen) |
| Treatment | ACEi/ARB + BB + MRA + SGLT2i | Rate control, diuretics, treat cause |
💊 MODULE 6 — DRUG TARGETS IN HF (Med School Killer Topic)
The Targets Map
NEUROHUMORAL AXIS
↓
┌─────────┴──────────┐
SNS RAAS
β1-receptor ACE/AT1 receptor
↓ ↓
β-BLOCKERS ACEi / ARBs
(carvedilol, (enalapril,
metoprolol) sacubitril/valsartan)
↓
Aldosterone
↓
MRA (spironolactone,
eplerenone)
FLUID OVERLOAD → DIURETICS (furosemide, HCTZ)
GLUCOSE pathway → SGLT2i (dapagliflozin) ← NEW 1st line
INOTROPES (acute only): Dobutamine (β1), Milrinone (PDE3i)
VASODILATORS: Nitrates (↓ preload), Hydralazine (↓ afterload)
DIGOXIN: ↑ contractility (Na/K-ATPase inhibitor) — narrow TI
Memory Aid - "A-BOMB" for HFrEF treatment:
ACEi/ARB (or sacubitril-valsartan) | Beta-blocker | MRA (mineralocorticoid antagonist) | Big add: SGLT2 inhibitor
🚦 MODULE 7 — ANGINA PATTERNS QUICK COMPARE
| Feature | Stable Angina | Unstable Angina | Prinzmetal (Variant) |
|---|---|---|---|
| Cause | Fixed plaque >70% | Plaque rupture + partial thrombus | Coronary vasospasm |
| Pain pattern | Exertional, relieved by rest | At rest OR crescendo | At rest, nocturnal |
| ECG | ST depression (ischemia) | ST depression / T-wave changes | ST ELEVATION (transient) |
| Troponin | Negative | Positive (UA→NSTEMI) | Usually negative |
| Tx | Nitrates + BB | Anticoagulation + revascularization | Ca-channel blockers (diltiazem) |
Mnemonic: "Stable = Steps only; Unstable = Unplanned at rest; Prinzmetal = Pure spasm"
🧠 MODULE 8 — VALVULAR DISEASE CHEAT SHEET
Stenosis vs Regurgitation Sound Pattern
Mnemonic: "PASS/FAIL"
Pulmonary/Aortic Stenosis = Systolic murmur Mitral/Tricuspid Stenosis = Diastolic murmur Regurgitation = OPPOSITE valve timing
| Valve Lesion | Sound | Classic Cause | Pressure effect |
|---|---|---|---|
| Aortic Stenosis | Systolic ejection murmur (harsh, radiates to neck) | Calcification (>70 yrs) / Bicuspid AV | LV pressure overload → Concentric hypertrophy |
| Aortic Regurgitation | Early diastolic murmur (decrescendo) | Marfan, Syphilis, IE | LV volume overload → Eccentric hypertrophy |
| Mitral Stenosis | Mid-diastolic rumble + opening snap | Rheumatic fever | LA enlargement → AF → Pulmonary HTN |
| Mitral Regurgitation | Holosystolic murmur (radiates to axilla) | MVP, IE, papillary rupture | LA + LV volume overload |
🔬 MODULE 9 — HIGH-YIELD PATHOLOGY BUZZWORDS
| Finding | Diagnosis |
|---|---|
| Foam cells in intima | Atherosclerosis (fatty streak) |
| Wavy fibers (H&E) | Early MI (6-12 hrs) |
| Neutrophils in myocardium | Acute MI (day 1-3) |
| Hemosiderin-laden macrophages (lung) | Left heart failure ("heart failure cells") |
| Vegetations on mitral/aortic valve | Endocarditis (large = IE; small + sterile = Libman-Sacks in SLE) |
| Aschoff bodies + Anitschkow cells | Rheumatic fever (myocarditis) |
| Banana-shaped nucleus macrophage | Anitschkow cell (pathognomonic of rheumatic fever) |
| Concentric onion-skin arterioles | Malignant hypertension |
| Fibrinoid necrosis in vessel walls | Malignant HTN / Vasculitis |
| Mucoid degeneration of valve | MVP (myxomatous degeneration) |
| Apple-green birefringence (Congo red) | Cardiac amyloidosis |
📋 MODULE 10 — ONE-LINE MEMORY AIDS COLLECTION
"SAD LIVES" = Left Heart Failure causes:
Stenosis (aortic/mitral) | Arrhythmias | Dilated CMP | Left IHD | Ischaemia | Valve disease | Endocarditis | Septal defects
"5 R's of Rheumatic Fever (Jones Criteria):"
Carditis | Arthritis (migratory) | Sydenham's Chorea | Subcutaneous nodules | Erythema marginatum Minor: Fever, ↑ ESR/CRP, Prolonged PR interval Mnemonic = "CASES + FP"
"ABC of MI management (STEMI):"
Aspirin + Anticoagulant | Beta-blocker | Clopidogrel/P2Y12 inhibitor | Dual antiplatelet | Early PCI (door-to-balloon <90 min)
"Dressler D's" (post-MI syndrome 2-10 weeks):
Delay (weeks later) | Dull chest pain | Diffuse ST elevation (pericarditis) | Diagnose with Echo | Drug = NSAIDs / Colchicine
🏁 EXAM PATTERN RECOGNITION GUIDE
"What Does the Exam Give You?" Pattern Matching
| Exam Gives You | Think |
|---|---|
| Systolic dysfunction + EF 30% + dilated LV | HFrEF - check cause (MI? Alcohol? Viral?) |
| Normal EF + dyspnea + LV hypertrophy in elderly HTN | HFpEF |
| Acute dyspnea + holosystolic murmur after MI (day 5) | Papillary muscle rupture (acute MR) |
| Persistent ST elevation weeks after MI | Ventricular aneurysm (NOT re-infarction) |
| Fever + chest pain + friction rub 3 weeks post-MI | Dressler syndrome |
| Young athlete + syncope + systolic murmur that increases with Valsalva | HCM (HOCM) - DECREASES with squatting |
| Mid-systolic click + late systolic murmur | Mitral Valve Prolapse (MVP) |
| Opening snap after S2 + mid-diastolic rumble | Mitral Stenosis (rheumatic) |
| Roth spots + Janeway lesions + Osler nodes + murmur + fever | Infective Endocarditis |
| Pulsus paradoxus + muffled heart sounds + JVD (Beck's triad) | Cardiac Tamponade |
Sources: Robbins Cotran & Kumar Pathologic Basis of Disease | Robbins & Kumar Basic Pathology | Katzung's Basic and Clinical Pharmacology 16e | Goodman & Gilman's Pharmacological Basis of Therapeutics
The pathophysiology of cvs medicine + pathology on ischemic heart disease, congestive cardiac failure, rheumatic fever, atheroma , arterioscletosis and others exam oriented simple flow charts
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
I have all the key source material. Now let me compile the full, deeply exam-oriented guide with clean flowcharts for every topic.
🫀 CARDIOVASCULAR PATHOPHYSIOLOGY — EXAM CRUSH MASTER GUIDE
IHD · CCF · Rheumatic Fever · Atheroma · Arteriosclerosis + More
Sources: Robbins Cotran & Kumar Pathologic Basis of Disease | Goldman-Cecil Medicine | Katzung's Clinical Pharmacology
═══════════════════════════════════
PART 1 — ARTERIOSCLEROSIS & ATHEROMA
═══════════════════════════════════
🔷 1A. ARTERIOSCLEROSIS — 3 Types (The Forgotten Comparison)
ARTERIOSCLEROSIS
(Hardening of arteries)
│
┌─────────┼─────────────┐
▼ ▼ ▼
ATHEROSCLEROSIS ARTERIOLOSCLEROSIS MONCKEBERG'S
(Large/medium (Small arteries MEDIAL
arteries) & arterioles) CALCIFICATION
│ │ │
Lipid plaque 2 sub-types: Calcium deposits
in INTIMA ① Hyaline (benign in MEDIA of
HTN, DM) medium arteries
② Hyperplastic NO atheroma
(malignant HTN) NO lumen change
"Onion-skin" CLINICALLY SILENT
(incidental X-ray)
Exam Tip: Only atherosclerosis causes lumen narrowing that matters clinically. Monckeberg is BENIGN and found incidentally on X-ray as "pipe-stem" calcification.
🔷 1B. ATHEROMA (Atherosclerosis) — Complete Pathophysiology Flowchart
RISK FACTORS
┌─────────────────────────────────────────────┐
│ HTN · Smoking · DM · Hyperlipidemia │
│ Obesity · Age · Male sex · Family Hx │
└─────────────────────────────────────────────┘
↓
ENDOTHELIAL INJURY / DYSFUNCTION
(Mechanical stress, oxidized LDL, toxins)
↓
┌───────────────────────────────┐
│ ↑ Permeability of intima │
│ LDL enters & oxidizes │
│ Monocytes adhere & migrate │
└───────────────────────────────┘
↓
FATTY STREAK (EARLIEST LESION)
Macrophages engulf oxidized LDL
→ FOAM CELLS form
T lymphocytes accumulate
↓
FIBROUS PLAQUE
SMC migrate media → intima
SMC proliferate + secrete ECM
Lipid core + Fibrous cap forms
↓
COMPLICATED PLAQUE (ADVANCED)
┌────────────────────────────────────┐
│ Calcification Ulceration │
│ Haemorrhage Thrombosis │
└────────────────────────────────────┘
↙ ↘
STABLE PLAQUE VULNERABLE PLAQUE
(Thick fibrous cap, (Thin cap, large
heavy calcification, lipid core, many
gradual stenosis) macrophages)
↓ ↓
STABLE ANGINA PLAQUE RUPTURE
↓
ACUTE THROMBOSIS
↓
┌───────────────┬─────────────┐
↓ ↓ ↓
STEMI / MI UNSTABLE SUDDEN
ANGINA DEATH
Atheroma Memory Aids:
"5 F's of Atherosclerosis Risk":
Fat (dyslipidaemia) · Family history · Fags (smoking) · Fat (obesity) · Forty+ (age)
"FOAM cell formation":
Fatty streak → Oxidised LDL phagocytosed → Accumulate in macrophages → Macrophages = FOAM cells
Key Exam Anatomy of a Plaque:
Lumen
─────────────────────────────
FIBROUS CAP
(Smooth muscle + collagen)
─────────────────────────────
LIPID CORE
(Cholesterol + necrotic
debris + foam cells)
─────────────────────────────
SHOULDER REGION ← Rupture-prone!
(Macrophages, T cells, thin cap)
─────────────────────────────
Media
═══════════════════════════════════
PART 2 — ISCHEMIC HEART DISEASE (IHD)
═══════════════════════════════════
🔴 2A. IHD Master Flowchart
CORONARY ATHEROSCLEROSIS (90% of IHD)
↓
┌──────┴───────┐
↓ ↓
STABLE UNSTABLE/RUPTURE
(Fixed stenosis (Plaque rupture
>70% lumen) + thrombus)
↓ ↓
STABLE ACUTE CORONARY
ANGINA SYNDROMES (ACS)
┌──────┬──────┐
↓ ↓ ↓
UNSTABLE NSTEMI STEMI
ANGINA
🔴 2B. Oxygen Supply vs Demand — The Core Concept
MYOCARDIAL ISCHAEMIA occurs when:
DEMAND > SUPPLY
DEMAND ↑ by: SUPPLY ↓ by:
• ↑ Heart rate • Stenotic artery (atheroma)
• ↑ Contractility • Coronary spasm (Prinzmetal)
• ↑ Wall tension • Thrombosis
• ↑ BP (afterload) • Anaemia (↓ O₂ carrying)
• Hypertrophy • Tachycardia (↓ diastolic
filling time)
🔴 2C. Angina Types — Side-by-Side Pattern
STABLE UNSTABLE PRINZMETAL
ANGINA ANGINA (VARIANT)
─────────────────────────────────────────────────────
CAUSE Fixed plaque Plaque rupture Vasospasm
(>70%) + partial (no fixed
thrombus plaque needed)
TRIGGER Exertion Rest OR less REST, often
exertion nocturnal
than before
ECG ST ↓ (during ST ↓ / T-wave ST ↑
episode) inversion (transient!)
TROPONIN Negative Often +ve Usually –ve
RELIEF Rest/GTN Partial GTN Ca-channel
blockers
TREATMENT BB + Nitrates DAPT + Heparin Diltiazem/
+ CCB + PCI Verapamil
🔴 2D. MYOCARDIAL INFARCTION — Sequence of Events
The Time-Based Pathology Table (Exam Favourite)
TIME GROSS HISTOLOGY KEY EXAM POINT
─────────────────────────────────────────────────────────────────────
0–4 hrs NORMAL Wavy/elongated No change on
fibres (EM) H&E! (trick Q)
No H&E change
4–12 hrs Pale / dark Coagulative Earliest
mottling necrosis begins, VISIBLE change
pyknosis, loss on H&E
of striations
12–24 hrs Pale / mottled Neutrophil Neutrophils
infiltration arrive
(peak day 2–3)
1–3 days YELLOW Dense neutrophils, Peak necrosis
soft centre nuclear debris period
3–7 days YELLOW, SOFT Macrophages ⚠ HIGHEST
(most danger!) phagocytose RUPTURE RISK
debris
1–3 wks Red-grey rim Granulation tissue Angiogenesis
(vascular + begins
fibroblasts)
>6 wks White fibrous Dense collagen SCAR complete
scar scar, no cells Non-contractile
Mnemonic — "Normal Neutrophils Must Go, Granulation Seals":
N-ormal · N-eutrophils · M-acrophages · G-ranulation · S-car
MI Complications Flowchart
ACUTE MI
│
├─ 0–24h: ARRHYTHMIAS (VF = #1 early death)
│ ↑ K+ leaks from necrotic cells → VF
│
├─ 1–3d: CARDIOGENIC SHOCK
│ Loss >40% LV myocardium
│ ↓CO → ↓BP → ↓organ perfusion
│
├─ 3–7d: MECHANICAL COMPLICATIONS (softening phase)
│ ├──── FREE WALL RUPTURE → Haemopericardium → TAMPONADE
│ │ (sudden death; Beck's triad: ↓BP, ↑JVP, muffled sounds)
│ ├──── PAPILLARY MUSCLE RUPTURE → Acute MR
│ │ (sudden pulmonary oedema, holosystolic murmur → axilla)
│ └──── SEPTAL RUPTURE (VSD)
│ (harsh holosystolic murmur, step-up in RV O₂)
│
├─ Days–Weeks: MURAL THROMBUS
│ Adherent to endocardium of infarcted zone
│ Risk of systemic emboli (stroke, mesenteric ischaemia)
│
├─ 2–10wks: DRESSLER SYNDROME
│ Autoimmune pericarditis post-MI
│ Fever + pleuritic chest pain + friction rub
│ Treatment: NSAIDs / Colchicine
│
└─ Months: VENTRICULAR ANEURYSM
Persistent ST elevation on ECG
Paradoxical systolic bulge
Risk of thrombus + refractory HF
═══════════════════════════════════
PART 3 — CONGESTIVE CARDIAC FAILURE (CCF)
═══════════════════════════════════
💙 3A. CCF Master Pathophysiology Flowchart
UNDERLYING CAUSE
┌─────────────────────────────────────────────────────┐
│ IHD · HTN · Valvular disease · Cardiomyopathy │
│ Congenital · Myocarditis · Arrhythmia │
└─────────────────────────────────────────────────────┘
↓
↓ MYOCARDIAL CONTRACTILITY
or ↑ WORKLOAD (pressure/volume)
↓
↓ CARDIAC OUTPUT
↓
┌───────────┴──────────┐
▼ ▼
↓ Baroreceptor ↓ Renal Perfusion
firing (carotid) ↓
↓ ↑ Renin → Ang II
↑ Sympathetic ↑ Aldosterone
discharge ↓
↑ HR, contractility, Na+/H₂O retention
vasoconstriction ↓
↓ ↑ Circulating volume
└─────────┬────────┘
↓
↑ PRELOAD + ↑ AFTERLOAD
↓
CARDIAC HYPERTROPHY/DILATION
↓
FURTHER ↓ CARDIAC OUTPUT
↓
VICIOUS CYCLE → DEATH
Key Compensatory Mechanisms & Why They Fail:
| Mechanism | Initially Helpful | Eventually Harmful |
|---|---|---|
| ↑ HR (SNS) | Maintains CO | Tachycardia → ↓ diastolic filling, ischaemia |
| ↑ Vasoconstriction (Ang II) | Maintains BP | ↑ Afterload → worsens pump function |
| Na+ retention (Aldosterone) | ↑ Preload | Fluid overload → congestion, oedema |
| Cardiac hypertrophy | ↑ Wall strength | Fibrosis, arrhythmias, poor relaxation |
💙 3B. LEFT vs RIGHT Heart Failure Flowchart
LEFT HEART FAILURE RIGHT HEART FAILURE
(Most common: IHD, HTN) (Most common CAUSE = Left HF!)
↓ ↓
LV cannot pump forward RV cannot pump forward
↓ ↓
Blood backs up into Blood backs up into
PULMONARY CIRCULATION SYSTEMIC VENOUS circulation
↓ ↓
Pulmonary venous HTN ↑ Systemic venous pressure
↓ ↓
Pulmonary oedema Peripheral oedema
Hepatomegaly / ascites
SYMPTOMS: SYMPTOMS:
• Dyspnoea on exertion • Pitting oedema (legs)
• Orthopnoea (2+ pillows) • JVP elevation
• Paroxysmal nocturnal • Hepatomegaly (tender)
dyspnoea (PND) • Ascites
• Pink frothy sputum • Anorexia / nausea
• Fine crackles (lungs) • Engorged neck veins
PATHOLOGY: PATHOLOGY:
• Heavy wet lungs • Nutmeg liver
• Heart failure cells • Congestive
(haemosiderin-laden splenomegaly
macrophages) • Peripheral oedema
• Pulmonary oedema
Memory Aid — "LMNOP for acute pulmonary oedema Rx":
Lasix (furosemide) · Morphine · Nitrates · Oxygen · Posture (sit upright)
💙 3C. Systolic vs Diastolic HF (HFrEF vs HFpEF)
HFrEF HFpEF
(Systolic) (Diastolic)
─────────────────────────────────────────────────
EF < 40% ≥ 50%
PROBLEM Can't SQUEEZE Can't RELAX
(↓ contractility) (↑ stiffness)
CAUSE MI, Dilated CMP, HTN, HCM,
Myocarditis, Old age, DM,
Alcohol, Viral Amyloid
WALL Thin + Dilated Thick + Stiff
(Eccentric hypertrophy) (Concentric hypertrophy)
Rx TARGET Reduce remodelling: Rate control,
ACEi + BB + MRA + Diuretics
SGLT2i (treat cause)
INOTROPES? YES (in acute) NO (may worsen)
═══════════════════════════════════
PART 4 — RHEUMATIC FEVER & RHD
═══════════════════════════════════
🟡 4A. Pathogenesis Flowchart (Molecular Mimicry)
Group A Streptococcus (GAS)
pharyngitis
↓
2–3 week latent period
(Antibody production time)
↓
Antibodies to Streptococcal M protein
CROSS-REACT with cardiac antigens
↓
┌──────────────────────────────┐
│ Molecular Mimicry │
│ (Strep M protein ≈ cardiac │
│ sarcolemmal proteins) │
└──────────────────────────────┘
↓
T cell + Antibody-mediated
IMMUNE ATTACK on heart
↓
PANCARDITIS = Pericarditis
+ Myocarditis
+ Endocarditis
↓
ASCHOFF BODIES in myocardium
(pathognomonic!)
↓
With repeated attacks:
CHRONIC RHEUMATIC HEART DISEASE
Key: Streptococci are ABSENT from the lesions (pure immune injury)
🟡 4B. Acute Rheumatic Fever — JONES CRITERIA
JONES CRITERIA (Diagnosis requires 2 MAJOR or 1 MAJOR + 2 MINOR)
+ Evidence of preceding GAS infection
MAJOR CRITERIA MINOR CRITERIA
("CASE C") ("FFFPPP")
─────────────────────────────────────────────────────
C arditis F ever
A rthritis (migratory, F↑ ESR / CRP
large joints — "flitting") P rolonged PR interval
S ydenham's Chorea (1st degree AV block)
("St Vitus' dance")
E rythema Marginatum
(skin — macular, central
clearing, like a map)
S ubcutaneous Nodules
(over bony prominences)
PLUS: Evidence of GAS infection
• ↑ ASO titre · Throat culture · Recent scarlet fever
Memory Mnemonic — "CASES F-P":
Carditis · Arthritis · Sydenham's chorea · Erythema marginatum · Subcutaneous nodules + Fever · Prolonged PR
🟡 4C. Pathology — Morphological Features
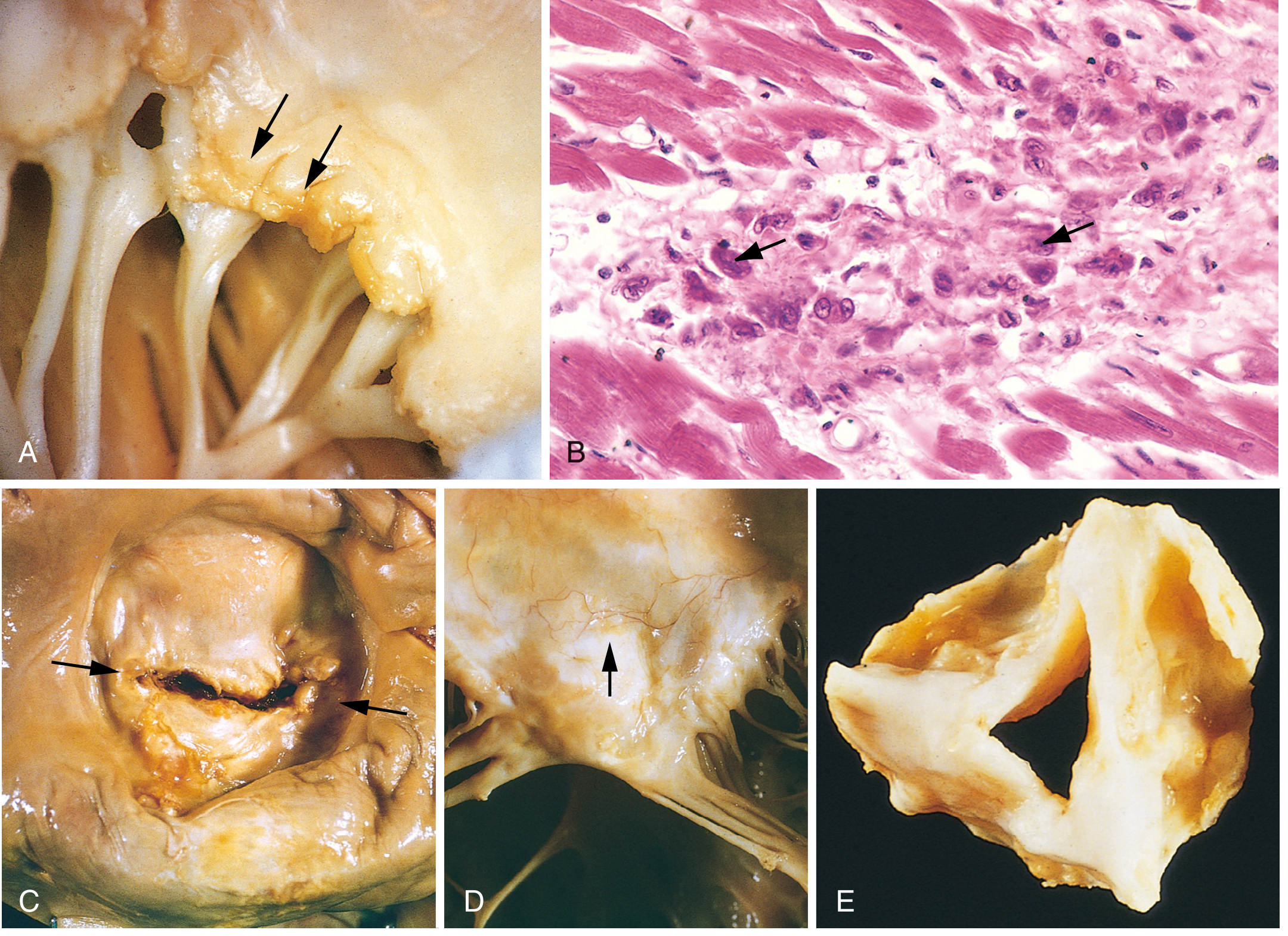
ACUTE RHD CHRONIC RHD
─────────────────────────────────────────────────
ASCHOFF BODIES VALVE SCARRING
• Myocardial foci of • Fibrous thickening
T-lymphocytes + of leaflets
plasma cells + • Commissural fusion
ANITSCHKOW cells • Chordae thickening
("caterpillar cells") and fusion
VERRUCAE FISH-MOUTH / BUTTON-
• Small 1–2mm vegetations HOLE STENOSIS
on valve line of closure (mitral valve — classic)
(ALONG closure line,
unlike IE which is on NEOVASCULARISATION
leaflet surface) of valve leaflets
MACCALLUM PLAQUE VALVES AFFECTED:
• Left atrial subendo- Mitral > Mitral+Aortic
cardial thickening > Tricuspid (rare)
🟡 4D. RHD → Mitral Stenosis Chain
Repeated RF episodes
↓
Mitral valve leaflet fusion + thickening
↓
MITRAL STENOSIS (RHD = virtually ONLY cause)
↓
"Fish mouth" / "button hole" valve orifice
↓
↑ LA pressure → LA ENLARGEMENT
↓
┌─────┴──────┐
↓ ↓
ATRIAL PULMONARY
FIBRILLATION HYPERTENSION
(risk of LA ↓
thrombus + Right heart
embolism) failure (cor pulmonale)
Exam Sign Pattern:
Opening Snap (OS) after S2
+
Mid-diastolic rumbling murmur (at apex)
+
Loud S1 (due to valve snapping shut)
= MITRAL STENOSIS (rheumatic)
═══════════════════════════════════
PART 5 — CARDIOMYOPATHIES (Bonus High-Yield)
═══════════════════════════════════
🟣 The 3 Types — Pattern Table
DILATED (DCM) HYPERTROPHIC (HCM) RESTRICTIVE (RCM)
──────────────────────────────────────────────────────────────────
PATHOLOGY Dilation + Asymmetric septal Stiff myocardium
systolic dysfun. hypertrophy Diastolic dysfun.
CAUSE Idiopathic (40%) GENETIC (AD) Amyloid, sarcoid,
Alcohol, viral MYH7 / MYBPC3 haemochromatosis
myocarditis, mutation eosinophilia
peripartum
SHAPE Dilated, Thick Normal size /
thin walls asymmetric slightly enlarged
septum stiff wall
OUTFLOW Normal OBSTRUCTION Normal
(until late) (HOCM — LVOTO)
MURMUR S3 gallop Systolic ejection ↑ JVP, ↓ pulse
murmur pressure
KEY Rx ACEi + BB + BB / Verapamil Treat cause
Diuretics Avoid inotropes! Diuretics (careful)
SGLT2i ICD if at risk
EXAM CLUE Young patient Young athlete Congo red +
+ AF + dilated + syncope + birefringence
LV on echo septal hypertrophy = AMYLOID
Mnemonic for HCM exam presentation:
"Young athlete drops dead OR syncopes on exertion + systolic murmur that INCREASES with Valsalva/standing, DECREASES with squatting/leg raise"
═══════════════════════════════════
PART 6 — ENDOCARDITIS COMPARISON
═══════════════════════════════════
🔶 Endocarditis Types — Quick Pattern
INFECTIVE (IE) RHEUMATIC LIBMAN-SACKS MARANTIC
(RHD) (SLE) (Terminal)
──────────────────────────────────────────────────────────────────────
VEGETAT. LARGE, irregular, Small (1–2mm) Small, sterile, Small, sterile
SIZE friable along closure on BOTH sides multiple
line of leaflet
LOCATION Atrial surface of Closure line Both surfaces Any valve
AV valves; of mitral of mitral
ventricular valve valve
surface of
semilunar
ORGANISM Strep viridans NONE NONE NONE
(dental); Staph (immune) (immune) (debilitating
aureus (IV drug); illness)
Strep bovis
(colon cancer link!)
KEY EXAM Roth spots, Aschoff SLE patient, Cancer/
FEATURES Osler nodes, bodies, antiphospholipid cachexia
Janeway lesions, caterpillar syndrome patient
splinter haemorrhages cells, mitral
stenosis
Mnemonic — "FROM JANE" for IE signs:
Fever · Roth spots (retina) · Osler nodes (painful, fingers) · Murmur · Janeway lesions (painless palms) · Anaemia · Nail (splinter haemorrhages) · Emboli (septic)
═══════════════════════════════════
PART 7 — TREATMENT FLOWCHARTS
═══════════════════════════════════
💊 STEMI Management — "TIME = MUSCLE"
STEMI Diagnosed (ST elevation + symptoms)
↓
IMMEDIATE (within 10 minutes):
Aspirin 300mg + P2Y12 inhibitor (ticagrelor/clopidogrel)
+ Anticoagulation (heparin/fondaparinux)
+ O₂ only if SpO₂ <94%
+ GTN if no hypotension
↓
REPERFUSION STRATEGY:
┌─────────────────────────────┐
│ PCI available? │
│ YES → Primary PCI │
│ (door-to-balloon │
│ <90 mins) │
│ NO → Thrombolysis │
│ (within 12h onset) │
│ Streptokinase/ │
│ Alteplase │
└─────────────────────────────┘
↓
SECONDARY PREVENTION:
DAPT (12 months)
Beta-blocker (reduce remodelling)
ACEi/ARB (reduce remodelling, ↓ mortality)
Statin (stabilise plaque, ↓ LDL)
+/– Eplerenone (if EF <40%)
💊 CCF/HFrEF Treatment — The "A-BOMB" Rule
ALL HFrEF PATIENTS (EF <40%) get:
A — ACEi (or ARB, or sacubitril/valsartan)
↓ Afterload, ↓ remodelling, ↓ mortality
B — Beta-Blocker (carvedilol, bisoprolol, metoprolol)
↓ HR, ↓ remodelling, ↓ sudden death
M — MRA (spironolactone or eplerenone)
↓ Aldosterone effects, ↓ fibrosis
+SGLT2 inhibitor (dapagliflozin / empagliflozin)
New 1st line — reduces HF hospitalisation
+ DIURETICS for symptoms (furosemide for oedema)
For refractory/advanced HF:
+ Ivabradine (if HR >70 in sinus rhythm)
+ Hydralazine + Isosorbide dinitrate (if ACEi intolerant)
+ ICD (if EF <35% despite 3 months Rx)
+ CRT (if LBBB + EF <35%)
═══════════════════════════════════
PART 8 — ONE-PAGE BUZZ-WORD MAP
═══════════════════════════════════
| Buzzword / Finding | Disease |
|---|---|
| Foam cells in intima | Atherosclerosis (fatty streak) |
| Wavy myocardial fibres (H&E, <12h) | Early MI |
| Neutrophil infiltration (day 1–3) | Acute MI |
| Macrophage-rich zone (day 3–7) | Peak rupture risk window |
| Haemosiderin-laden macrophages in lung | Left heart failure ("heart failure cells") |
| Aschoff bodies + Anitschkow "caterpillar" cells | Rheumatic fever |
| Small 1–2mm vegetations ALONG closure line | Rheumatic endocarditis |
| Large irregular friable vegetations | Infective endocarditis |
| Vegetations on BOTH SIDES of mitral valve | Libman-Sacks (SLE) |
| "Fish mouth" mitral valve | Chronic rheumatic mitral stenosis |
| Asymmetric septal hypertrophy | HCM (HOCM) |
| Apple-green birefringence on Congo red | Cardiac amyloidosis (RCM) |
| "Onion-skin" arteriolar walls | Malignant hypertension |
| Fibrinoid necrosis + arteriolar wall | Malignant HTN / Vasculitis |
| Pipe-stem calcification on X-ray | Monckeberg's medial calcification |
| Concentric LV hypertrophy + thick wall | HTN / Aortic stenosis |
| Dilated LV + thin wall | Dilated CMP / Late HFrEF |
| Persistent ST elevation weeks post-MI | Ventricular aneurysm |
| Fever + rub + chest pain 2–10 wks post-MI | Dressler syndrome |
| Beck's triad (↓BP + ↑JVP + muffled sounds) | Cardiac tamponade |
| Loud S1 + Opening snap + Mid-diastolic rumble | Mitral stenosis (rheumatic) |
═══════════════════════════════════
PART 9 — EXAM PATTERN RECOGNITION
═══════════════════════════════════
QUESTION GIVES YOU: THINK:
──────────────────────────────────────────────────────────
Young + sore throat + 3 wks later RHEUMATIC FEVER
fever, migratory arthritis, (Jones criteria!)
carditis
↑ ASO titre + 1st degree AV block RF minor criteria
+ fever
Mid-diastolic rumble + opening snap MITRAL STENOSIS
+ AF + history of RF (RHD)
Acute MI + day 5 + sudden PAPILLARY MUSCLE
holosystolic murmur + pulmonary RUPTURE → acute MR
oedema
Acute MI + day 5 + harsh VENTRICULAR SEPTAL
holosystolic murmur + right heart RUPTURE (VSD)
strain + step-up in RV O₂
Acute MI + sudden drop in BP + FREE WALL RUPTURE
JVP rising + muffled sounds → TAMPONADE
Persistent ST elevation 3 months VENTRICULAR
post-MI + paradoxical wall motion ANEURYSM
Young athlete + syncope + HCM (HOCM)
↑ murmur with Valsalva
Fever + new murmur + IV drug user INFECTIVE
or recent dental work ENDOCARDITIS
+ Osler nodes + Roth spots
SLE patient + valve vegetations LIBMAN-SACKS
on both sides ENDOCARDITIS
Elderly + calcific aortic stenosis NORMAL WEAR
(crescendo-decrescendo murmur (NOT rheumatic)
radiating to neck)
Marfan / Syphilis patient + AORTIC
early diastolic murmur REGURGITATION
Sources: Robbins Cotran & Kumar Pathologic Basis of Disease (9e) | Goldman-Cecil Medicine International Edition | Katzung's Basic and Clinical Pharmacology 16e | Robbins & Kumar Basic Pathology
This is a shared conversation. Sign in to Orris to start your own chat.