Iron biochemistry
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content from multiple authoritative textbooks and four excellent diagrams. Let me compile the full answer.
Iron Biochemistry
1. Total Body Iron Content and Distribution
The total iron in the body averages 4-5 grams in adults, distributed as follows:
| Compartment | % of Total | Amount |
|---|---|---|
| Hemoglobin (erythrocytes) | ~65% | ~2,500 mg |
| Myoglobin (muscle) | ~4% | ~150 mg |
| Heme enzymes (cytochromes, catalase, peroxidase) | ~1% | ~15 mg |
| Transferrin (plasma transport) | ~0.1% | ~3 mg |
| Storage (ferritin + hemosiderin) | 15-30% | 200-1,000 mg liver + ~600 mg macrophages |
- Guyton and Hall Textbook of Medical Physiology, p. 446
- Harrison's Principles of Internal Medicine 22E, p. 806
2. Iron's Functional Roles
Iron is indispensable for:
- Oxygen transport - as the core of heme in hemoglobin and myoglobin
- Cellular respiration - cytochromes and cytochrome oxidase in the electron transport chain
- Antioxidant defense - catalase and peroxidase
- DNA synthesis - ribonucleotide reductase (non-heme iron)
- Energy production - iron-sulfur (Fe-S) clusters in mitochondrial complexes
- Cell cycle regulation - iron utilized in mitochondria to form heme and Fe-S clusters
Because free iron generates reactive oxygen species (ROS) via Fenton chemistry, it is always protein-bound and its homeostasis is tightly regulated.
3. Intestinal Absorption
Only 1-2 mg/day is absorbed from the diet (dietary intake is ~15 mg/day; ~6 mg per 1,000 kcal).
Heme iron
- Derived from red meat myoglobin and hemoglobin
- Taken up intact by enterocytes via an undefined mechanism
- Constitutes only ~6% of dietary iron but represents ~30% of absorbed iron
- Not affected by dietary inhibitors
Non-heme iron
- Must be reduced from Fe³+ → Fe²+ before absorption
- Steps:
- Gastric acid lowers luminal pH, facilitating reduction
- Duodenal cytochrome B (DCYTB) - a brush-border ferrireductase converts Fe³+ to Fe²+
- DMT1 (Divalent Metal Transporter 1) imports Fe²+ across the apical membrane into the enterocyte
- Iron is either stored as ferritin within the enterocyte or exported at the basolateral membrane by ferroportin
- At the basolateral surface, hephaestin (a ceruloplasmin-like oxidase) re-oxidizes Fe²+ to Fe³+, which then binds transferrin in plasma
Enhancers of absorption: ascorbic acid, meat, acidic pH
Inhibitors: phytates, phosphates (in vegetables/cereals), tannins (tea, coffee)
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, p. 927
- Harrison's Principles of Internal Medicine 22E, p. 806
4. Plasma Transport: Transferrin
- Transferrin is a 76 kDa beta-globulin glycoprotein synthesized by the liver
- Each molecule has two binding sites for Fe³+ (monoferric or diferric)
- Normal plasma level: 204-360 mg/dL
- Carries only ~3-4 mg of iron but turns over 10x per day (~30-40 mg/day flux)
- ~80% of plasma iron is delivered to the erythroid marrow for hemoglobin synthesis
Transferrin Receptor-Mediated Uptake (TfR1)
- Diferric transferrin binds TfR1 (CD71) on the cell surface
- The complex is internalized via clathrin-coated pit endocytosis
- A proton-pumping ATPase acidifies the endosome to ~pH 5.5
- Iron dissociates from transferrin; STEAP3 (a ferrireductase) reduces Fe³+ to Fe²+
- DMT1 transports Fe²+ into the cytosol, then to mitochondria for heme synthesis
- Apotransferrin returns to the cell surface and is released back into circulation
- Henry's Clinical Diagnosis and Management by Laboratory Methods, p. 675
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, p. 927
5. Iron Storage: Ferritin and Hemosiderin
Ferritin
- A protein-iron storage complex; apoferritin MW ~450-460 kDa
- Composed of 24 subunits (H-heavy and L-light chains)
- H subunits have ferroxidase activity (oxidize Fe²+ to Fe³+ for incorporation)
- H gene on chromosome 11; L gene on chromosome 19
- Central cavity stores a crystalline core of ferric oxyhydroxide (FeOOH)
- Can hold up to 4,000 atoms of iron per molecule; >30% of its weight may be iron
- Water-soluble, iron is readily mobilizable
Hemosiderin
- Aggregates of FeOOH core crystals with partially degraded protein shells (lysosomal proteolysis)
- Water-insoluble; visible as large granules under light microscopy
- Iron is much harder to mobilize than ferritin iron
- Accumulates when total body iron exceeds apoferritin storage capacity
Storage sites: reticuloendothelial system (liver Kupffer cells, splenic macrophages, bone marrow) and hepatocytes.
6. Iron Recycling by Macrophages
-
Senescent RBCs (lifespan ~120 days) are phagocytosed by splenic and liver macrophages
-
Hemoglobin → heme → iron is liberated within the macrophage
-
Heme is catabolized by heme oxygenase → biliverdin → bilirubin + Fe²+
-
Ferroportin on the macrophage surface exports iron back to plasma
-
This recycling provides ~20-25 mg iron/day - far exceeding the 1-2 mg dietary absorption
-
In intravascular hemolysis: hemoglobin-haptoglobin and heme-hemopexin complexes are taken up by hepatocytes and macrophages respectively
-
Harrison's Principles of Internal Medicine 22E, p. 807
7. The Iron Cycle (Visual)
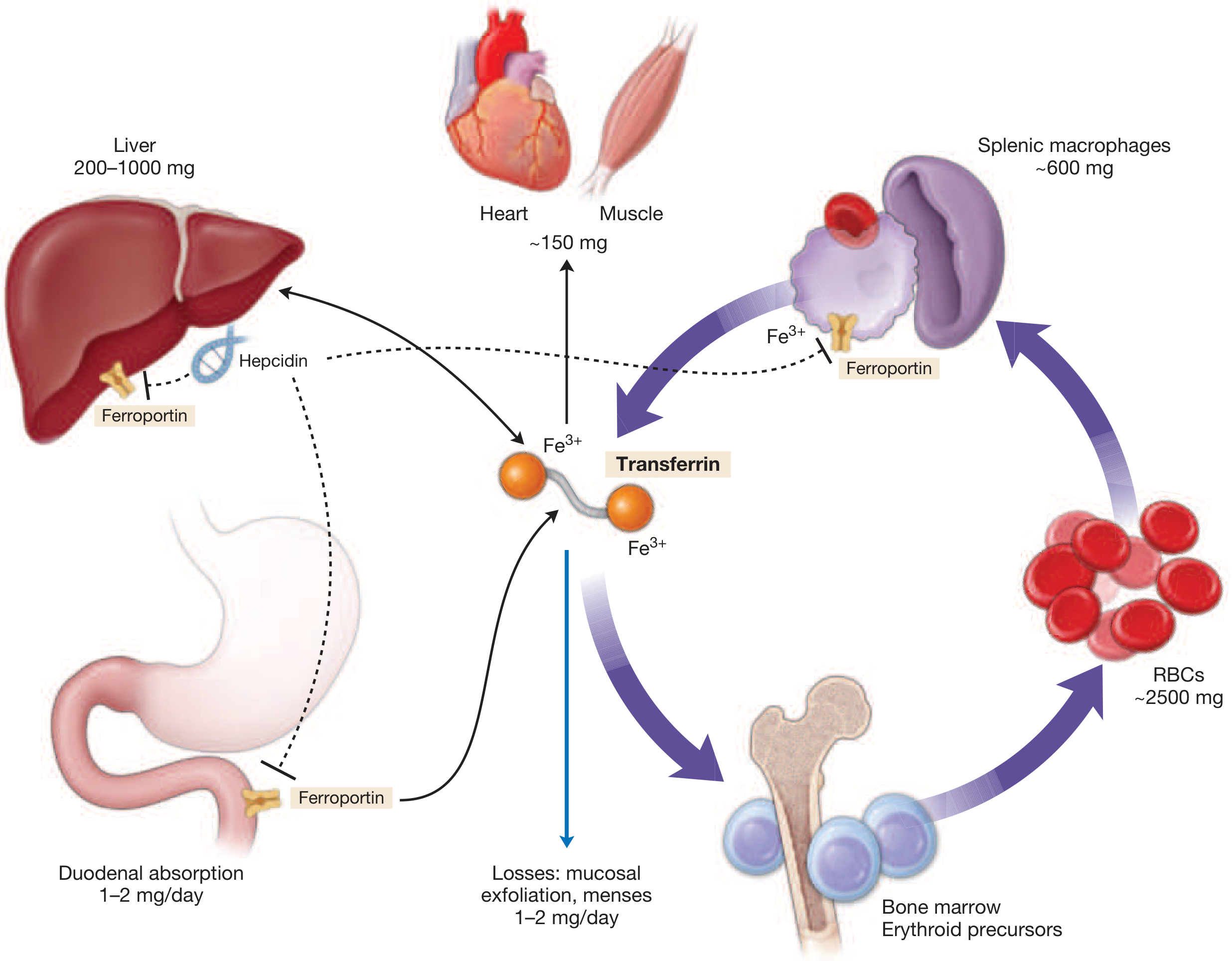
Iron cycle: Transferrin is central to iron trafficking. Most iron (20-25 mg/day) is recycled from macrophages; only 1-2 mg comes from intestinal absorption. Hepcidin controls ferroportin activity.
- Harrison's Principles of Internal Medicine 22E
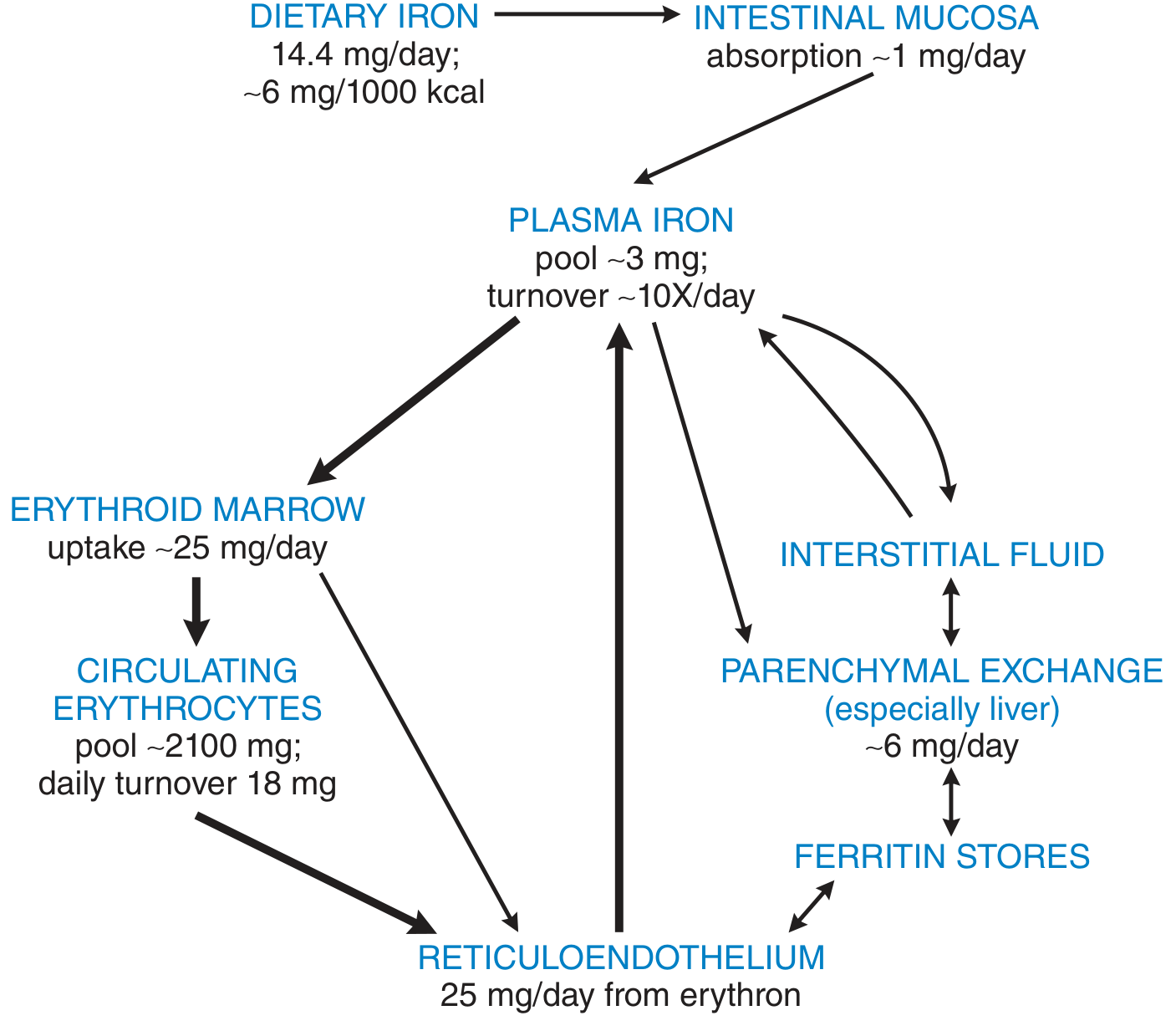
Quantitative iron flow: plasma iron pool of ~3 mg turns over ~10×/day; erythroid marrow uptake ~25 mg/day; RBC pool ~2,100 mg
- Goodman & Gilman's The Pharmacological Basis of Therapeutics
8. Hepcidin - The Master Regulator
Hepcidin is a 25-amino acid antimicrobial peptide encoded by the HAMP gene, produced and secreted by the liver. It is the primary systemic regulator of iron homeostasis.
Mechanism of Action
- Hepcidin binds to ferroportin on the surface of enterocytes, macrophages, and hepatocytes
- This triggers internalization and lysosomal degradation of ferroportin
- Reduced ferroportin activity means: less iron absorption from gut + less iron release from macrophage stores → hypoferremia
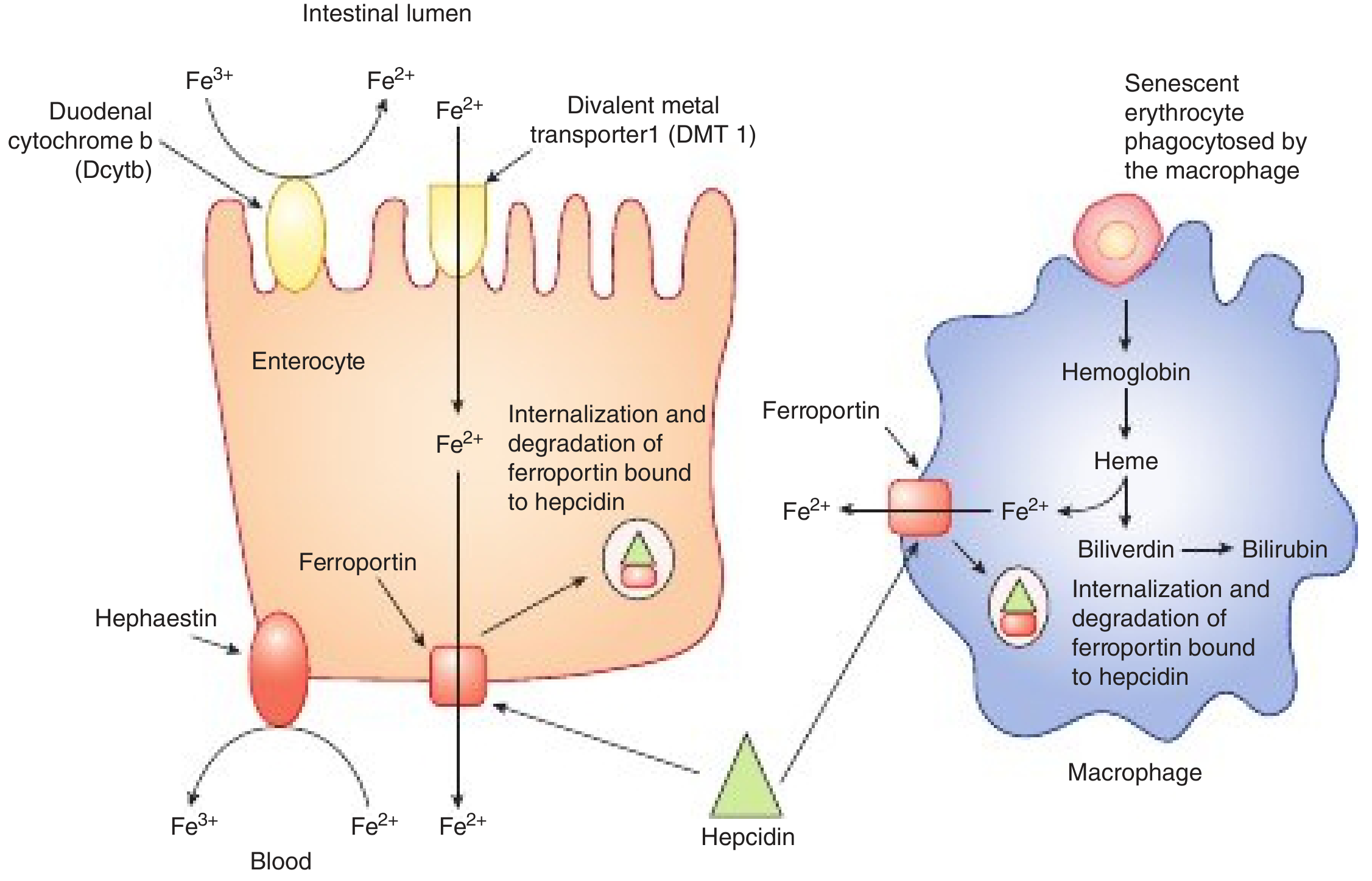
Hepcidin binds ferroportin on both enterocytes and macrophages, triggering its internalization and degradation
- Harper's Illustrated Biochemistry, 32nd Ed, p. 654
Signals that INCREASE hepcidin (reduce iron absorption)
| Signal | Pathway |
|---|---|
| High iron / high transferrin saturation | HFE-TfR2 complex → BMP-SMAD signaling |
| Inflammation | IL-6 → JAK-STAT pathway |
| BMP ligands + hemojuvelin (HJV) coreceptor | BMP receptor → SMAD → HAMP transcription |
Signals that DECREASE hepcidin (increase iron absorption)
| Signal | Mechanism |
|---|---|
| Iron deficiency | TMPRSS6 antagonizes BMP pathway |
| Hypoxia / hemorrhage | Erythroferrone (from erythroblasts) sequesters BMPs |
| Erythropoietin stimulation | Increases erythroferrone |
| Testosterone | Adapts supply to male erythropoiesis |
| FGL1 (fibrinogen-like protein 1) | Released by hepatocytes |
- Harrison's Principles of Internal Medicine 22E, p. 806
- Harper's Illustrated Biochemistry, 32nd Ed, pp. 653-654
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 788
9. Cellular Iron Regulation: IRP/IRE System
At the cellular level, iron supply is sensed by two Iron Regulatory Proteins (IRP1 and IRP2) - cytosolic RNA-binding proteins:
| mRNA target | IRE location | Effect of IRP binding (low iron) |
|---|---|---|
| Ferritin mRNA | 5' UTR | Represses translation (less storage) |
| TfR1 mRNA | 3' UTR | Stabilizes mRNA → more receptor expression (more uptake) |
| Ferroportin mRNA | 5' UTR | Represses translation (less export) |
| HIF-2α mRNA | 5' UTR | Regulates erythropoietin expression |
| ALAS2 mRNA (5'-aminolevulinate synthase) | 5' UTR | Regulates first step of heme synthesis |
Low iron → IRPs bind IREs:
- ↓ Ferritin (less storage)
- ↑ TfR1 (more uptake)
- Net effect: more iron captured
High iron → IRPs do not bind IREs:
-
↑ Ferritin (more storage)
-
↓ TfR1 (less uptake)
-
Net effect: excess iron stored safely
-
Goodman & Gilman's The Pharmacological Basis of Therapeutics, p. 927
-
Harrison's Principles of Internal Medicine 22E, p. 806
10. Iron Loss
The body has no regulated excretion mechanism for iron. Iron is lost passively:
- Men: ~0.6-1 mg/day (fecal, desquamated epithelial cells, sweat)
- Women: ~1.3 mg/day average (+ menstrual losses of ~0.5-1 mg/day)
- Pregnancy: up to 5-6 mg/day in the 2nd-3rd trimesters (fetal loading + expanded red cell mass)
Because excretion cannot be regulated, absorption is the sole control point for iron homeostasis.
11. Hereditary Hemochromatosis - When Regulation Fails
Mutations in HFE, TfR2, HJV (hemojuvelin), or hepcidin (HAMP) impair the iron-sensing signals that stimulate hepcidin, resulting in low circulating hepcidin and unchecked ferroportin activity:
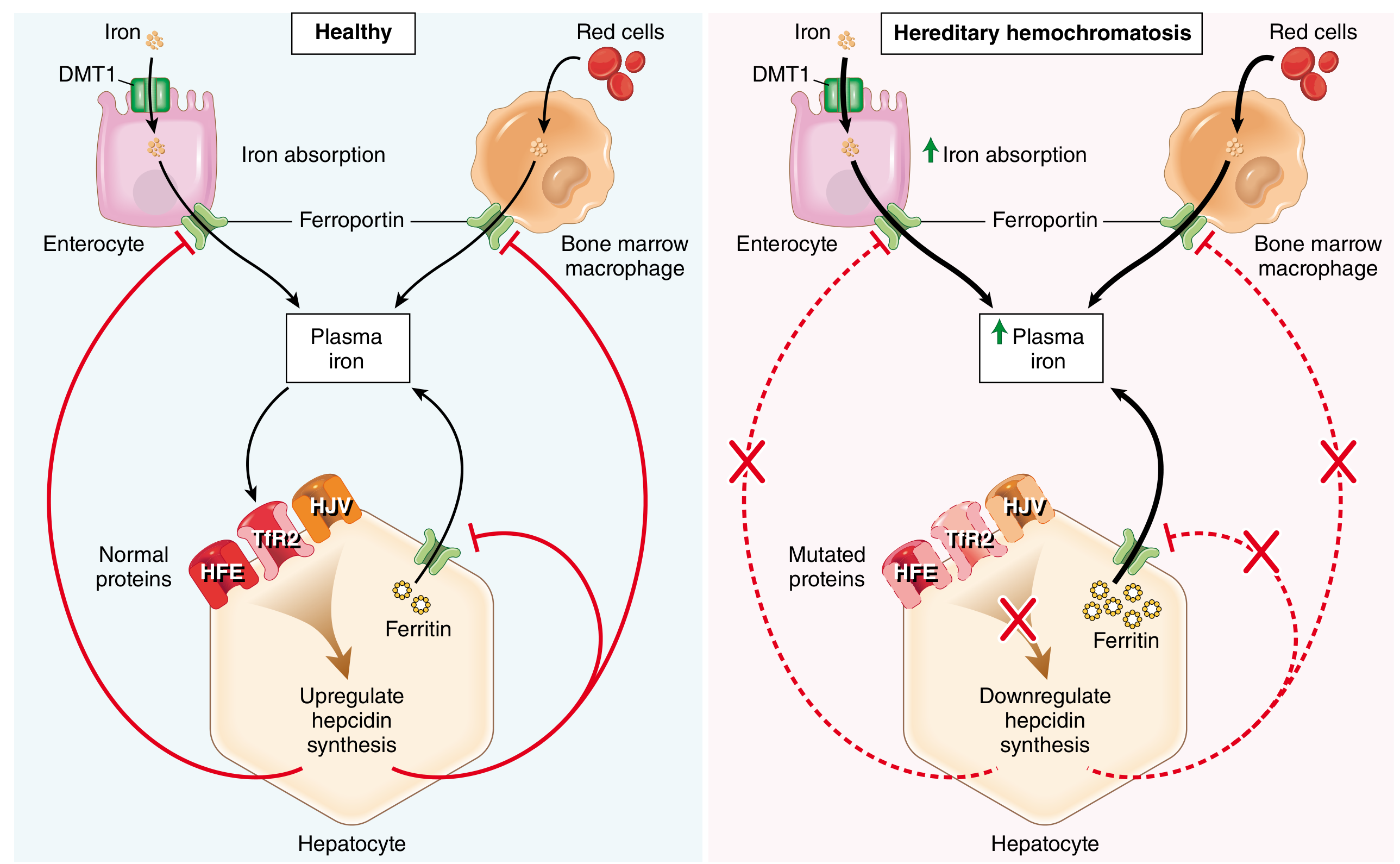
In HH: mutated HFE/HJV/TfR2 cannot signal hepcidin synthesis; ferroportin runs unchecked → systemic iron accumulation at 0.5-1 g/year → disease manifests after ~20 g stored iron.
Iron accumulation causes organ damage via:
- Lipid peroxidation (iron-catalyzed Fenton reaction → ROS)
- Activation of hepatic stellate cells → collagen formation → cirrhosis
- DNA damage → hepatocellular carcinoma risk
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 788
12. Daily Iron Requirements Summary
| Group | Daily requirement |
|---|---|
| Adult male | ~13 µg/kg (~1 mg/day) |
| Menstruating female | ~21 µg/kg (~1.4 mg/day) |
| Pregnancy (2nd-3rd trimester) | ~80 µg/kg (~5-6 mg/day) |
| Infant | ~67 µg/kg |
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, p. 928
Key take-home points:
- Iron is always protein-bound - free iron is toxic (Fenton chemistry)
- The body conserves iron tightly; 80-90% of daily needs come from macrophage recycling of old RBCs
- Hepcidin-ferroportin is the master regulatory axis at the systemic level
- IRP-IRE system handles cell-level iron sensing
- Absorption is the only adjustable output - there is no regulated excretion
- DMT1 (apical uptake) and ferroportin (basolateral export) are the critical transport proteins in the intestinal enterocyte
Vitamin a, d , c , b12 biochemistry mbbs
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Here is the complete MBBS-level biochemistry of all four vitamins, drawn from Robbins Pathology, Harper's Illustrated Biochemistry, Harrison's Principles, Goodman & Gilman, and Fitzpatrick's Dermatology.
Vitamins A, D, C, and B12 - Biochemistry (MBBS)
VITAMIN A (RETINOL)
Nature and Forms
Vitamin A is a fat-soluble vitamin that exists in several interconvertible forms:
| Form | Source/Role |
|---|---|
| Retinol (all-trans) | Alcohol form; transport and storage |
| Retinal (retinaldehyde) | Aldehyde form; required for vision |
| Retinoic acid | Acid form; gene regulation, differentiation |
| Retinyl esters | Storage form in liver |
| β-carotene | Plant precursor (provitamin A); 1 molecule → 2 retinol |
Dietary Sources and Absorption
- Preformed vitamin A (retinyl esters): liver, egg yolk, dairy, fish liver oils
- Provitamin A (β-carotene): yellow/orange vegetables, dark leafy greens
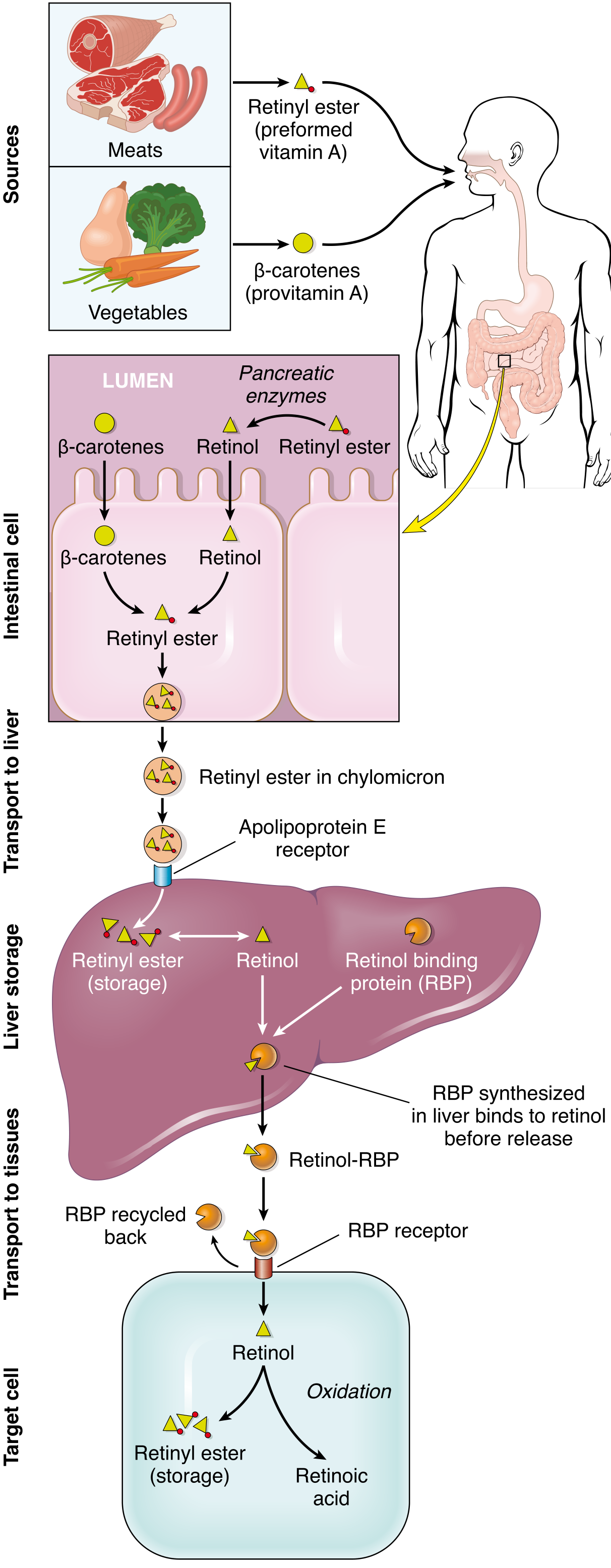
Vitamin A metabolism - Robbins, Cotran & Kumar Pathologic Basis of Disease
Absorption steps:
- Pancreatic enzymes hydrolyze retinyl esters → retinol in the intestinal lumen
- β-carotene is cleaved by intestinal β-carotene dioxygenase → retinal → retinol
- Retinol is re-esterified in enterocytes → incorporated into chylomicrons
- Chylomicrons are taken up by the liver (via ApoE receptors)
- Liver stores retinyl esters in perisinusoidal stellate (Ito) cells (90% of body stores)
- Body stores are sufficient for at least 6 months in a well-nourished individual
Transport
- Retinol is released from liver bound to Retinol-Binding Protein (RBP) - a hepatic protein
- The retinol-RBP complex circulates and delivers retinol to peripheral tissues via RBP receptors on cell surfaces
- RBP is a negative acute phase protein - synthesis falls during infection (important mechanism of deficiency exacerbation)
Functions
1. Vision (Rhodopsin Cycle)
The most well-known function:
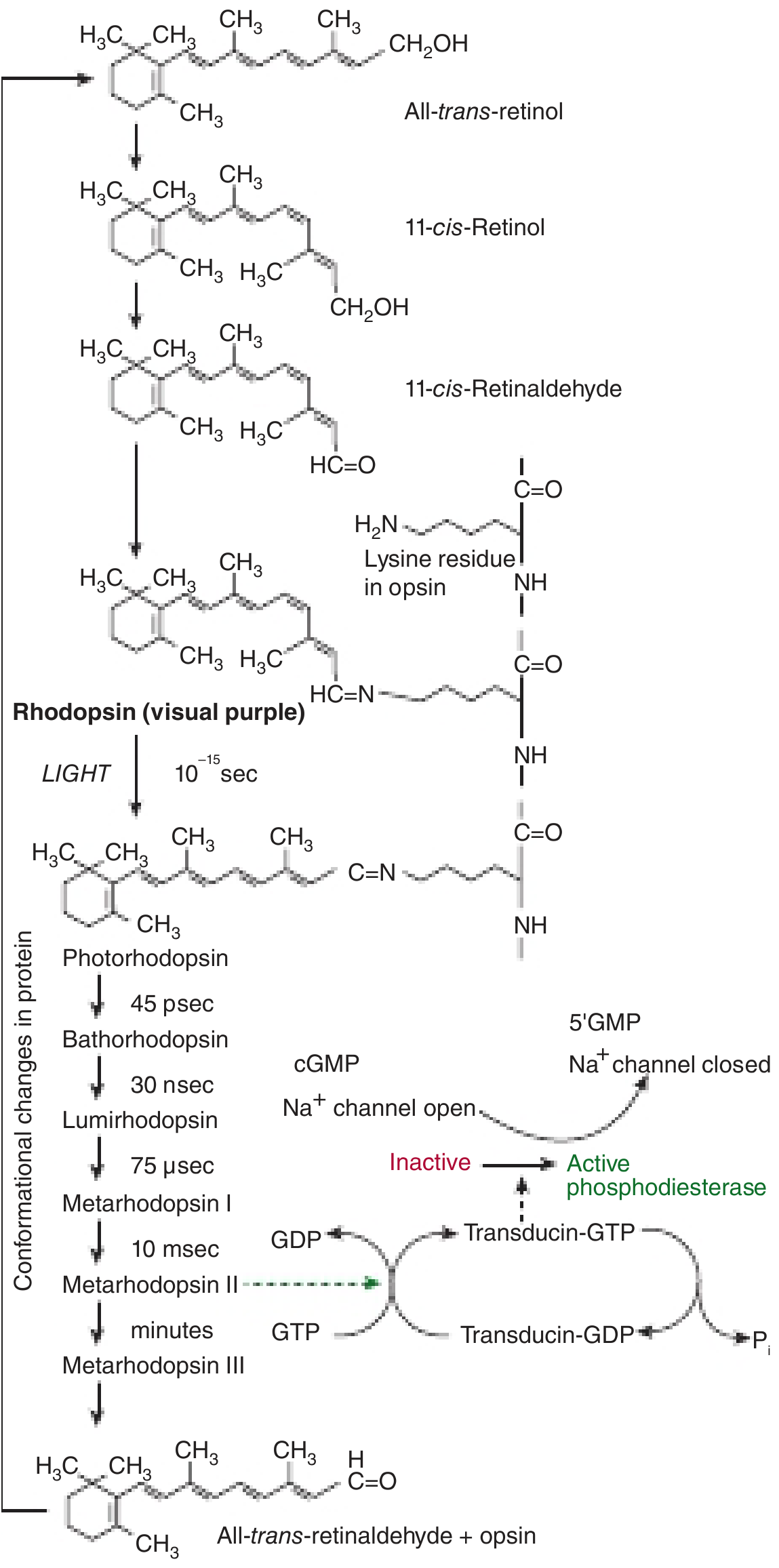
Rhodopsin visual cycle - Harper's Illustrated Biochemistry 32nd Ed
Steps:
- All-trans-retinol → isomerized to 11-cis-retinol
- Oxidized to 11-cis-retinal
- Covalently combines with opsin (7-transmembrane rod protein) → forms rhodopsin (visual purple)
- A photon of light causes 11-cis-retinal → all-trans-retinal (isomerization in 10⁻¹⁵ seconds)
- This dissociates from opsin → conformational change in opsin → activates transducin (G-protein) → activates phosphodiesterase → cGMP → 5'-GMP → Na⁺ channels close → hyperpolarization → nerve impulse
- During dark adaptation, some all-trans-retinal is reconverted to 11-cis-retinal; remainder is reduced to retinol and lost from retina - explaining continuous supply requirement
Four visual pigments:
- Rhodopsin (rods) - low-light / scotopic vision
- Three iodopsins (cones) - color / photopic vision, each responsive to different wavelengths
2. Epithelial Cell Differentiation and Growth
- Retinoic acid (RA) binds Retinoic Acid Receptors (RARs) - nuclear receptors
- RAR forms obligatory heterodimers with RXR (Retinoid X Receptor); both have α, β, γ isoforms
- RAR/RXR heterodimers bind Retinoic Acid Response Elements (RAREs) in gene promoters
- Regulates genes encoding: growth factor receptors, tumor suppressors, secreted proteins
- Without adequate retinoic acid → mucus-secreting epithelium undergoes squamous metaplasia (keratinizing transformation)
3. Immune Function
- Required for differentiation of immune system cells
- Vitamin A supplementation reduces mortality from diarrheal diseases by ~28%
4. Metabolic Effects (RXR Heterodimers)
- RXR (activated by 9-cis-retinoic acid) forms heterodimers with:
- Vitamin D receptor
- PPARγ (Peroxisome Proliferator-Activated Receptor γ) → regulates adipogenesis, lipid metabolism
- Drug-metabolizing nuclear receptors
5. Clinical Use of Retinoids
- Acne, psoriasis (13-cis-retinoic acid / isotretinoin)
- Acute Promyelocytic Leukemia (APL): All-trans-retinoic acid (ATRA) binds PML-RARα fusion protein → induces differentiation and apoptosis of leukemic cells
- Neuroblastoma recurrence prevention (13-cis-retinoic acid)
Deficiency
Most common cause: Primary malnutrition worldwide; also malabsorption of fats
Sequence of ocular changes:
- Loss of sensitivity to green light
- Night blindness (nyctalopia) - earliest sign
- Xerophthalmia - dryness of conjunctiva (Bitot's spots - foamy, silvery-grey deposits)
- Keratomalacia - corneal softening and ulceration → irreversible blindness
Vitamin A deficiency is the most important preventable cause of blindness worldwide.
Systemic changes:
- Squamous metaplasia of respiratory, GI, urinary tract epithelium
- Increased susceptibility to infections
- Impaired growth
Toxicity (Hypervitaminosis A)
-
CNS: headache, nausea, ataxia, increased CSF pressure
-
Liver: hepatomegaly, hyperlipidemia
-
Bone: thickening of long bones, hypercalcemia
-
Skin: dryness, desquamation, alopecia
-
Teratogenic in pregnancy - causes neural tube defects
-
Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 416
-
Harper's Illustrated Biochemistry 32nd Ed, p. 547
VITAMIN D (CALCIFEROL)
Nature - "More Hormone Than Vitamin"
Vitamin D is technically not a true vitamin because it can be synthesized endogenously in the skin. It functions as a steroid hormone.
Two major forms:
- Vitamin D₃ (cholecalciferol) - synthesized in skin / from animal food
- Vitamin D₂ (ergocalciferol) - from plant/fungal sources (ergosterol); used in food fortification
Synthesis and Metabolism
Step 1 - Skin synthesis:
- 7-dehydrocholesterol (cholesterol precursor in skin) absorbs UV radiation (280-315 nm)
- Undergoes non-enzymatic photolysis → previtamin D
- Previtamin D undergoes spontaneous thermal isomerization over hours → cholecalciferol (Vitamin D₃)
- Absorbed into bloodstream; plasma levels peak at end of summer, lowest at end of winter
- Beyond ~40° latitude, UV radiation is insufficient in winter
Step 2 - Liver (25-hydroxylation):
- Cholecalciferol → calcidiol [25-hydroxycholecalciferol / 25(OH)D₃]
- Enzyme: calciol-25-hydroxylase (CYP2R1)
- Released into circulation bound to Vitamin D-Binding Globulin (VDBG) - the main circulating storage form
- 25(OH)D is the best indicator of vitamin D status in blood tests
Step 3 - Kidney (1α-hydroxylation → active form):
- Calcidiol → calcitriol [1,25-dihydroxycholecalciferol / 1,25(OH)₂D₃]
- Enzyme: calcidiol-1α-hydroxylase (CYP27B1) - the key regulated step
- OR: 24-hydroxylation → 24,25-dihydroxyvitamin D (inactive/inactivation pathway)
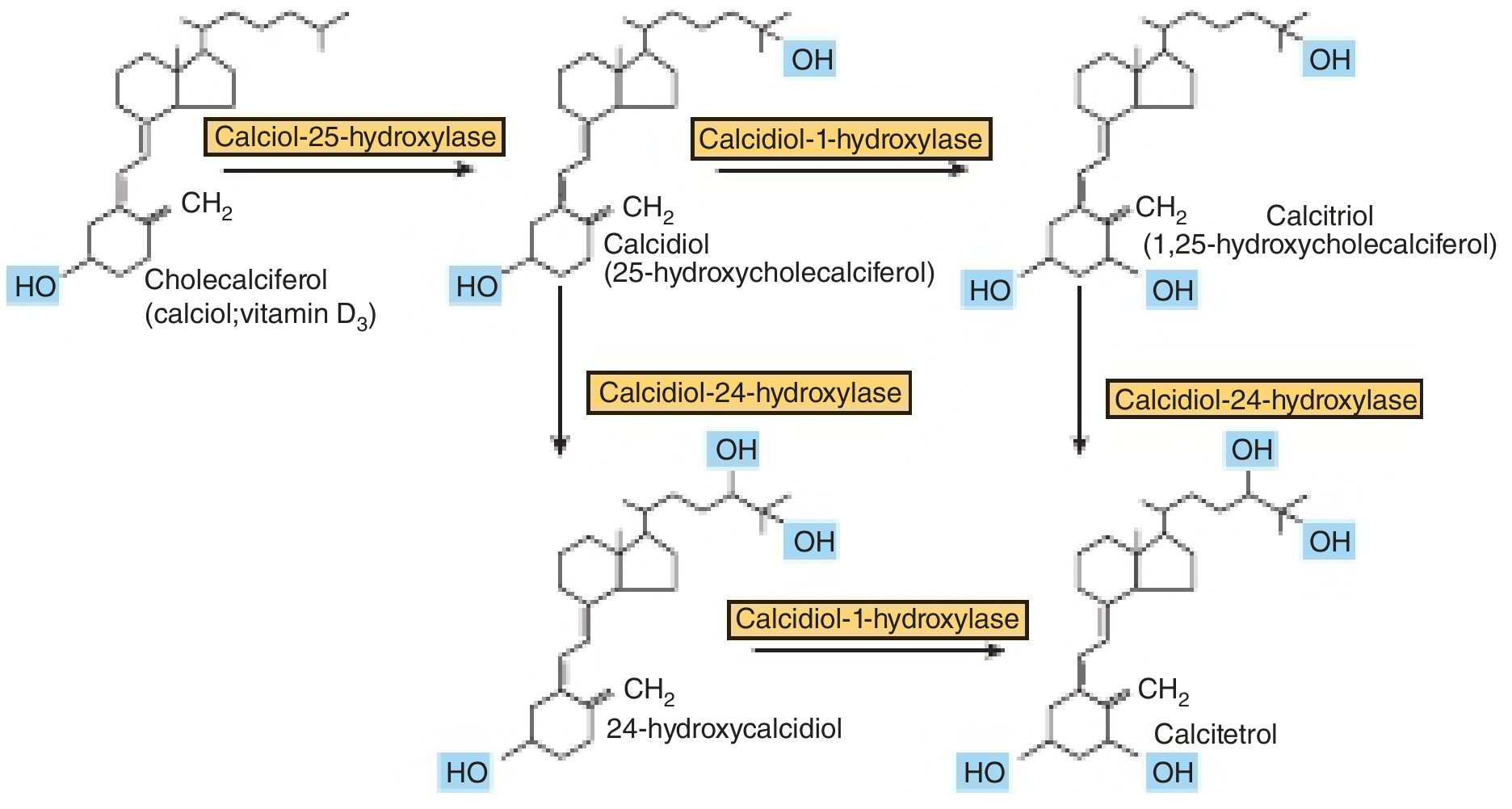
Vitamin D metabolism pathway - Harper's Illustrated Biochemistry 32nd Ed, p. 550
Regulation of Calcitriol Synthesis
| Factor | Effect on 1α-hydroxylase | Effect on calcitriol |
|---|---|---|
| Low serum calcium | ↑ | ↑ (indirect via PTH) |
| PTH | ↑ | ↑ |
| Low phosphate | ↑ | ↑ |
| High calcitriol (feedback) | ↓ (induces 24-hydroxylase) | ↓ |
| High calcium/phosphate | ↓ | ↓ |
| FGF-23 (from bone) | ↓ | ↓ |
Mechanism of Action
Calcitriol acts like a steroid hormone:
- Binds Vitamin D Receptor (VDR) - a nuclear receptor
- VDR heterodimerizes with RXR
- Binds Vitamin D Response Elements (VDREs) → regulates gene transcription
- Also has rapid non-genomic effects (membrane transporters)
Functions of Calcitriol - Maintaining Plasma Calcium
Three key actions:
- ↑ Intestinal calcium absorption (by inducing calbindin D - a calcium transport protein)
- ↑ Renal calcium reabsorption (distal tubule)
- ↑ Bone mineral mobilization (with PTH)
Other functions:
- Insulin secretion and synthesis
- Differentiation of monocyte precursors
- Inhibition of T-lymphocyte interleukin production (immunomodulation)
- Inhibition of B-lymphocyte immunoglobulin synthesis
- Regulation of parathyroid and thyroid hormone synthesis
- Cell proliferation inhibition - protective against colorectal and prostate cancer
Deficiency
Pathophysiology:
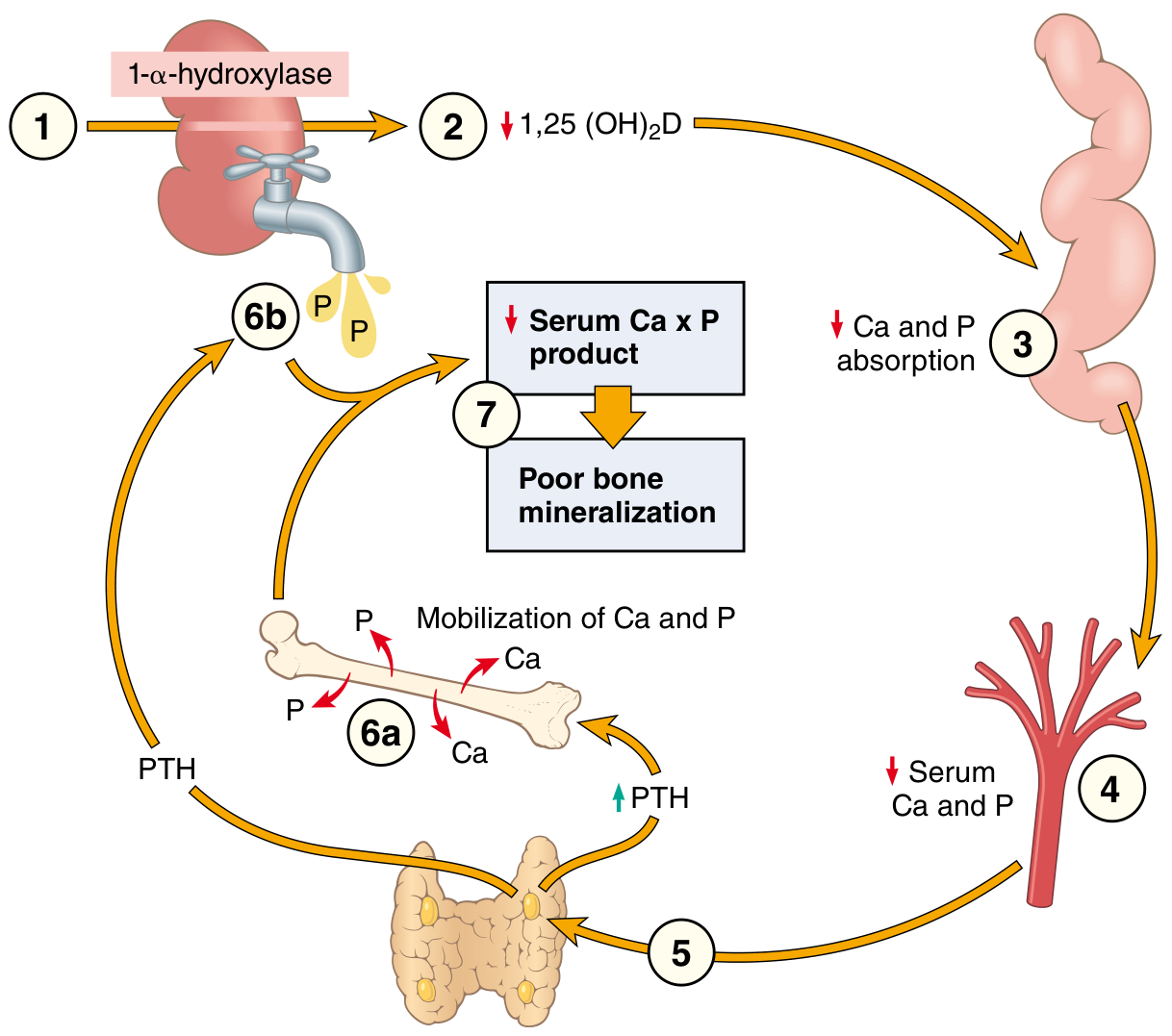
Vitamin D deficiency consequences - Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 420
| Age | Disease | Features |
|---|---|---|
| Children | Rickets | Failure of bone mineralization in growing skeleton |
| Adults | Osteomalacia | Demineralization of formed bone; bone pain, pseudofractures |
Rickets - skeletal changes:
- Craniotabes (softened occipital/parietal bones)
- Frontal bossing, squared head
- Rachitic rosary (beaded costochondral junctions)
- Pigeon breast deformity (anterior sternal protrusion)
- Harrison sulcus
- Bow legs (genu varum) in ambulatory children
- Delayed fontanelle closure
Lab findings: normal or slightly low serum Ca, low serum phosphate, elevated PTH, elevated alkaline phosphatase
Toxicity
-
Hypercalcemia → contraction of blood vessels, hypertension
-
Calcinosis (soft tissue calcification)
-
Some infants are sensitive at doses as low as 50 µg/day
-
Note: excess sunlight does NOT cause toxicity (limited 7-dehydrocholesterol production; previtamin D is photo-degraded)
-
Harper's Illustrated Biochemistry 32nd Ed, pp. 549-551
-
Robbins, Cotran & Kumar Pathologic Basis of Disease, pp. 419-420
VITAMIN C (ASCORBIC ACID)
Nature
- Water-soluble vitamin
- L-ascorbic acid; most animals synthesize it endogenously from glucose
- Humans, other primates, and guinea pigs lack L-gulonolactone oxidase - the enzyme for the final step → entirely dependent on diet
- Humans are unique in this deficit among large mammals
Sources
- Citrus fruits, kiwi, guava, strawberries, bell peppers, tomatoes, broccoli
- Liver, fish; present in milk (but lost on prolonged storage/heating)
Biochemical Functions
1. Collagen Synthesis (PRIMARY AND MOST IMPORTANT)
- Vitamin C activates prolyl hydroxylase and lysyl hydroxylase enzymes
- These enzymes hydroxylate proline → hydroxyproline and lysine → hydroxylysine in procollagen
- Hydroxyproline is essential for the triple-helix stability of collagen
- Hydroxylysine is essential for cross-linking of collagen fibrils
- Without hydroxylation: procollagen cannot form a stable helix → inefficiently secreted → lacks tensile strength → more soluble → vulnerable to degradation
- Collagen, which has the highest hydroxyproline content of any protein, is most affected - especially in blood vessels
Mechanism of hydroxylase activation: Vitamin C keeps the iron in the enzyme active site in the Fe²+ (ferrous) form - the active form. Without vitamin C, Fe²+ is oxidized to Fe³+ → enzyme inactive.
2. Neurotransmitter Synthesis
- Required for dopamine β-hydroxylase - hydroxylates dopamine → norepinephrine
3. Antioxidant Function
- Acts as a reducing agent (electron donor)
- Regenerates vitamin E from the tocopheryl radical
- Reduces oxidized iron (Fe³+ → Fe²+) in the gut, enhancing non-heme iron absorption
- Quenches reactive oxygen species and free radicals
4. Bile Acid Synthesis
- Required for 7α-hydroxylation of cholesterol (first step in bile acid synthesis)
5. Carnitine Synthesis
- Required for hydroxylation steps in carnitine biosynthesis
Deficiency - SCURVY
Classic findings result from defective collagen:
| System | Features |
|---|---|
| Gums | Swollen, spongy, bleeding gums (gingivitis); loose teeth |
| Skin | Perifollicular hemorrhages; corkscrew hairs (pathognomonic); ecchymoses |
| Bones | Subperiosteal hemorrhages; "scorbutic rosary" in children; Trümmerfeld zone (zone of rarefaction) |
| Joints | Hemarthroses |
| Systemic | Poor wound healing; fatigue; emotional lability |
| Children | Fröhlich syndrome - Frankel sign on X-ray |
Histology of scurvy:
- Perifollicular hemorrhages in dermis
- Hemosiderin deposits
- Bones show fractures at growth plate (Trümmerfeld zone) and subperiosteal hemorrhages
At-risk populations:
- Elderly living alone
- Persons with alcohol use disorder
- Patients on peritoneal dialysis / hemodialysis
- Infants on evaporated milk without supplementation
- Food faddists
Toxicity
-
Megadose vitamin C has not been proven to prevent colds in controlled trials
-
Mild antihistamine action may give some relief
-
Excess can cause: oxalate kidney stones, GI upset, interference with B12 absorption
-
Robbins, Cotran & Kumar Pathologic Basis of Disease, pp. 419-422
-
Guyton and Hall Textbook of Medical Physiology
VITAMIN B12 (COBALAMIN)
Structure and Chemistry
- Water-soluble vitamin with the most complex structure of all vitamins
- Contains a corrin ring (similar to porphyrin) with a cobalt atom at the center
- The cobalt atom forms a coordination bond with a cyanide, methyl, adenosyl, or hydroxyl group
Active coenzyme forms:
| Form | Enzyme | Reaction |
|---|---|---|
| Methylcobalamin | Methionine synthase | Homocysteine → Methionine |
| 5'-deoxyadenosylcobalamin (AdoB12) | Methylmalonyl-CoA mutase | Methylmalonyl-CoA → Succinyl-CoA |
Sources and Requirements
- Found exclusively in animal products: liver, organ meats, eggs, milk, beef, shellfish
- Strict vegans and breastfed infants of vegan mothers are at high risk
- Daily requirement: ~2.4 µg/day in adults
Absorption - The Intrinsic Factor Pathway (Key Exam Topic)
A multi-step process requiring several proteins:
- Stomach: Gastric acid and pepsin release B12 from food proteins → B12 binds R-binders (haptocorrins) secreted by salivary glands and gastric mucosa
- Duodenum: Pancreatic proteases digest R-binders → free B12 is then bound by Intrinsic Factor (IF) - a glycoprotein secreted by gastric parietal cells
- Terminal Ileum: The IF-B12 complex binds cubilin-amnionless receptors (CUBAM receptors) on ileal enterocytes → receptor-mediated endocytosis
- Enterocyte: B12 dissociates from IF → enters portal circulation bound to Transcobalamin II (TC-II) → delivered to all tissues
- 1-5% passive absorption occurs along entire intestine (important for pharmacological oral dosing)
Body stores: 2-5 mg (mainly liver) - sufficient for 3-6 years; this is why deficiency takes years to develop after dietary cessation
Biochemical Reactions
Reaction 1: Homocysteine → Methionine
- Enzyme: Methionine synthase
- Coenzyme: Methylcobalamin (methyl group donor)
- Co-substrate: N5-methyltetrahydrofolate (N5-methyl-THF) donates the methyl group to cobalamin → regenerates THF
- Products: Methionine + THF
Clinical significance of this reaction:
- Methionine is required for DNA synthesis, protein synthesis, lipid methylation
- THF regeneration is essential for purine/pyrimidine synthesis (DNA)
- B12 deficiency → THF is "trapped" as N5-methyl-THF (methylfolate trap) → functional folate deficiency → megaloblastic anemia (identical to folate deficiency anemia)
- Elevated homocysteine (risk factor for cardiovascular disease and neural tube defects)
Reaction 2: Methylmalonyl-CoA → Succinyl-CoA
- Enzyme: Methylmalonyl-CoA mutase
- Coenzyme: 5'-deoxyadenosylcobalamin
- Succinyl-CoA enters the TCA cycle
- B12 deficiency → methylmalonic acid (MMA) accumulates
- Abnormal fatty acids are incorporated into myelin → Subacute Combined Degeneration (SACD) of the spinal cord
Causes of Deficiency
| Category | Examples |
|---|---|
| Inadequate intake | Strict veganism, malnutrition, eating disorders |
| ↓ Intrinsic factor | Pernicious anemia (autoimmune), atrophic gastritis, total gastrectomy, gastric bypass |
| Malabsorption at terminal ileum | Crohn's disease, ileal resection, celiac disease, Whipple disease |
| Competing organisms | Bacterial overgrowth, fish tapeworm (Diphyllobothrium latum) |
| ↓ Gastric acid | Chronic PPI/H2-blocker use (B12 stays food-bound) |
| Drug-induced | Metformin (inhibits TC-II absorption); Nitrous oxide (irreversibly oxidizes cobalamin) |
| Inborn errors | Transcobalamin II deficiency |
Pernicious Anemia:
- Autoimmune gastritis → destruction of gastric parietal cells
- Anti-parietal cell antibodies (~90% sensitive) and anti-intrinsic factor antibodies (~60% sensitive)
- Leads to achlorhydria + absent IF
Clinical Features of B12 Deficiency
1. Hematological
- Megaloblastic anemia (due to methylfolate trap → impaired DNA synthesis → delayed nuclear maturation with normal cytoplasmic development)
- Macrocytic anemia (MCV >100 fL)
- Hypersegmented neutrophils (≥5 lobes) - pathognomonic
- Pancytopenia in severe cases
2. Neurological - SACD (Subacute Combined Degeneration)
- Demyelination of the posterior columns (vibration, proprioception loss, sensory ataxia) and lateral columns (corticospinal tract - upper motor neuron signs)
- First symptoms: Numbness/tingling in hands, then lower extremities
- Impaired vibration and proprioception (large fiber loss) with preserved pain/temperature (small fiber spared)
- Unsteady gait, Romberg positive
- Hyperreflexia + absent Achilles reflex (a mixed picture)
- Optic atrophy (less common)
- Behavioral changes: irritability, forgetfulness, dementia, psychosis ("megaloblastic madness")
- CRITICAL POINT: Neurological damage can occur even WITHOUT anemia (in ~40% of cases)
- Giving folate alone to a B12-deficient patient corrects anemia but allows neurological damage to progress - a clinical danger
3. Other
- Glossitis (smooth, beefy-red "Hunter's glossitis")
- Elevated serum homocysteine AND methylmalonic acid (MMA) - both elevated distinguishes B12 from folate deficiency (folate deficiency only elevates homocysteine, NOT MMA)
Diagnosis
| Test | Finding in B12 Deficiency |
|---|---|
| Serum B12 | Low (<200 pg/mL) |
| MCV | Elevated (>100 fL) |
| Blood film | Macrocytes, hypersegmented neutrophils |
| Serum homocysteine | Elevated |
| Serum methylmalonic acid (MMA) | Elevated (specific for B12 deficiency) |
| Anti-IF antibodies | Positive in ~60% of pernicious anemia |
| Anti-parietal cell antibodies | Positive in ~90% of pernicious anemia |
| Schilling test | Distinguishes dietary vs. IF-related malabsorption |
Treatment
-
Pernicious anemia / IF deficiency: Intramuscular cyanocobalamin 1000 µg weekly × 4 weeks, then monthly lifelong
-
Dietary deficiency / food-cobalamin malabsorption: Oral B12 1000 µg/day (relies on passive absorption - 1-5%)
-
Neurological deficits: at least 50% of patients retain some permanent neurologic deficit even after treatment
-
Fitzpatrick's Dermatology, Volume 1, p. 2661
-
Harrison's Principles of Internal Medicine 22E, p. 3655
Quick Comparison Table (MBBS Exam Summary)
| Feature | Vitamin A | Vitamin D | Vitamin C | Vitamin B12 |
|---|---|---|---|---|
| Type | Fat-soluble | Fat-soluble (hormone) | Water-soluble | Water-soluble |
| Active form | Retinoic acid / Retinal | Calcitriol [1,25(OH)₂D₃] | L-ascorbic acid | Methylcobalamin / AdoB12 |
| Key enzyme | Retinal dehydrogenase | 1α-hydroxylase (kidney) | Prolyl hydroxylase | Methionine synthase / MMA mutase |
| Key receptor | RAR/RXR (nuclear) | VDR/RXR (nuclear) | No nuclear receptor | Coenzyme (direct) |
| Storage | Liver (Ito cells) 6 months | VDBG (calcidiol) | Minimal | Liver 3-6 years |
| Deficiency disease | Night blindness → Xerophthalmia | Rickets / Osteomalacia | Scurvy | Megaloblastic anemia + SACD |
| Key deficiency marker | Clinical (night blindness) | ↓ serum 25(OH)D, ↑ ALP | Clinical (perifollicular hemorrhage) | ↑ MMA + homocysteine |
| Classic sign | Bitot's spots | Rachitic rosary | Perifollicular hemorrhage; corkscrew hairs | Hypersegmented neutrophils |
| Toxicity | Yes (teratogenic) | Yes (hypercalcemia) | Rare (kidney stones) | None known |
| Transport protein | RBP | Vitamin D-binding globulin | Free in plasma | Transcobalamin II |
This is a shared conversation. Sign in to Orris to start your own chat.