Hymenolpsis nana
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information from multiple authoritative sources. Here is a complete summary:
Hymenolepis nana (Dwarf Tapeworm)
Nomenclature note: Recent molecular data have reclassified this organism to Rodentolepis nana (previously Hymenolepis nana) — Harrison's Principles of Internal Medicine 22E uses this new name, though H. nana remains widely used in clinical literature.
Classification
- Class: Cestoda (tapeworm)
- Common name: Dwarf tapeworm
- Unique distinction: The only human cestode that does not require an intermediate host to complete its life cycle
Morphology
| Feature | Detail |
|---|---|
| Adult length | 2–4 cm (some sources up to 40 mm) — "dwarf" compared to Taenia (several metres) |
| Scolex | 4 muscular suckers + crown of hooklets (rostellum) |
| Eggs | Oval, 30–47 µm, thin smooth outer shell; inner membrane with 4–8 polar filaments extending from two poles; contain a 6-hooked oncosphere (hexacanth embryo) |
Life Cycle
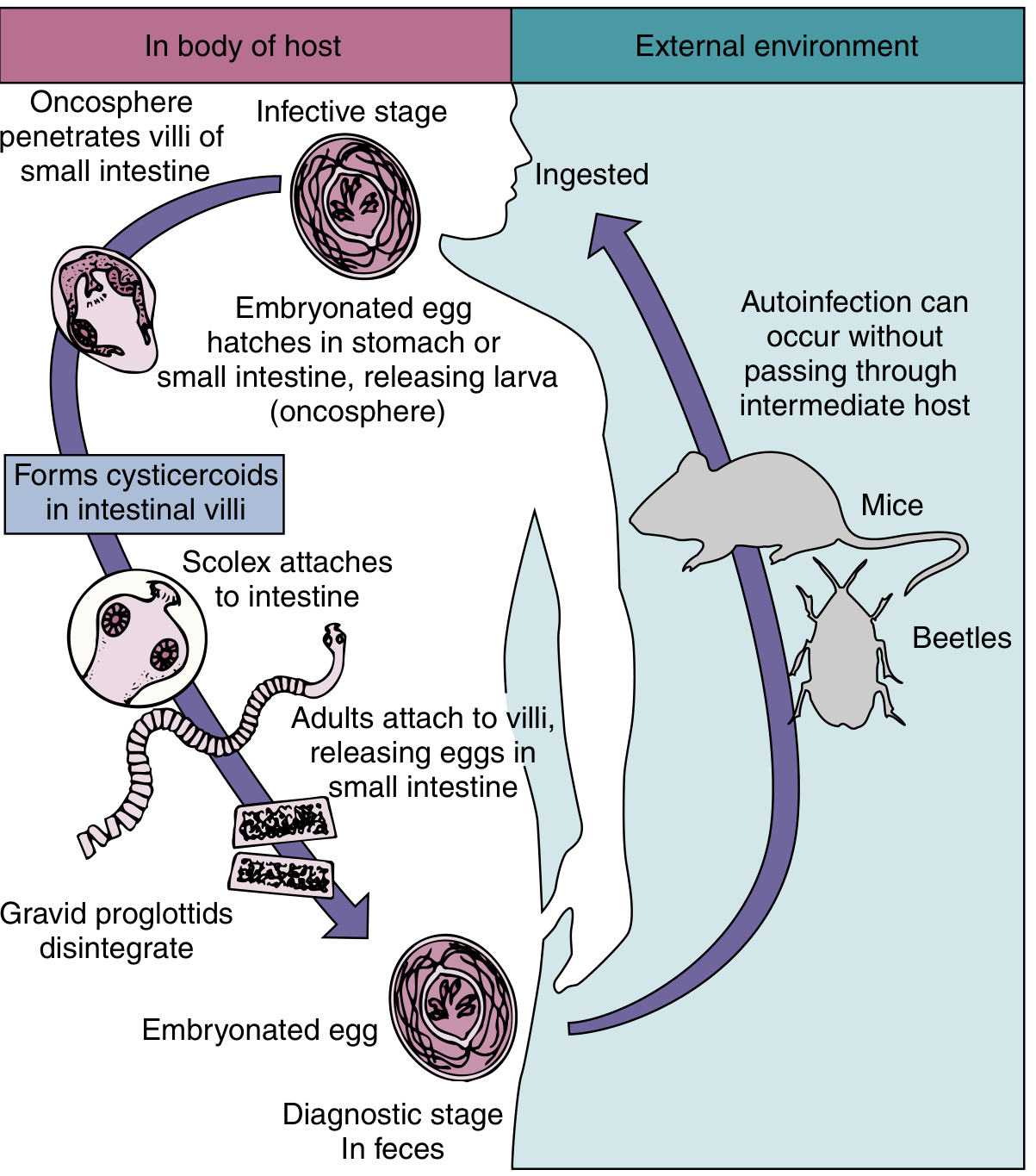
Life cycle of H. nana (dwarf tapeworm) — Medical Microbiology 9e
Three routes of infection:
- Direct (fecal-oral, no intermediate host) — Embryonated eggs ingested → oncosphere released → penetrates intestinal villi → develops into cysticercoid larva → re-enters intestinal lumen → scolex attaches to small intestinal mucosa → matures into adult in 10–12 days → gravid proglottids disintegrate in situ, releasing eggs into feces
- Via arthropod intermediate host — Accidental ingestion of infected beetles (contaminating grain/flour) containing cysticercoids
- Autoinfection (internal) — Eggs hatch within the intestinal lumen without leaving the host → new cysticercoids form → leads to hyperinfection with very heavy worm burdens
- Adult worm lifespan: ~4–10 weeks; infection perpetuated by repeated autoinfection cycles
Reservoir hosts: Mice (also beetles as intermediate hosts)
Epidemiology
- Most prevalent tapeworm infection worldwide: estimated 50–75 million cases globally
- Distribution: worldwide, including temperate and tropical regions
- Most common tapeworm infection in North America
- Highest risk: children, institutionalized patients, immunocompromised hosts
- Transmission: primarily person-to-person fecal-oral route; also via contaminated grain/flour containing infected beetles
- Capable of person-to-person spread (unlike most cestodes)
Clinical Features
| Worm burden | Symptoms |
|---|---|
| Light infection | Asymptomatic (most common) |
| Heavy infection / hyperinfection | Diarrhea, abdominal pain, anorexia, headache, weight loss, malabsorption |
Heavy infection is particularly seen in children harboring hundreds or thousands of worms, and in immunocompromised patients where autoinfection is less controlled.
Diagnosis
- Stool microscopy: Detection of characteristic eggs in wet mount of concentrated stool — oval, 30–47 µm, with polar filaments and a 6-hooked oncosphere inside
- More than one specimen may be required
- Culture, serology, antigen detection, and PCR are not routinely used
- Adult worms occasionally found during colonoscopy
Treatment
| Drug | Dose | Notes |
|---|---|---|
| Praziquantel (drug of choice) | 25 mg/kg once | Active against both adult worms and cysticercoids in the intestinal wall |
| Nitazoxanide (alternative) | 500 mg twice daily × 3 days | Alternative when praziquantel unavailable |
| Niclosamide | Standard dose | Alternative (older agent) |
Prevention & Control
- Hand hygiene (especially in households, schools, day-care centers)
- Improved sanitation
- Mass chemotherapy in epidemic settings
- Proper food storage to prevent beetle contamination of grain/flour
Sources: Medical Microbiology 9e | Harrison's Principles of Internal Medicine 22E | Goldman-Cecil Medicine | Tietz Textbook of Laboratory Medicine 7e
This is a shared conversation. Sign in to Orris to start your own chat.