Optical Coherence Tomography for 10 marks
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Searching Images
optical coherence tomography retinal layers OCT scan
I now have comprehensive content from multiple authoritative textbooks. Let me compile a thorough 10-mark answer.
Optical Coherence Tomography (OCT)
Definition and Principle
Optical coherence tomography (OCT) is a non-invasive, non-contact, high-resolution imaging technique that produces cross-sectional images of biological tissue — most notably the retina — using near-infrared light interferometry. It is analogous to B-scan ultrasonography, except that it uses light instead of sound waves. OCT achieves axial resolutions of 3–10 µm (far superior to ultrasound), enabling visualization of individual retinal layers in vivo.
"OCT is analogous to B-scan ultrasonography but uses near-infrared light interferometry rather than sound waves." — Kanski's Clinical Ophthalmology, 10th ed.
Physical Basis / How It Works
The instrument emits low-coherence near-infrared light (~820 nm for posterior segment; ~1310 nm for anterior segment) from a superluminescent diode. The light beam is split by a beam splitter (fibreoptic coupler):
- Half is directed toward the tissue
- Half toward a reference mirror
Reflected light from the tissue and reflected reference light are recombined in an interferometer. The echo time delay of the back-reflected signals is analyzed and translated into a high-resolution cross-sectional image (A-scan → multiple A-scans combined = B-scan).
The most highly reflective structures: nerve fiber layer (NFL), retinal pigment epithelium (RPE), hard exudates, scar tissue.
Low reflectivity is seen with: intraretinal fluid, subretinal fluid.
Low reflectivity is seen with: intraretinal fluid, subretinal fluid.
Generations of OCT Technology
| Type | Feature |
|---|---|
| Time Domain (TD-OCT) | Reference mirror moves mechanically; older, slower (~400 A-scans/sec); resolution ~10 µm |
| Spectral/Fourier Domain (SD-OCT) | No moving parts; simultaneous collection of all frequency data; faster (~25,000–70,000 A-scans/sec); resolution ~5–7 µm; now standard |
| Swept-Source OCT (SS-OCT) | Tunable laser light source; ultra-high speed; better choroidal penetration; resolution ~3 µm |
| Enhanced Depth Imaging (EDI-OCT) | Optimizes visualization of the choroid by positioning OCT image deeper |
Normal OCT Appearance of the Retina
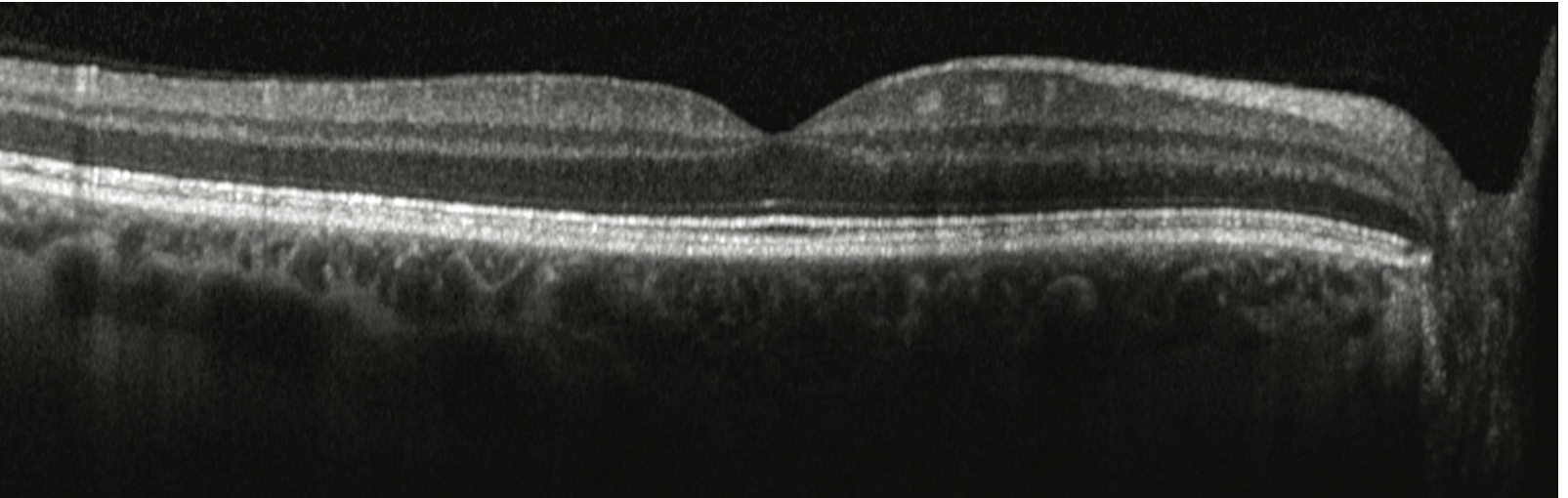
On a normal OCT scan, the following layers can be individually resolved (innermost to outermost):
- Internal limiting membrane (ILM)
- Retinal nerve fiber layer (RNFL)
- Ganglion cell layer (GCL)
- Inner plexiform layer (IPL)
- Inner nuclear layer (INL)
- Outer plexiform layer (OPL)
- Outer nuclear layer (ONL)
- External limiting membrane (ELM)
- Inner segment / outer segment junction (IS/OS = ellipsoid zone)
- Retinal pigment epithelium (RPE)
- Choroid (visible on SS-OCT/EDI)
The fovea appears as a central concavity with thinning of the inner retinal layers.
Clinical Applications in Ophthalmology
1. Macular Diseases
- Age-related macular degeneration (AMD): Detects drusen, geographic atrophy, pigment epithelial detachment (PED), and subretinal/intraretinal fluid in neovascular AMD; monitors treatment response to anti-VEGF therapy
- Diabetic macular edema (DME): Quantifies retinal thickness; detects cystoid spaces, hard exudates, and tractional components
- Central serous chorioretinopathy (CSCR): Identifies subretinal fluid, RPE detachment
- Macular hole: Stages holes (Gass classification) and assesses surgical outcomes
- Epiretinal membrane: Defines tractional interface, inner surface folds
- Vitreomacular traction (VMT): Visualizes vitreous attachment and degree of traction
2. Vitreoretinal Interface
- Macular holes, cysts, epiretinal membranes, vitreoretinal strands, subhyaloid hemorrhage
3. Glaucoma
- RNFL thickness measurement around the optic disc — gold standard for structural monitoring
- Ganglion cell complex (GCC) analysis at the macula
- Optic nerve head cup-to-disc ratio quantification
- Detects pre-perimetric glaucoma (structural damage before visual field loss)
4. Optic Nerve & Neuro-ophthalmology
- Optic neuritis / multiple sclerosis: RNFL thinning indicates retrograde axonal loss; used as a biomarker for MS progression
- Papilledema (disc edema): Quantifies NFL swelling
- Optic neuropathies (compressive, ischemic, hereditary — e.g., Leber's)
- Optic nerve drusen
5. Retinal Vascular Diseases
- Retinal vein occlusion (branch or central): Monitors macular edema
- Retinal artery occlusion: Demonstrates inner retinal hyperreflectivity (ischemic edema)
6. Anterior Segment OCT (AS-OCT)
- Uses 1310 nm wavelength
- Corneal mapping (e.g., Descemet membrane detachment)
- Angle anatomy in glaucoma (narrow angle, plateau iris)
- Anterior segment dysgenesis
- Post-surgical assessment (DSAEK, DMEK, LASIK flap)
OCT Angiography (OCTA)
A newer, non-invasive, dye-free technique that images retinal and choroidal blood flow without fluorescein or indocyanine green injection.
Principle: Repeated B-scans at the same location detect motion of red blood cells as a changing signal; static tissue produces no signal. This generates en-face maps of the microvasculature at different depth layers.
Applications:
- Neovascular AMD: Detects choroidal neovascularization (CNV), including non-exudative CNV
- Diabetic retinopathy: Identifies neovascularization, IRMA, foveal avascular zone (FAZ) enlargement, and microvascular changes even before clinical retinopathy
- Superficial and deep capillary plexi mapping
- Macular ischemia assessment
Limitations: Small field of view, cannot demonstrate leakage/staining/pooling (unlike FA), motion artifacts, requires good patient fixation.
Intravascular OCT (IV-OCT) — Cardiology Application
Used in coronary artery imaging via catheter:
- A single optical fiber is introduced into the coronary artery
- Provides image resolution of 12–20 µm axially (far superior to IVUS at ~100 µm)
- Identifies atherosclerotic plaque components: lipid (low-signal), fibrous cap (signal-rich), calcification (signal-poor with sharp borders)
- Detects thin-cap fibroatheroma (TCFA) — vulnerable plaques prone to rupture
- Guides PCI/stent deployment — assesses stent apposition, dissection, and tissue coverage
Limitation: Requires blood clearance (saline or contrast flush) as red blood cells attenuate the OCT signal.
Advantages of OCT
| Advantage | Detail |
|---|---|
| Non-invasive, non-contact | No dye injection needed (unlike FA/ICGA) |
| Ultra-high resolution | 3–10 µm; superior to all other in-vivo imaging |
| Objective & quantitative | Retinal thickness maps, RNFL measurements |
| Fast acquisition | SD-OCT captures full macular volumes in <2 sec |
| Repeatable | Ideal for longitudinal disease monitoring |
| No radiation | Safe for repeated use |
Limitations
- Media opacities (dense cataract, vitreous hemorrhage) reduce image quality
- Requires patient cooperation and fixation
- OCTA: Cannot show leakage; small field of view
- IV-OCT: Requires blood clearance; risk of contrast/saline flush
- Limited tissue penetration (cannot image through thick scarring or dense pigmentation)
Summary for 10 Marks
| Point | Key Fact |
|---|---|
| Principle | Near-IR interferometry; echo time delay of back-reflected light |
| Resolution | 3–10 µm axial (SD-OCT); superior to USG |
| Technology | TD-OCT → SD-OCT (standard) → SS-OCT (newest) |
| Normal retina | 10 distinct layers resolved; foveal pit visible |
| Macular disease | AMD, DME, macular hole, ERM, CSCR |
| Glaucoma | RNFL/GCC thickness; pre-perimetric detection |
| Neuro | RNFL as biomarker for MS; optic neuritis |
| AS-OCT | Cornea, anterior angle, post-surgical |
| OCTA | Non-invasive flow imaging; no dye needed |
| IV-OCT | Coronary plaque characterization; TCFA detection |
Sources: Kanski's Clinical Ophthalmology 10th ed. | The Wills Eye Manual | Fuster and Hurst's The Heart 15th ed.
This is a shared conversation. Sign in to Orris to start your own chat.