Explain me erythropoiesis in detail
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive, detailed information from multiple authoritative textbooks and excellent diagrams. Let me compile the full answer.
Erythropoiesis - A Detailed Explanation
Erythropoiesis is the process by which red blood cells (RBCs) are produced from pluripotent hematopoietic stem cells. It occurs primarily in the red bone marrow in adults (vertebrae, ribs, sternum, iliac crests, proximal femur/humerus). Under normal conditions, approximately 2.5 to 3.0 million erythrocytes are produced every second, replacing about 1% of the circulating RBC mass daily.
1. Sites of Erythropoiesis (Developmental Progression)
- Yolk sac (week 3-8 of embryonic life) - primitive erythropoiesis
- Liver and spleen (fetal period, weeks 6-28) - definitive erythropoiesis
- Bone marrow (from month 5 of fetal life onwards, and exclusively after birth)
In pathological states (e.g., myelofibrosis, severe thalassemia), the liver and spleen may resume erythropoiesis - this is called extramedullary erythropoiesis.
2. Stem Cell Hierarchy and Progenitor Stages
The progression begins with uncommitted multipotent stem cells and moves through increasingly committed progenitors:
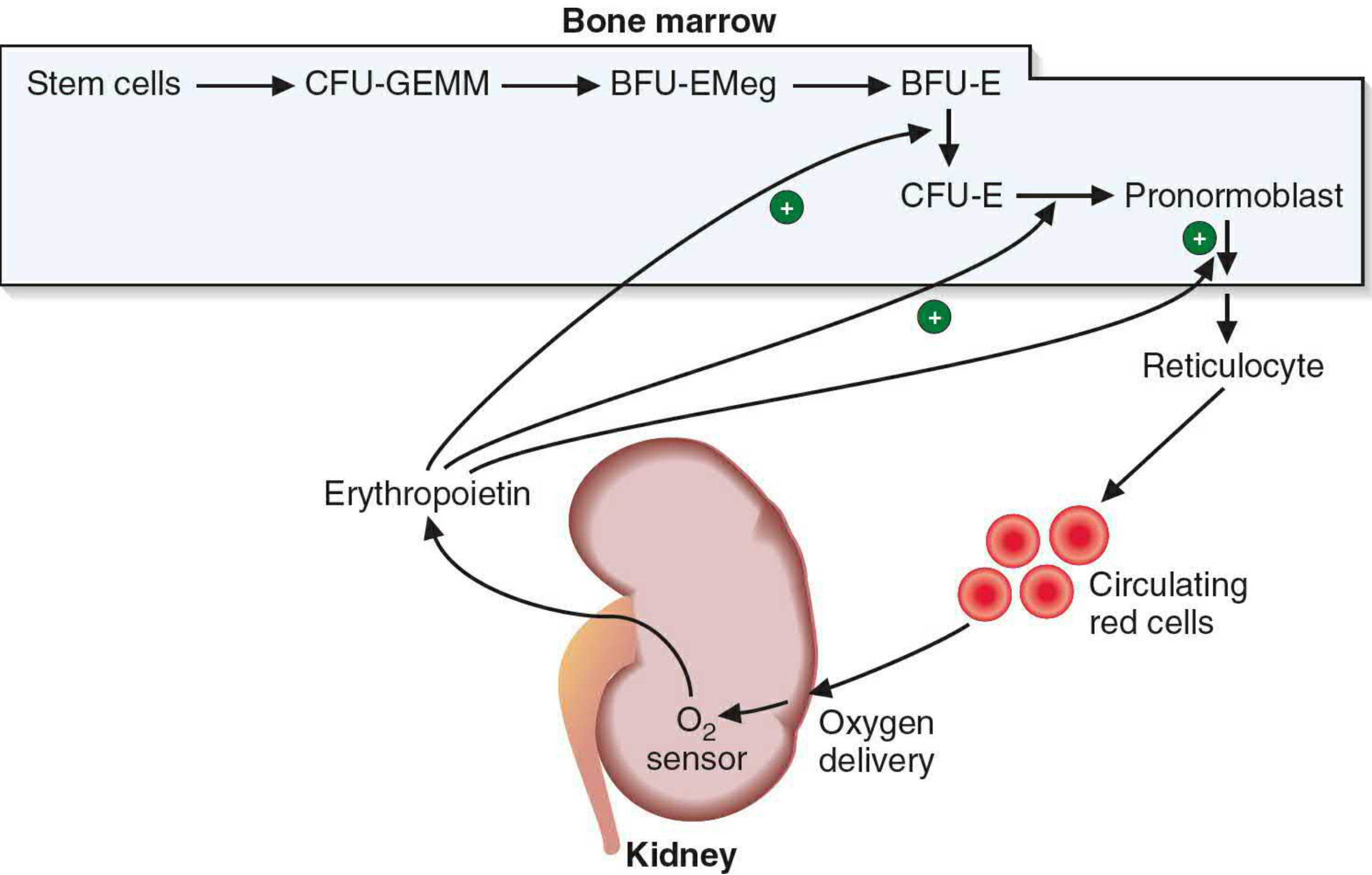
Erythropoietin stimulation of erythrocyte maturation. The kidney acts as an O₂ sensor, releasing EPO which drives progenitors toward the red cell lineage.
| Stage | Key Features |
|---|---|
| HSC (Hematopoietic Stem Cell) | Self-renewing, pluripotent |
| CMP (Common Myeloid Progenitor) | Commits to myeloid lineage |
| CFU-GEMM | Colony-forming unit: Granulocyte, Erythroid, Monocyte, Megakaryocyte |
| MEP | Megakaryocyte-Erythroid Progenitor |
| BFU-E | Burst-Forming Unit - Erythroid (EPO-insensitive initially) |
| CFU-E | Colony-Forming Unit - Erythroid (highly EPO-sensitive) |
| Proerythroblast | First morphologically recognizable erythroid cell |
The transcription factor GATA-1 is required for terminal differentiation of MEP cells into the definitive erythroid lineage. Additional regulatory signals include IL-3, IL-4, and, most importantly, erythropoietin (EPO).
3. Morphological Stages of Maturation (Normoblastic Series)
The key hallmark of maturation is: progressive nuclear condensation and extrusion + progressive hemoglobin accumulation + decreasing cell size + loss of ribosomes (RNA).
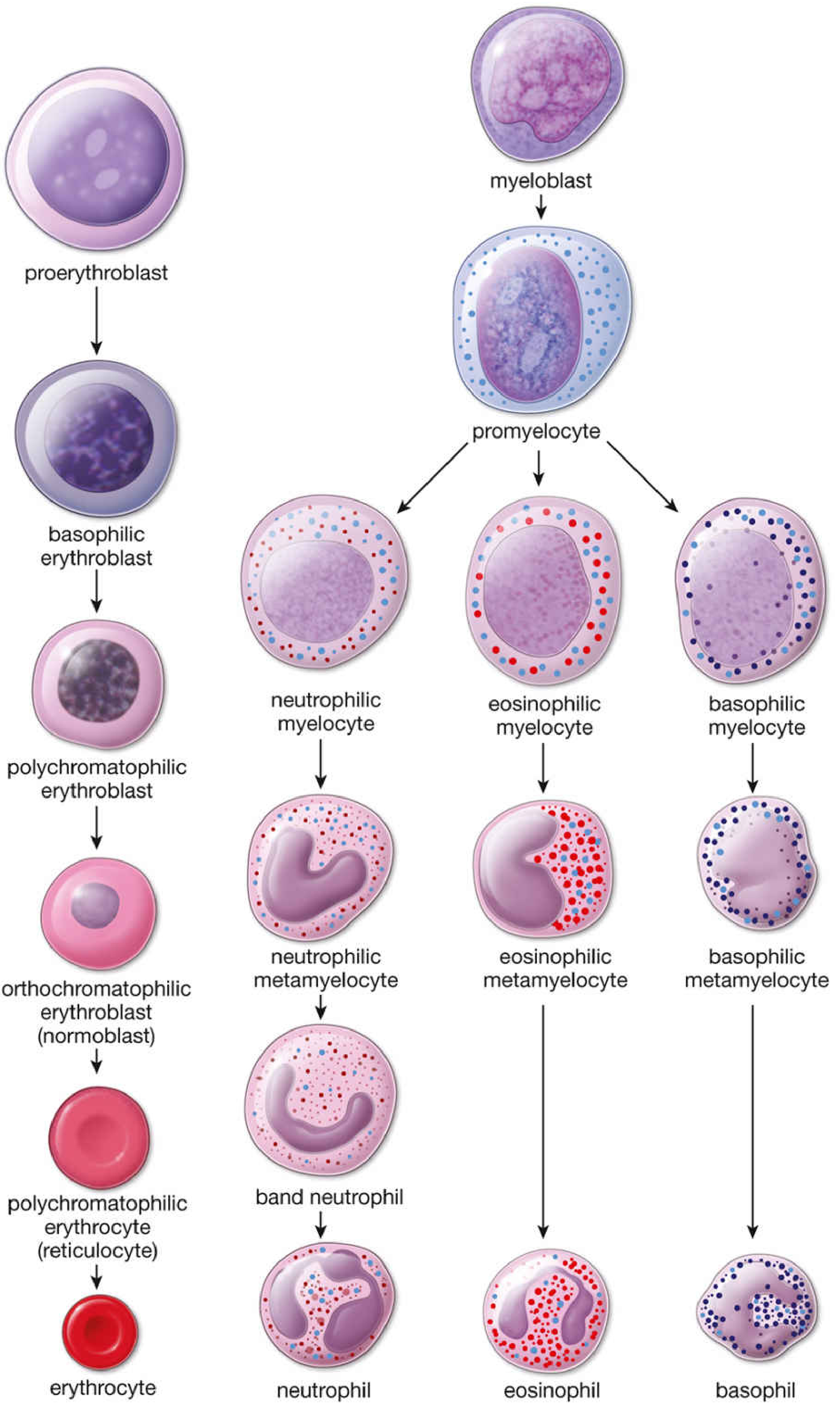
Normal human bone marrow stages of erythrocytic differentiation (left column), compared with granulocytic differentiation (right).
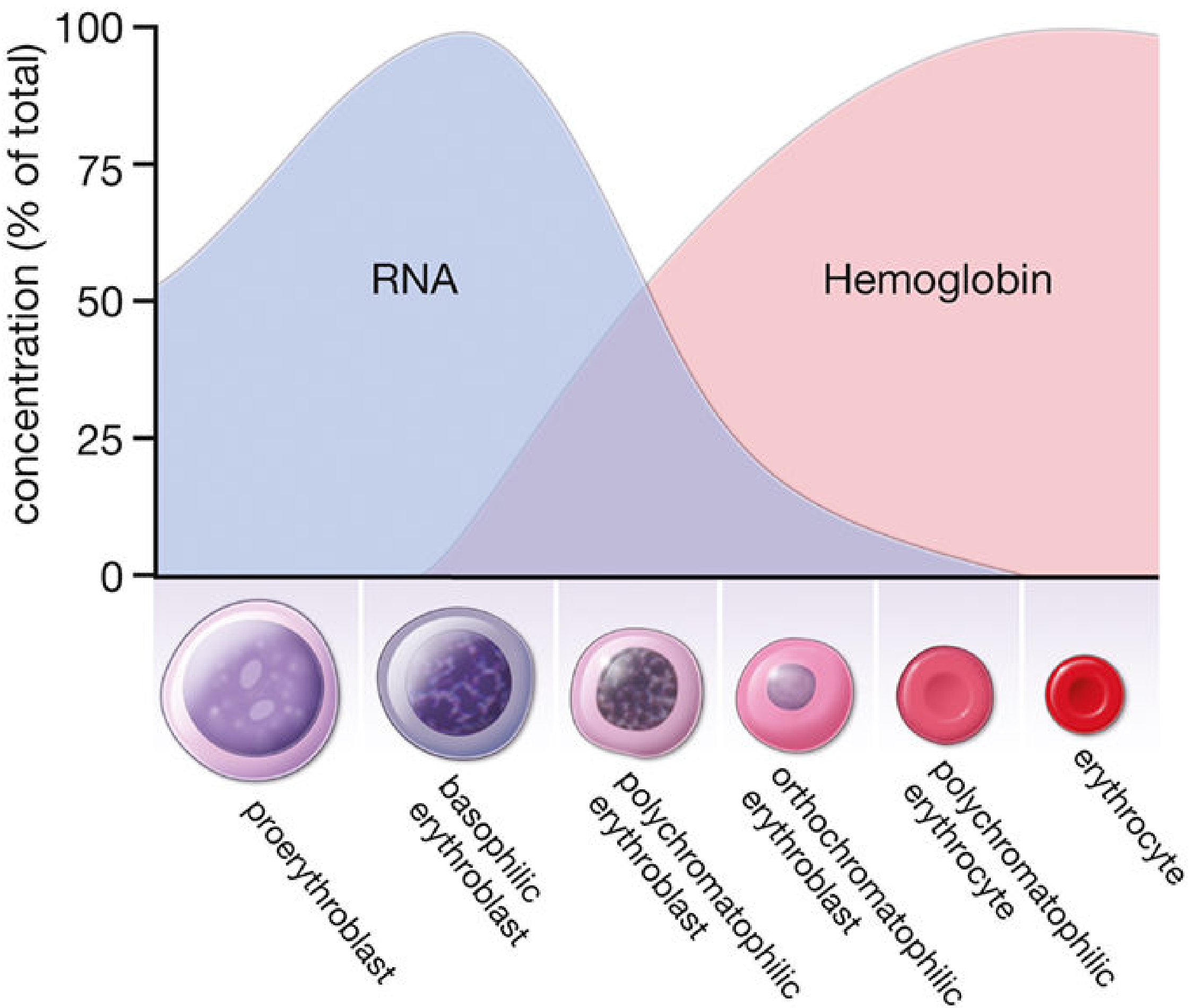
As erythropoiesis progresses, RNA (blue) peaks early then falls while hemoglobin (pink) rises progressively.
Stage 1: Proerythroblast (Pronormoblast)
- Size: 12-20 µm (the largest erythroid precursor)
- Nucleus: Large, round, with fine uniform chromatin; 1-2 prominent nucleoli; nuclear membrane well defined
- Cytoplasm: Moderate basophilia due to abundant free ribosomes; NO granules
- Function: Components for Hgb synthesis begin to accumulate; undergoes mitosis → 2 basophilic erythroblasts
- Duration: ~24 hours
Stage 2: Basophilic Erythroblast (Basophilic Normoblast)
- Size: 10-16 µm (smaller than proerythroblast)
- Nucleus: Smaller, progressively more heterochromatic; chromatin condenses with each mitosis; nucleoli disappear
- Cytoplasm: Deeply basophilic due to large numbers of polyribosomes actively synthesizing hemoglobin
- Key: RNA content is at its highest here (alongside the proerythroblast)
- Duration: ~24 hours; divides to form polychromatophilic erythroblasts
Stage 3: Polychromatophilic Erythroblast (Polychromatophilic Normoblast)
- Size: Smaller still
- Nucleus: Coarse heterochromatin in a checkerboard pattern (highly characteristic); nucleus is reduced
- Cytoplasm: Mixed staining - both basophilic (ribosomes) and acidophilic (hemoglobin), giving gray or lilac color. This mixed staining is the hallmark of this stage.
- Key: This is the last stage capable of mitosis. Hemoglobin accumulation accelerates as RNA begins to fall.
- Duration: ~30 hours
Stage 4: Orthochromatophilic Erythroblast (Orthochromatic Normoblast / Late Normoblast)
- Size: Smaller than polychromatophilic stage
- Nucleus: Pyknotic (small, dense, dark, condensed) - N/C ratio is very low; mitosis is now impossible
- Cytoplasm: Predominantly acidophilic/eosinophilic due to abundant hemoglobin; only slight polychromasia remains; fewer polyribosomes
- Key step: After the last mitosis, the pyknotic nucleus + small rim of cytoplasm are extruded (enucleation) via cytoplasmic contractions, forming the reticulocyte
Stage 5: Reticulocyte (Polychromatophilic Erythrocyte)
- Nucleus: Absent (enucleated)
- Cytoplasm: Still contains residual ribosomes, mRNA, and mitochondria - giving a polychromatophilic (pink-gray) appearance on Wright-Giemsa stain; with supravital stains (brilliant cresyl blue) the ribosomal network appears as a reticulum (hence the name)
- Function: Still capable of synthesizing hemoglobin using residual mRNA and ribosomes
- Location: Reticulocytes spend 1-2 days in the bone marrow stroma, then are released into blood where they circulate for another ~1 day
- Maturation: The spleen removes residual organelles (ribosomes, mitochondria) → mature erythrocyte
- Normal reticulocyte count: ~1% of circulating RBCs
Stage 6: Mature Erythrocyte (RBC)
- Size: 7.2-7.8 µm biconcave disc
- No nucleus, no organelles
- Packed with hemoglobin (~33 g/dL intracellular)
- Lifespan: 120 days; senescent cells removed by macrophages in the spleen, liver, and bone marrow
Key mnemonic for maturation direction: Size ↓ → Nuclear chromatin condenses ↓ → Basophilia ↓ → Hemoglobin (acidophilia) ↑ → Nucleus extruded → Reticulocyte → Mature RBC
4. Erythroblastic Islands
In the bone marrow, developing erythroid cells are physically organized around central macrophages in structures called erythroblastic islands. The central macrophage:
- Provides iron for hemoglobin synthesis (via ferritin)
- Phagocytoses extruded nuclei
- Provides growth factors and adhesion signals
These islands are fragmented when marrow aspirates are spread on slides, but fragments of macrophage cytoplasm may remain attached to normoblasts (especially visible on Prussian blue-stained films).
5. Regulation of Erythropoiesis
Erythropoietin (EPO)
EPO is the master regulator of erythropoiesis. It is a glycoprotein (~30.4-34 kDa) produced:
- 90% by peritubular fibroblast-like interstitial cells in the renal cortex and outer medulla
- ~10% by the liver (hepatocytes and Ito cells)
EPO acts on CFU-E and early erythroblasts (which express EPO receptors / EPO-Rs), promoting:
- Proliferation of committed erythroid progenitors
- Survival (anti-apoptotic effect)
- Differentiation and hemoglobin synthesis
In the absence of EPO, severe anemia invariably results (as seen in renal failure).
The Hypoxia-HIF Axis
The renal oxygen sensor operates as a feedback loop:
Hypoxia → HIF-1α stabilized → Binds HIF-1β → Binds hypoxia response element
→ Erythropoietin gene transcription → EPO released → Bone marrow →
More RBCs → Improved O₂ delivery → Suppresses HIF → Less EPO
Under normoxic conditions, prolyl hydroxylase domain (PHD) enzymes hydroxylate HIF-1α, targeting it for proteasomal degradation by the VHL ubiquitin ligase. Hypoxia inhibits PHDs → HIF-1α is stabilized → translocates to nucleus → drives EPO gene expression.
HIF-2α (EPAS-1) is actually the more important isoform for EPO production in the kidney (compared to HIF-1α which has broader roles). Loss-of-function in the HIF-2α gene accounts for the lower hematocrit seen in Tibetan/Sherpa highlanders despite living at altitude.
Other Regulatory Factors
| Factor | Role |
|---|---|
| Iron | Essential for heme synthesis (protoporphyrin IX + Fe²⁺); absorbed in duodenum via DMT1, transported as transferrin, stored as ferritin/hemosiderin |
| Vitamin B12 (Cobalamin) | Required for DNA synthesis (thymidylate synthesis via methylmalonyl-CoA pathway); deficiency → megaloblastic anemia |
| Folic Acid | Required for DNA synthesis (thymidylate synthesis); deficiency → megaloblastic anemia |
| GATA-1 | Transcription factor essential for terminal erythroid differentiation |
| SCF (Stem Cell Factor) | Acts on BFU-E/early progenitors |
| IL-3 | Supports early erythroid progenitors |
| Testosterone/Androgens | Stimulate EPO production (explains higher Hgb in males) |
| Thyroid hormones | Permissive role; hypothyroidism causes mild anemia |
6. Kinetics and Production Numbers
- Each pronormoblast undergoes 3-4 mitotic divisions over ~3 days → theoretically produces up to 16 reticulocytes
- Approximately ~10¹² (1 trillion) RBCs produced per day
- Reticulocytes spend 1-2 days in marrow + 1 day in peripheral blood before full maturation
- Under severe hypoxia, the marrow pool of reticulocytes can be released, approximately doubling the circulating reticulocyte count
- Mature RBCs circulate for 120 days before destruction
7. Hemoglobin Synthesis During Erythropoiesis
Hemoglobin synthesis begins in the basophilic erythroblast and continues through to the reticulocyte stage:
- Heme synthesis occurs in mitochondria (ALA synthase is the rate-limiting enzyme) and cytoplasm
- Globin chain synthesis occurs on cytoplasmic ribosomes (polyribosomes)
- Each person synthesizes approximately 10¹² RBCs per day, so iron, B12, and folate deficiencies rapidly impair production
Hemoglobin switching:
- Embryonic Hgb (ζ₂ε₂) → present in yolk sac stage
- Fetal Hgb / HbF (α₂γ₂) → predominant during fetal life; higher O₂ affinity
- Adult HbA (α₂β₂) → predominant after ~6 months of age; ~97% of adult Hgb
- Adult HbA₂ (α₂δ₂) → ~2-3% of adult Hgb
8. Clinical Correlations
| Condition | Mechanism | Effect on Erythropoiesis |
|---|---|---|
| Iron deficiency anemia | Insufficient iron for heme | Microcytic, hypochromic anemia; increased RBC production attempts but cells are small |
| B12/Folate deficiency | Impaired DNA synthesis | Megaloblastic anemia; large cells; ineffective erythropoiesis |
| Thalassemia | Globin chain imbalance | Ineffective erythropoiesis; intramedullary destruction of erythroblasts; extramedullary hematopoiesis |
| Anemia of CKD | Low EPO production | Normocytic, normochromic anemia; responds to EPO therapy |
| Polycythemia vera | JAK2 V617F mutation → EPO-independent proliferation | Unregulated erythropoiesis |
| High-altitude erythrocytosis | Chronic hypoxia → elevated EPO | Increased RBC mass (polycythemia); problematic if Hct >60% due to hyperviscosity |
| Aplastic anemia | Stem cell failure/destruction | Pancytopenia; erythropoiesis severely reduced |
Sources:
- Histology: A Text and Atlas with Correlated Cell and Molecular Biology (Eroschenko)
- Henry's Clinical Diagnosis and Management by Laboratory Methods
- Basic Medical Biochemistry: A Clinical Approach, 6e
- Brenner and Rector's The Kidney, 2-Volume Set
- Goodman & Gilman's The Pharmacological Basis of Therapeutics
- Guyton and Hall Textbook of Medical Physiology
This is a shared conversation. Sign in to Orris to start your own chat.