Morphological and radiological (rotteveel) classification of otosclerosis in simplified manner for ms ent pg exam
Reading File
Finding Sources
Searching the Web
Rotteveel radiological classification otosclerosis stages simplified ENT
Finding Sources
Finding Sources
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC7051554
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Finding Sources
Searching the Web
morphological classification otosclerosis types footplate ENT PG exam Cremers Tos stapedial
Reading File
I now have all the information needed for a comprehensive, exam-ready answer. Here is the full response:
Otosclerosis: Morphological & Radiological (Rotteveel) Classification
For MS ENT PG Exam
PART 1: MORPHOLOGICAL CLASSIFICATION
A. Broad Morphological Types
| Type | Basis | Hearing Loss |
|---|---|---|
| Histological otosclerosis | Microscopic disease only; no fixation of ossicles; silent | None - found only at autopsy |
| Clinical otosclerosis | Disease causes symptoms (stapes fixation or cochlear involvement) | Present |
B. Clinical Otosclerosis - By Site
1. Stapedial (Fenestral) Otosclerosis - ~80%
- Focus at fissula ante fenestram (anterior oval window margin) - most common site
- Causes stapes footplate fixation → Conductive Hearing Loss (CHL)
- Can progress to oval window obliteration
Intraoperative footplate appearance (Malafronte classification):
| Degree | Appearance | Frequency | Description |
|---|---|---|---|
| I | Blue footplate | 71.8% | Otosclerotic focus from oval window rim - anterior (most common), posterior, or both |
| II | White footplate | 21.4% | Two subtypes: Diffuse (focus involves most of footplate) or Biscuit type (central island with well-defined rim, ~23%) |
| III | Obliterative | 6.8% | Massive otospongiotic focus completely covers footplate - most difficult surgically |
Exam tip: "Biscuit footplate" = white, disc-shaped mass in center of footplate with clear margins. "Obliterative otosclerosis" = footplate not visible at all = rare, challenging.
2. Cochlear (Retrofenestral) Otosclerosis - ~20%
- Demineralization of cochlear capsule (otic capsule)
- Causes Sensorineural or Mixed Hearing Loss
- Shows "double-ring effect" on CT / "fourth ring of Valvassori"
- Also called Malignant otosclerosis when severe SNHL occurs
3. Mixed Otosclerosis
- Stapedial + cochlear involvement
- Mixed hearing loss
C. Surgical/Footplate Classification (Tos modification of Cremers)
Based on whether the footplate or superstructure is fixed:
| Group | Feature |
|---|---|
| Group 1 | Footplate fixation only (superstructure mobile) |
| Group 2 | Footplate + superstructure fixed (monobloc stapes) |
- In ~20% of cases, the superstructure (crura) may be abnormal
PART 2: RADIOLOGICAL CLASSIFICATION - ROTTEVEEL CT CLASSIFICATION
This is the most commonly asked classification in PG exams for imaging of otosclerosis.
Based on: Rotteveel LJ et al. (2004) - from a study of 53 patients undergoing cochlear implantation for otosclerosis. Uses axial HRCT temporal bone.
The Three Types
TYPE 1 - Purely Fenestral
- Only fenestral (oval window area) involvement
- No cochlear/retrofenestral disease
- CT: Hypodense focus anterior to oval window (fissula ante fenestram)
- Hearing loss: Conductive only
TYPE 2 - Retrofenestral Disease (± Fenestral)
Retrofenestral = involvement of cochlear capsule. Divided into 3 subtypes:
| Subtype | Feature | Mnemonic |
|---|---|---|
| 2A | "Double-ring effect" only | A = ring Around cochlea |
| 2B | Narrowing of basal turn of cochlea only | B = Basal turn |
| 2C | Both double-ring effect + narrowed basal turn | C = Combination |
The "Double-Ring Effect" explained:
- Normal otic capsule = uniformly dense white ring on CT
- In active otosclerosis: spongiotic (demineralized) foci surround the cochlear canal → creates a halo of low density around the cochlear lumen
- Appears as: dense cochlear wall (inner ring) + hypodense spongiotic halo + outer otic capsule (outer ring) = double ring
- Indicates active retrofenestral disease
TYPE 3 - Severe Retrofenestral Involvement (± Fenestral)
- Otic capsule is unrecognizable
- Complete dissolution of cochlear capsule architecture
- Massive demineralization throughout
- Hearing loss: Severe-profound SNHL
- These patients are candidates for cochlear implantation
- Surgically challenging due to obliteration
Summary Table - Rotteveel Classification
| Type | Location | CT Finding | Clinical Implication |
|---|---|---|---|
| 1 | Fenestral only | Hypodensity at fissula ante fenestram | CHL → stapedectomy candidate |
| 2A | Retrofenestral | Double-ring effect around cochlea | Mixed HL |
| 2B | Retrofenestral | Basal turn narrowing | Mixed HL |
| 2C | Retrofenestral | Double-ring + basal turn narrowing | Mixed/SNHL |
| 3 | Severe retrofenestral | Unrecognizable otic capsule | Profound SNHL → CI candidate |
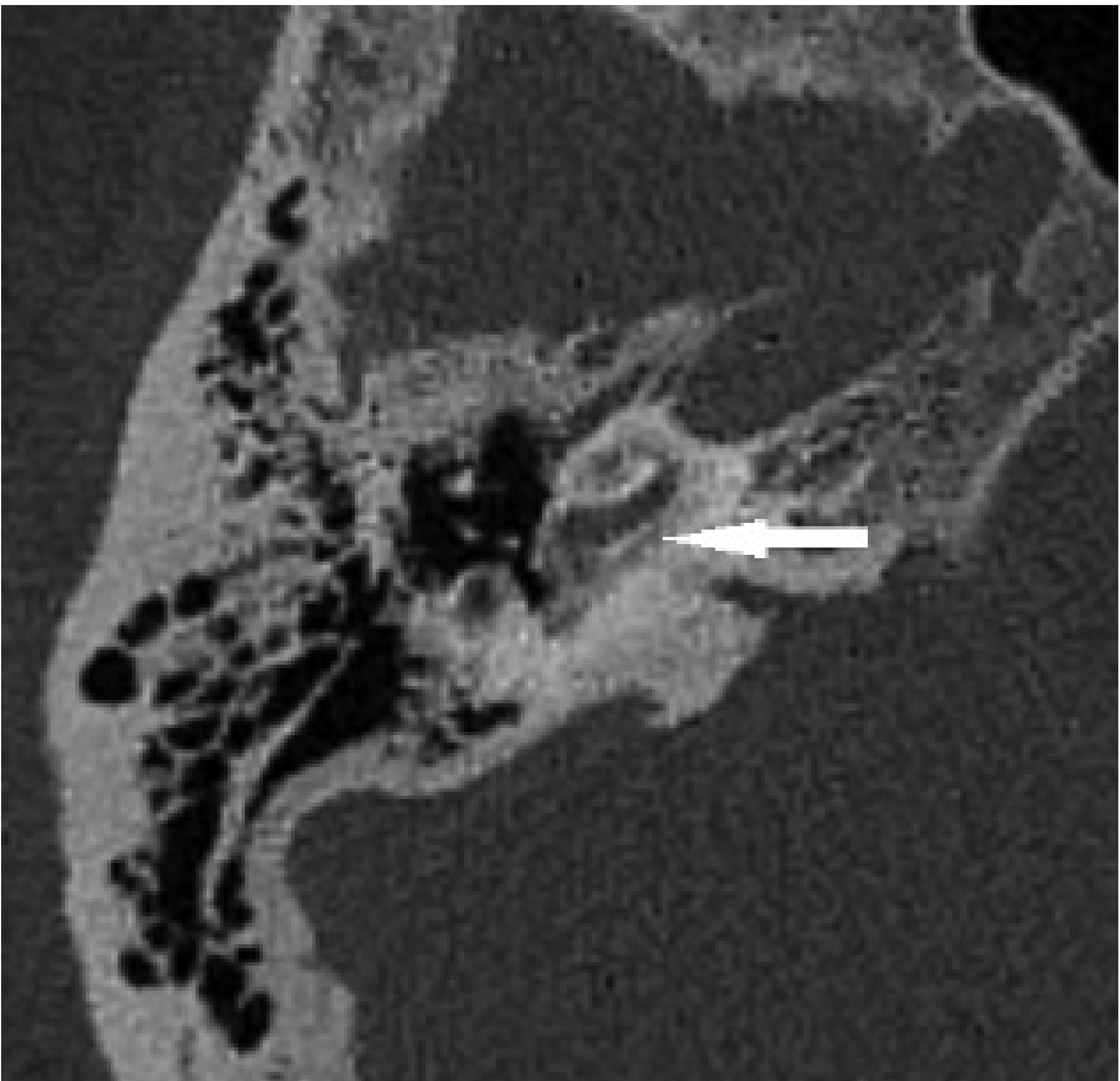
CT Image - Retrofenestral Otosclerosis
This axial CT from Scott-Brown's shows low density surrounding the cochlea (arrow) - the hallmark of retrofenestral otosclerosis:
Comparison with Symons/Fanning Classification (Also Asked)
| Symons/Fanning Grade | Description | Rotteveel Equivalent |
|---|---|---|
| 0 | Normal | - |
| 1 | Fenestral only (spongiotic or sclerotic) | Type 1 |
| 2A | Basal turn cochlear disease ± fenestral | Type 2B |
| 2B | Middle/apical turns ± fenestral | Type 2 variants |
| 3 | Diffuse confluent cochlear involvement | Type 3 |
Symons/Fanning has better interobserver agreement (κ = 0.92) vs Rotteveel (κ = 0.77) and allows more precise cochlear localization. However, Rotteveel is more commonly asked in Indian PG exams.
Key Exam Points to Remember
- Most common site of otosclerosis = fissula ante fenestram (anterior oval window)
- Fourth ring of Valvassori = the spongiotic halo seen around cochlea on CT in retrofenestral disease
- Double-ring sign = pathognomonic of active retrofenestral otosclerosis on CT
- Rotteveel Type 3 = unrecognizable otic capsule = worst prognosis = cochlear implant candidate
- Biscuit footplate = white, disc-shaped footplate - a morphological surgical finding
- Obliterative otosclerosis = no visible footplate - requires laser/drill for fenestration
- CT is the investigation of choice; MRI shows enhancement on post-contrast T1 in active phase
- Normal otic capsule = densest bone in body - any loss of density = abnormal
Sources: Cummings Otolaryngology (Chapter 146); Scott-Brown's Otorhinolaryngology Vol 2 (Chapter 97); Shambaugh Surgery of the Ear (Chapter 13); Rotteveel et al., Otology & Neurotology 2004; Symons & Fanning CT Grading (PMC7051554)
This is a shared conversation. Sign in to Orris to start your own chat.