Pleural tapping datail with lab, diagnosis
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a detailed, textbook-sourced guide to pleural tapping (thoracentesis) - from procedure technique to laboratory analysis and diagnosis.
Pleural Tapping (Thoracentesis) - Complete Guide
1. Definition and Indications
Thoracentesis is the insertion of a needle or catheter into the pleural space to aspirate fluid. It may be:
- Diagnostic - to determine the cause of an undiagnosed pleural effusion
- Therapeutic - to relieve dyspnea from a large effusion
Indications for diagnostic thoracentesis: Any free pleural fluid measuring >10 mm on lateral decubitus film, ultrasound, or chest CT without a clearly evident cause. Even when CHF is suspected, thoracentesis should not be delayed if the patient is febrile, has pleuritic chest pain, or effusions are asymmetric.
2. Patient Positioning
Three positions are used, shown below:
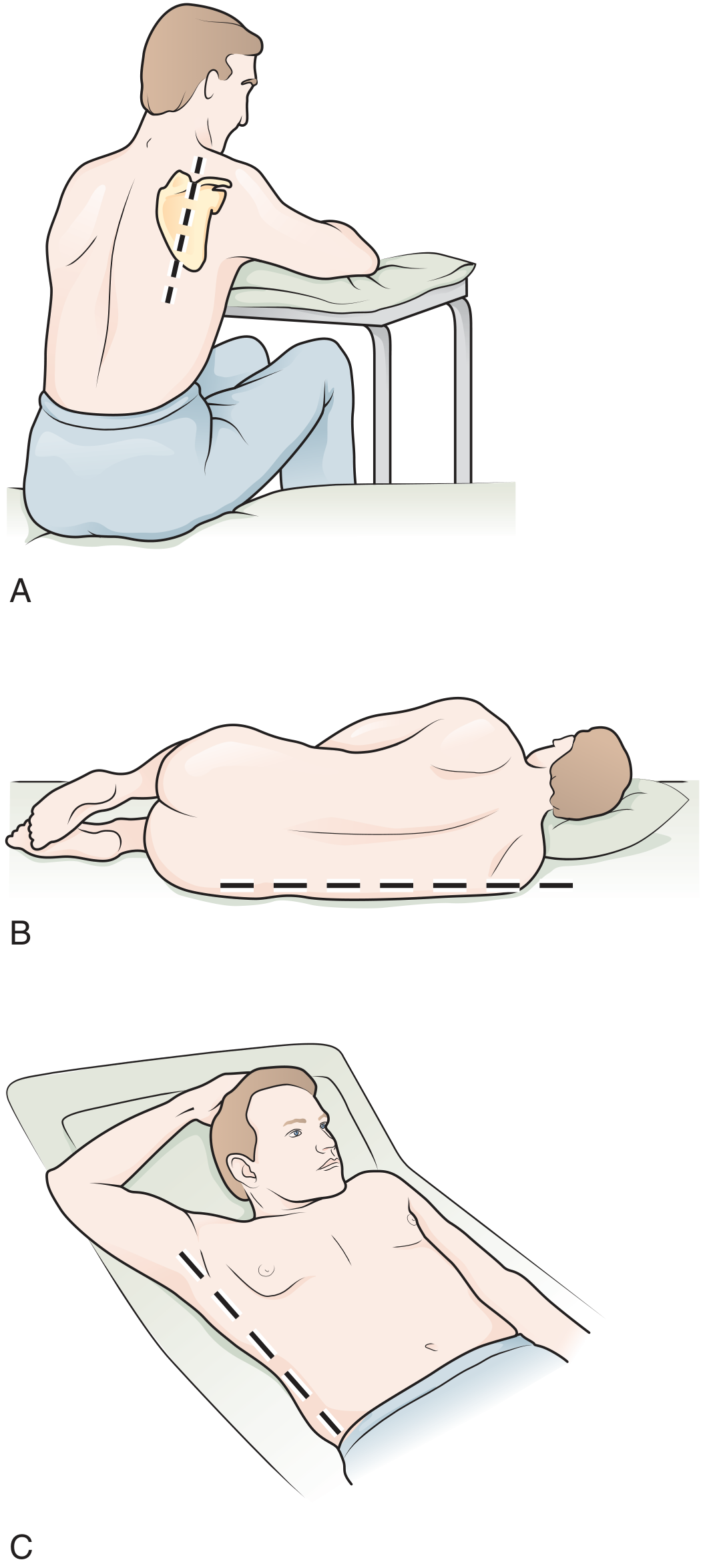
A. Upright (preferred): Patient sits on edge of bed, arms extended forward on a Mayo stand, leaning slightly forward.
B. Lateral decubitus: Used when patient is too ill to sit; affected side down, back at edge of bed - insert at posterior axillary line.
C. Supine with head elevated: Use midaxillary line as insertion point.
3. Site of Needle Insertion
- 1-2 intercostal spaces below the highest level of effusion in the midscapular or posterior axillary line
- Never below the 9th rib (risk of diaphragm/liver/spleen injury)
- Never medial to the midscapular line (intercostal artery runs more centrally near the spine)
- Needle passes over the top of the rib (never below the rib) to avoid the neurovascular bundle
- At least 10 mm of fluid thickness should be confirmed on ultrasound at the selected site
4. Equipment
- 3.5-5 MHz ultrasound transducer for guidance
- 25-gauge needle + 1% or 2% lidocaine for local anesthesia
- Thoracentesis needle-catheter unit (over-the-needle catheter)
- 10-60 mL syringes, three-way stopcock
- High-pressure collection tubing with vacuum bottle
- Sterile drapes and gloves
5. Procedure Steps
- Ultrasound localization - confirm fluid level, measure depth, mark insertion site
- Time-out - verify correct patient, procedure, and side
- Sterile prep and draping of the insertion site
- Local anesthesia - create a skin wheal at the upper edge of the rib with 25-gauge needle using lidocaine; advance through anesthetized track down to the parietal pleura
- Needle insertion - walk the needle-catheter unit over the rib, applying gentle negative pressure; when fluid enters syringe, angle slightly caudally
- Advance catheter - hold needle steady, twist catheter to break its seal, advance into pleural space; immediately cover catheter hub to prevent air entry
- Collect diagnostic specimen first (~60 mL into labeled tubes)
- Drain therapeutic volume using vacuum bottle via three-way stopcock
- Volume limit: Maximum 1500 mL to avoid reexpansion pulmonary edema and symptomatic hypotension
- Withdrawal - ask patient to exhale fully, then withdraw needle
6. Post-Procedure
- Post-procedure CXR or bedside ultrasound (check for lung sliding) to exclude pneumothorax
- Routine CXR is NOT needed in uncomplicated, well-tolerated procedures
- Patients at higher risk (prior radiotherapy, multiple passes, mechanical ventilation, new symptoms) require imaging
7. Complications
| Complication | Rate | Notes |
|---|---|---|
| Pneumothorax | ~2-6% (0.6% with US guidance) | Only ~1/3 require chest tube |
| Hemothorax | ~1% (0.2% with US guidance) | Due to intercostal artery injury |
| Reexpansion pulmonary edema | ~0.01% | Risk with >1500 mL removed |
| Pneumothorax ex vacuo | Rare | Occurs when lung cannot reexpand (endobronchial lesion) |
Source: Roberts and Hedges' Clinical Procedures in Emergency Medicine; Murray & Nadel's Textbook of Respiratory Medicine
8. Pleural Fluid Analysis - Lab Tests
Step 1: Visual Inspection
| Appearance | Suggests |
|---|---|
| Bloody / hemorrhagic | Trauma, malignancy, pulmonary infarction |
| White / milky | Lipids (chylothorax or pseudochylothorax) |
| Purulent, malodorous | Empyema |
| Contains food particles | Esophageal rupture |
Step 2: Transudate vs. Exudate - Light's Criteria
The first and most important step. Exudate is present if at least ONE of the following is met:
| Criterion | Exudate Threshold |
|---|---|
| Pleural fluid protein / Serum protein ratio | > 0.5 |
| Pleural fluid LDH / Serum LDH ratio | > 0.6 |
| Pleural fluid LDH | > 2/3 upper limit of normal serum LDH |
If transudate: Stop further fluid analysis; treat the underlying cause (CHF, cirrhosis, nephrotic syndrome).
Alternative criteria when diuretics have been used (CHF): Diuretics falsely elevate pleural protein and LDH, making transudates appear exudative. Use instead:
- Serum protein - pleural protein > 3.1 g/dL → transudate
- Serum albumin - pleural albumin > 1.2 g/dL → transudate
- Pleural fluid NT-proBNP > 1500 pg/mL → CHF (94% sensitive, 91% specific)
Step 3: Exudate Workup - Standard Tests (All Undiagnosed Exudates)
| Test | Result | Probable Diagnosis |
|---|---|---|
| WBC count | >10,000 cells/mm³ | Parapneumonic (also pancreatitis, PE, collagen vascular) |
| Neutrophil predominance | >50% | Acute process: pneumonia, pulmonary infarction |
| Lymphocyte predominance | >50% | Chronic process: malignancy, TB |
| Eosinophils | >10% | Blood/air in pleural space; no clear etiology common |
| Glucose | <60 mg/dL | Complicated parapneumonic, malignancy, TB, rheumatoid, hemothorax, paragonimiasis |
| Glucose | <40 mg/dL | Consider tube thoracostomy (parapneumonic) |
| Glucose | <30 mg/dL | Rheumatoid pleuritis |
| Glucose | >80 mg/dL in exudate | Suggests SLE |
| Cytology | Malignant cells | Malignancy (sensitivity ~55-60% on 1st sample; up to 90% with 3 samples) |
| Gram stain + culture | Positive | Bacterial infection; inoculate blood culture bottles for 20% higher yield |
Step 4: Pleural Fluid pH
- Measured with a blood gas machine (pH paper/meter not accurate)
- Collected anaerobically in heparinized syringe, placed on ice, analyzed within 1 hour
- pH <7.20 is seen in 10 conditions: complicated parapneumonic, esophageal rupture, rheumatoid pleuritis, TB, malignancy, hemothorax, systemic acidosis, paragonimiasis, lupus, urinothorax
Critical threshold: pH <7.20 in parapneumonic effusion = indication for chest tube (tube thoracostomy)
Pleural fluid glucose <60 mg/dL can substitute for pH when accuracy cannot be ensured.
Step 5: Additional Targeted Tests
| Test | Indication | Interpretation |
|---|---|---|
| Hematocrit (bloody fluid) | Bloody appearance | PF Hct >50% of serum Hct = hemothorax → tube thoracostomy |
| NT-proBNP | Suspected CHF | >1500 pg/mL = CHF with 94% sensitivity, 91% specificity |
| AFB culture + ADA | Suspected TB | Elevated ADA supports TB pleuritis |
| Triglycerides | Milky fluid | >110 mg/dL = chylothorax |
| Cholesterol | Milky fluid | Elevated = pseudochylothorax (cholesterol effusion) |
| Amylase | Suspected pancreatitis or esophageal rupture | Elevated amylase |
| LDH serial levels | Monitoring known exudate | Rising LDH = worsening inflammation; falling = resolving |
9. Diagnosis by Effusion Type
Transudates (causes)
- Congestive heart failure (most common)
- Hepatic hydrothorax (cirrhosis)
- Nephrotic syndrome
- Myxedema
- Peritoneal dialysis
- Pericardial disease
- Central venous occlusion
Exudates (causes)
- Infectious: Bacterial parapneumonic/empyema, TB, fungal, viral
- Malignant: Metastatic disease (most common), mesothelioma, lymphoma
- Inflammatory: Rheumatoid pleuritis, SLE, sarcoidosis, drug-induced
- Vascular: Pulmonary embolism
- GI: Pancreatitis, esophageal perforation, hepatic abscess
- Other: Chylothorax, hemothorax, post-cardiac injury syndrome
10. Indications for Tube Thoracostomy (in Parapneumonic Effusion)
- Effusion >50% of hemithorax
- Loculated effusion
- Pleural thickening on CT
- Frank pus aspirated (empyema)
- Pleural fluid pH <7.20
- Pleural fluid glucose <60 mg/dL
- Positive Gram stain or culture
11. Contraindications and Special Situations
- Coagulopathy / thrombocytopenia: Safe when performed by experienced operators (small-bore needle)
- Mechanical ventilation: Can be done safely with US guidance
- Clopidogrel: Ideally withhold 5 days before procedure (Society of Interventional Radiology); use US guidance if cannot be withheld
- Pediatric patients: Same principles; smallest possible needle; sedation may be needed; never below the 9th rib
Sources: Roberts and Hedges' Clinical Procedures in Emergency Medicine; Murray & Nadel's Textbook of Respiratory Medicine (2-Volume); Fishman's Pulmonary Diseases and Disorders; Tintinalli's Emergency Medicine
In Hinghlish
Pleural Tapping (Thoracentesis) - Hinglish mein
1. Definition aur Indications
Thoracentesis ek procedure hai jisme pleural space mein needle ya catheter daali jaati hai aur fluid aspirate kiya jaata hai. Yeh do types ka hota hai:
- Diagnostic - fluid ka cause pata karne ke liye
- Therapeutic - badi effusion se dyspnea (saans ki takleef) kam karne ke liye
Kab karna chahiye? Jab bhi free pleural fluid >10 mm dikhe X-ray, ultrasound ya CT scan par - aur cause clearly pata nahi ho. Agar patient ko fever hai, pleuritic chest pain hai, ya dono sides ki effusion unequal size ki hai - toh bina delay ke thoracentesis karo, CHF ka wait mat karo.
2. Patient Positioning
A. Upright (best position): Patient bed ke edge par baithega, dono haath aage Mayo stand par rakhe, thoda aage jhuke.
B. Lateral decubitus: Jab patient baitha nahi sak raha - affected side neeche rakho, back bed ke edge par ho - posterior axillary line par needle daalo.
C. Supine with head elevated: Midaxillary line par needle daalo.
3. Needle Kahan Daalni Hai
- Effusion ke highest level se 1-2 intercostal space neeche, midscapular ya posterior axillary line mein
- 9th rib se neeche kabhi nahi - diaphragm, liver ya spleen injury ka risk
- Midscapular line se medial kabhi nahi - wahan intercostal artery zyada central hoti hai
- Needle rib ke upar se jaaye - neeche se nahi (neurovascular bundle bachao)
- US par selected site par minimum 10 mm fluid hona chahiye
4. Procedure Steps - Step by Step
- Ultrasound se localize karo - fluid depth confirm karo, site mark karo
- Time-out lo - sahi patient, sahi procedure, sahi side verify karo
- Sterile prep aur draping karo
- Local anesthesia - 25-gauge needle se lidocaine (1-2%) ka skin wheal banao rib ke upper edge par; parietal pleura tak anesthetize karo
- Needle insert karo - rib ke upar se walk karo, gentle suction lagate raho; jab fluid aaye toh needle ko thoda caudally angle karo
- Catheter advance karo - needle ko hold karo, catheter twist karke pleural space mein advance karo; hub ko finger se cover karo taaki air andar na jaaye
- Diagnostic specimen pehle collect karo (~60 mL)
- Therapeutic drainage - vacuum bottle se, three-way stopcock ke zariye
- Maximum 1500 mL drain karo ek baar mein - zyada nikalne se reexpansion pulmonary edema ho sakta hai
- Withdrawal - patient ko puri saans chhod ne kaho, phir needle nikaalo
5. Complications
| Complication | Rate | Baat |
|---|---|---|
| Pneumothorax | 2-6% (US se 0.6%) | Sirf 1/3 ko chest tube chahiye |
| Hemothorax | 1% (US se 0.2%) | Intercostal artery injury se |
| Reexpansion pulmonary edema | 0.01% | >1500 mL nikalne par |
6. Pleural Fluid Lab Analysis
Step 1: Visual Dekho - Aankhon Se
| Fluid kaisa dikhta hai | Kya suggest karta hai |
|---|---|
| Bloody / laal | Trauma, malignancy, pulmonary infarction |
| White / milky | Lipids - chylothorax |
| Purulent, badbu wala | Empyema (pus) |
| Khaane ke particles | Esophageal rupture |
Step 2: Transudate vs Exudate - Light's Criteria ⭐
Yeh SABSE PEHLA aur SABSE ZAROORI step hai. Agar koi EK bhi criteria meet ho toh EXUDATE hai:
| Criteria | Exudate hoga agar |
|---|---|
| Pleural fluid protein / Serum protein | > 0.5 |
| Pleural fluid LDH / Serum LDH | > 0.6 |
| Pleural fluid LDH | > 2/3 upper limit of normal serum LDH |
Yaad rakho: Agar transudate hai toh aur koi fluid test mat karo - seedha underlying cause treat karo (CHF, cirrhosis, nephrotic syndrome).
Jab patient diuretics le raha ho (CHF mein): Diuretics protein aur LDH badha dete hain, isliye transudate bhi exudate lag sakta hai. Tab yeh use karo:
- Serum protein - Pleural protein > 3.1 g/dL → Transudate
- Serum albumin - Pleural albumin > 1.2 g/dL → Transudate
- Pleural NT-proBNP > 1500 pg/mL → CHF (94% sensitive)
Step 3: Exudate Mein Standard Tests
| Test | Result | Diagnosis |
|---|---|---|
| WBC count | >10,000/mm³ | Parapneumonic (pneumonia wali effusion) |
| Neutrophil predominance | >50% | Acute process - pneumonia, pulmonary infarction |
| Lymphocyte predominance | >50% | Chronic - malignancy ya TB |
| Eosinophils | >10% | Blood ya air pleural space mein |
| Glucose | <60 mg/dL | Complicated parapneumonic, malignancy, TB, rheumatoid |
| Glucose | <40 mg/dL | Chest tube lagao (parapneumonic mein) |
| Glucose | <30 mg/dL | Rheumatoid pleuritis |
| Cytology | Malignant cells | Malignancy (1st sample mein ~60% sensitive; 3 samples mein ~90%) |
| Gram stain + Culture | Positive | Bacterial infection; blood culture bottles mein inoculate karo - yield 20% badh jaati hai |
Step 4: Pleural Fluid pH
- Blood gas machine se measure karo sirf - pH paper ya meter accurate nahi hota
- Heparinized syringe mein anaerobically collect karo, ice par rakho, 1 ghante mein analyze karo
- pH <7.20 in 10 conditions mein hota hai:
- Complicated parapneumonic
- Esophageal rupture
- Rheumatoid pleuritis
- TB pleuritis
- Malignancy
- Hemothorax
- Systemic acidosis
- Paragonimiasis
- Lupus pleuritis
- Urinothorax
Critical: Parapneumonic effusion mein pH <7.20 = Chest tube daalo!
Agar pH accurately measure nahi ho sakta, toh glucose <60 mg/dL substitute kar sakte ho.
Step 5: Additional Tests (Targeted)
| Test | Kab karo | Kya matlab |
|---|---|---|
| Hematocrit | Fluid bloody ho | PF Hct >50% of serum Hct = Hemothorax → Tube thoracostomy |
| NT-proBNP | CHF suspected | >1500 pg/mL = CHF |
| ADA (Adenosine Deaminase) | TB suspected | Elevated = TB pleuritis |
| Triglycerides | Milky fluid | >110 mg/dL = Chylothorax |
| Amylase | Pancreatitis / esophageal rupture suspected | Elevated |
| LDH serial | Known exudate monitor | Rising = worsening; Falling = resolving |
7. Diagnosis - Effusion Type se
Transudate ki causes (yaad karo - LOW protein, LOW LDH)
- CHF (sabse common)
- Hepatic hydrothorax (cirrhosis)
- Nephrotic syndrome
- Myxedema (hypothyroidism)
- Peritoneal dialysis
- Pericardial disease
Exudate ki causes (HIGH protein, HIGH LDH)
- Infectious: Parapneumonic / empyema, TB, fungal
- Malignant: Metastatic disease (lung, breast, lymphoma), mesothelioma
- Inflammatory: Rheumatoid pleuritis, SLE, drug-induced
- Vascular: Pulmonary embolism
- GI: Pancreatitis, esophageal perforation
- Others: Chylothorax, hemothorax
8. Tube Thoracostomy kab karo? (Parapneumonic mein)
Yeh saare indications hain chest tube daalne ke:
- Effusion hemithorax ka >50%
- Loculated effusion
- CT par pleural thickening
- Frank pus aspirate ho (empyema)
- Pleural fluid pH <7.20
- Pleural fluid glucose <60 mg/dL
- Positive Gram stain ya culture
Quick Revision Table 📋
Fluid dikhne par:
↓
Light's Criteria lagao
↓
Transudate → CHF/Cirrhosis/Nephrotic treat karo
↓
Exudate → WBC differential + Glucose + Culture + Cytology
↓
pH <7.20 ya Glucose <60 + parapneumonic → CHEST TUBE
↓
Cytology positive → Malignancy workup
↓
Lymphocyte dominant + ADA high → TB treat karo
Sources: Roberts and Hedges' Clinical Procedures in Emergency Medicine; Murray & Nadel's Textbook of Respiratory Medicine; Fishman's Pulmonary Diseases and Disorders; Tintinalli's Emergency Medicine
CHF kya hai
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Ab mere paas poora material hai. Hinglish mein comprehensive answer deta hoon.
CHF (Congestive Heart Failure) - Hinglish mein
CHF ka Full Form kya hai?
CHF = Congestive Heart Failure
Hindi mein: Dil ki Kamzori ya Dil ka Failur
Yeh ek syndrome hai jisme heart itna kamzor ho jaata hai ki woh body ki zaroorat ke hisaab se poora khoon pump nahi kar sakta. Iske wajah se fluid body mein jama ho jaata hai - khaas kar lungs (congestion) aur pair-paon mein (edema).
Simple Analogy se Samjho 🫀
Soch lo dil ek water pump hai. Pump agar theek se kaam na kare, toh paani tank mein bhar jaata hai. Usi tarah dil agar theek se pump na kare, toh fluid lungs aur body mein bhar jaata hai - isse CHF kehte hain.
1. Causes - CHF Kyon Hota Hai?
| Cause | Hindi Explanation |
|---|---|
| Coronary Artery Disease (CAD) | Dil ki naaliyan block hona |
| Hypertension (HTN) | High blood pressure se dil ka kaam badhna |
| Myocardial Infarction (MI) | Heart attack ke baad dil kamzor hona |
| Valvular Heart Disease | Dil ke valve ka kharaab hona |
| Diabetes | Sugar se blood vessels damage |
| Alcoholism | Sharaab se heart muscle damage |
| Anemia | Khoon ki kami |
| Hyperthyroidism | Thyroid zyada active hona |
2. Pathophysiology - Andar Kya Hota Hai?
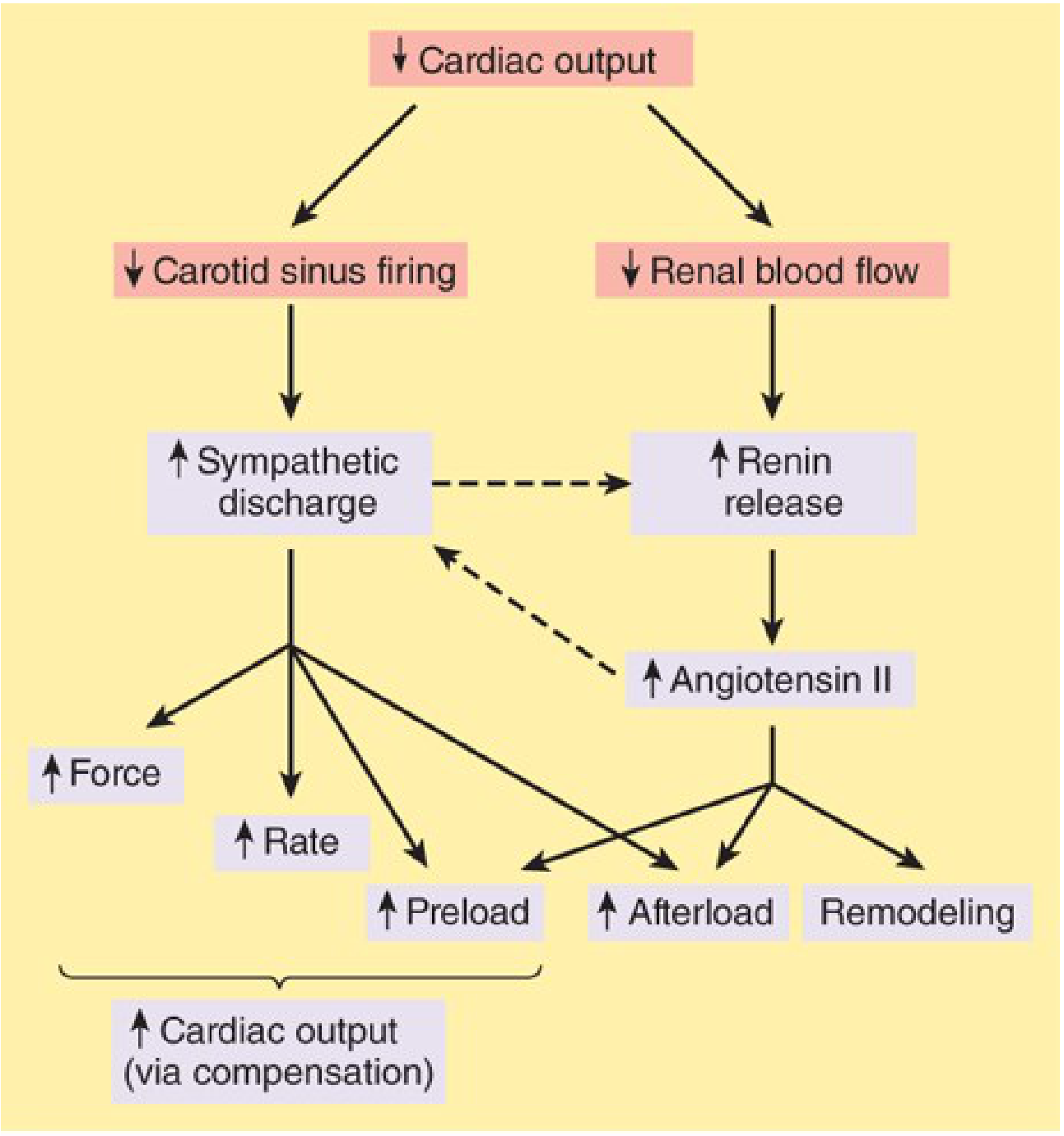
Step by Step Samjho:
Step 1 - Dil ka output girta hai
Kisi bhi cause se dil ka cardiac output (pump karne ki taakat) kam ho jaati hai.
Step 2 - Body compensate karne ki koshish karti hai
Body do bade systems activate karti hai:
- Sympathetic Nervous System (SNS): Dil tez dhakta hai, zyada force se pump karta hai
- RAAS (Renin-Angiotensin-Aldosterone System): Kidney kam blood flow feel karke renin release karti hai → Angiotensin II banta hai → Aldosterone banta hai → Body mein sodium aur paani retain hota hai
Step 3 - Iska ulta asar hota hai (Vicious Cycle)
- Angiotensin II afterload badhata hai (dil ko pump karne mein zyada resistance)
- Aldosterone fluid retain karata hai (load aur badh jaata hai)
- Catecholamines (adrenaline) dil ki muscle ko directly toxic hote hain
- Heart muscle remodel hoti hai - stretch hoti hai, dilate hoti hai, aur aur kamzor hoti jaati hai
↓ Cardiac Output
↓
SNS + RAAS activate
↓
Vasoconstriction + Fluid Retention
↓
↑ Afterload + ↑ Preload
↓
Heart aur kamzor hota jaata hai ← Yeh cycle repeat hota rehta hai
3. Types of CHF
A. Systolic Heart Failure (HFrEF)
- Dil ki pump karne ki taakat kam ho jaati hai
- Ejection Fraction (EF) <45% (normal >60%)
- Dil bada aur dilated dikhta hai
- Zyada common - MI ke baad hota hai
B. Diastolic Heart Failure (HFpEF)
- Dil pump toh karta hai theek se, par relax nahi kar pata
- EF normal rehta hai
- HTN, diabetes, aging se hota hai
- Dil stiff aur hypertrophied hota hai
C. High-Output Failure (rare)
- Body ki demand itni zyada hoti hai ki normal output bhi insufficient
- Hyperthyroidism, severe anemia, arteriovenous shunts mein
4. Symptoms - CHF mein kya lagta hai?
Left Heart Failure (Lungs mein fluid):
- Dyspnea - saans phoolna (exertion par ya rest par)
- Orthopnea - lait kar saans nahi aa rahi, 2-3 takia rakh ke sona padta hai
- PND (Paroxysmal Nocturnal Dyspnea) - raat ko achanak uthkar saans lena
- Cough - pink frothy sputum (pulmonary edema mein)
- Crackles - lungs mein fluid ki wajah se awaaz
Right Heart Failure (Body mein fluid):
- Pedal edema - pair-paon mein sujan
- Ascites - pet mein paani
- Hepatomegaly - liver bada hona
- JVP raised - gardan ki naso mein pressure
- Pleural effusion - chest mein paani (isi liye CHF transudate effusion ka #1 cause hai!)
Dono mein:
- Tachycardia - dil tez chalna
- Fatigue - thakaan, exercise tolerance kam hona
- Cardiomegaly - dil ka bada hona X-ray par
5. Classification - NYHA aur ACC/AHA
NYHA (New York Heart Association) - Symptoms ke hisaab se:
| Class | Kya hota hai |
|---|---|
| Class I | Koi symptom nahi - normal activity par koi takleef nahi |
| Class II | Thodi zyada activity par saans phoolna |
| Class III | Normal activity par bhi saans phoolna, aaraama par theek |
| Class IV | Aaraam par bhi saans nahi aati - sabse severe |
ACC/AHA Stages:
| Stage | Description |
|---|---|
| A | Risk factors hain (HTN, DM, CAD) par dil theek hai - koi symptom nahi |
| B | Dil mein structural problem hai par abhi symptom nahi |
| C | Dil mein problem + symptoms hain (NYHA II-III) |
| D | Aaraama par bhi symptoms - end-stage (NYHA IV) |
6. Diagnosis - Kaise Pata Chalta Hai?
| Test | Kya milta hai |
|---|---|
| ECG | Arrhythmia, LVH, ischemia ke signs |
| Chest X-ray | Cardiomegaly, pulmonary congestion, pleural effusion |
| Echocardiogram | EF measure karna, structure dekhna - sabse important test |
| BNP / NT-proBNP | >400 pg/mL = CHF (biomarker of cardiac stretch) |
| CBC | Anemia rule out karo |
| Serum electrolytes | Na, K, Cr - treatment guide karta hai |
| LFT/KFT | Liver aur kidney function CHF se affect hote hain |
| Thyroid function | Hypothyroidism/hyperthyroidism rule out |
7. Treatment - Kya Karte Hain?
Drugs jo mortality kam karti hain (Life-saving!):
| Drug | Kaise kaam karta hai | Dose (example) |
|---|---|---|
| ACE Inhibitors (Enalapril, Ramipril) | RAAS block karo, afterload kam karo | Enalapril 2.5-20mg BD |
| ARBs (Losartan) | ACE intolerant patients ke liye | Losartan 25-100mg OD |
| Beta Blockers (Carvedilol, Metoprolol) | SNS block karo, HR kam karo | Carvedilol 3.125-25mg BD |
| Aldosterone Antagonists (Spironolactone) | Fluid aur sodium retain hone se roko | 25-50mg OD |
| ARNI (Sacubitril/Valsartan) | Modern therapy - survival badhata hai | - |
| SGLT2 inhibitors (Dapagliflozin) | New drug - HF hospitalizations kam karta hai | - |
Symptomatic Relief ke liye:
| Drug | Kaam |
|---|---|
| Diuretics (Furosemide) | Fluid bahar nikalo - edema kam karo |
| Digoxin | Dil ki pumping improve karo (symptoms mein) |
Non-pharmacological:
- Salt restriction (namak kam - <2g/day)
- Fluid restriction
- Daily weight monitoring
- Exercise (stable CHF mein)
- ICD/CRT (advanced cases mein)
- Heart transplant (end-stage)
8. CHF aur Pleural Effusion ka Connection
CHF transudate pleural effusion ka sabse common cause hai. Yeh isliye hota hai:
- Left heart fail hota hai → Pulmonary venous pressure badhti hai → Fluid lungs ke bahar pleural space mein aata hai
- Right heart fail hota hai → Systemic venous pressure badhti hai → Direct pleural leakage
Yaad rakho: CHF mein pleural effusion mostly bilateral hota hai; unilateral hoga toh aur cause sochna padega.
CHF ki pleural effusion mein Light's criteria false positive de sakta hai agar patient diuretics le raha ho - isliye NT-proBNP >1500 pg/mL use karo confirm karne ke liye.
Quick Summary Box 📋
CHF = Dil pump nahi kar pata
↓
Lungs mein paani → Saans phoolna
Pair mein paani → Sujan
Pleural space mein paani → Pleural effusion (transudate)
↓
Diagnosis: Echo + BNP + CXR
↓
Treatment: ACEi + Beta-blocker + Diuretic + Spiro
↓
Mortality: ~50% within 5 years of diagnosis
Sources: Textbook of Family Medicine; Katzung's Basic and Clinical Pharmacology; Braunwald's Heart Disease; Murray & Nadel's Textbook of Respiratory Medicine
This is a shared conversation. Sign in to Orris to start your own chat.