Femoral head blood supply
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive, high-quality information from multiple authoritative sources. Here is the complete answer:
Blood Supply to the Femoral Head
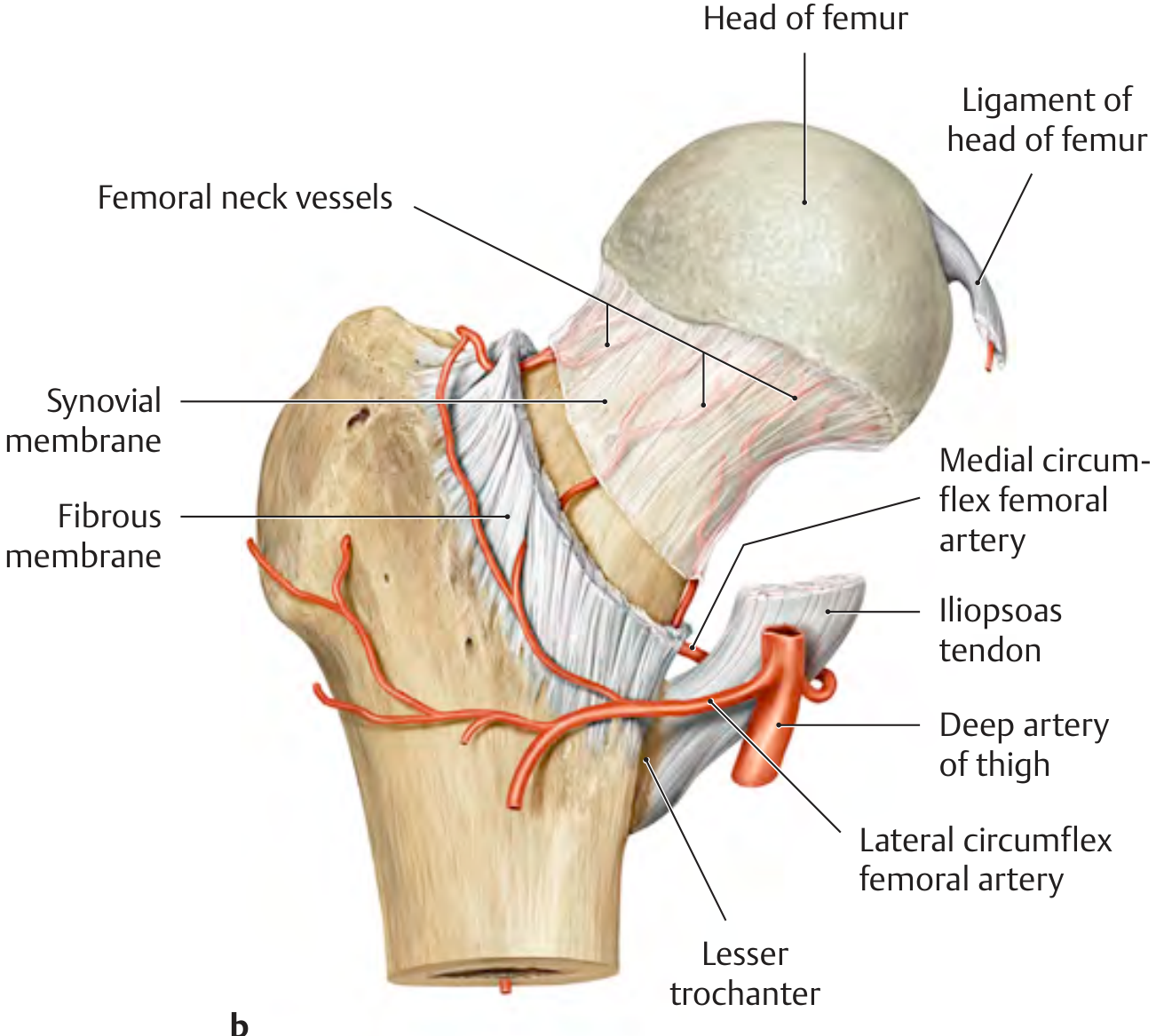
Course of femoral neck vessels showing the medial and lateral circumflex femoral arteries and the ligament of the head of femur (THIEME Atlas of General Anatomy)
Three Sources of Blood Supply
The femoral head receives blood from three distinct sources:
1. Retinacular (Capsular) Vessels - Most Important
These are the dominant supply. They arise primarily from the medial femoral circumflex artery (MFCA) and to a lesser extent from the lateral femoral circumflex artery (LFCA), both of which are branches of the profunda femoris artery (in 79% of individuals; in ~20%, one or both arise directly from the femoral artery).
- The MFCA and LFCA form an extracapsular arterial ring at the base of the femoral neck.
- From this ring, ascending cervical arteries course along the neck, penetrate the capsule, and form the subsynovial intracapsular arterial ring at the base of the femoral head.
- The terminal branches travel within fibrous extensions of the capsule wall called the retinacula of Weitbrecht (posterosuperior on the femoral neck) and perforate bone 2-4 mm lateral to the articular cartilage.
- There are four groups of terminal vessels (anterior, medial, lateral, posterior) - the lateral group is the largest contributor.
Quantitative contribution (cadaveric MRI, Dewar et al.):
- MFCA: ~82% of femoral head perfusion
- LFCA: ~18% of femoral head perfusion
2. Intramedullary Vessels
Some additional blood supply reaches the femoral head via medullary bone in the femoral neck. These vessels are equally vulnerable to disruption in displaced fractures.
3. Artery of the Ligamentum Teres (Foveal Artery)
- A branch of the obturator artery (or occasionally the MFCA).
- Enters through the ligamentum teres to supply the foveal region of the femoral head.
- Generally small, variable, and insufficient on its own to maintain complete vascularity of the entire head - it cannot compensate after displaced fractures.
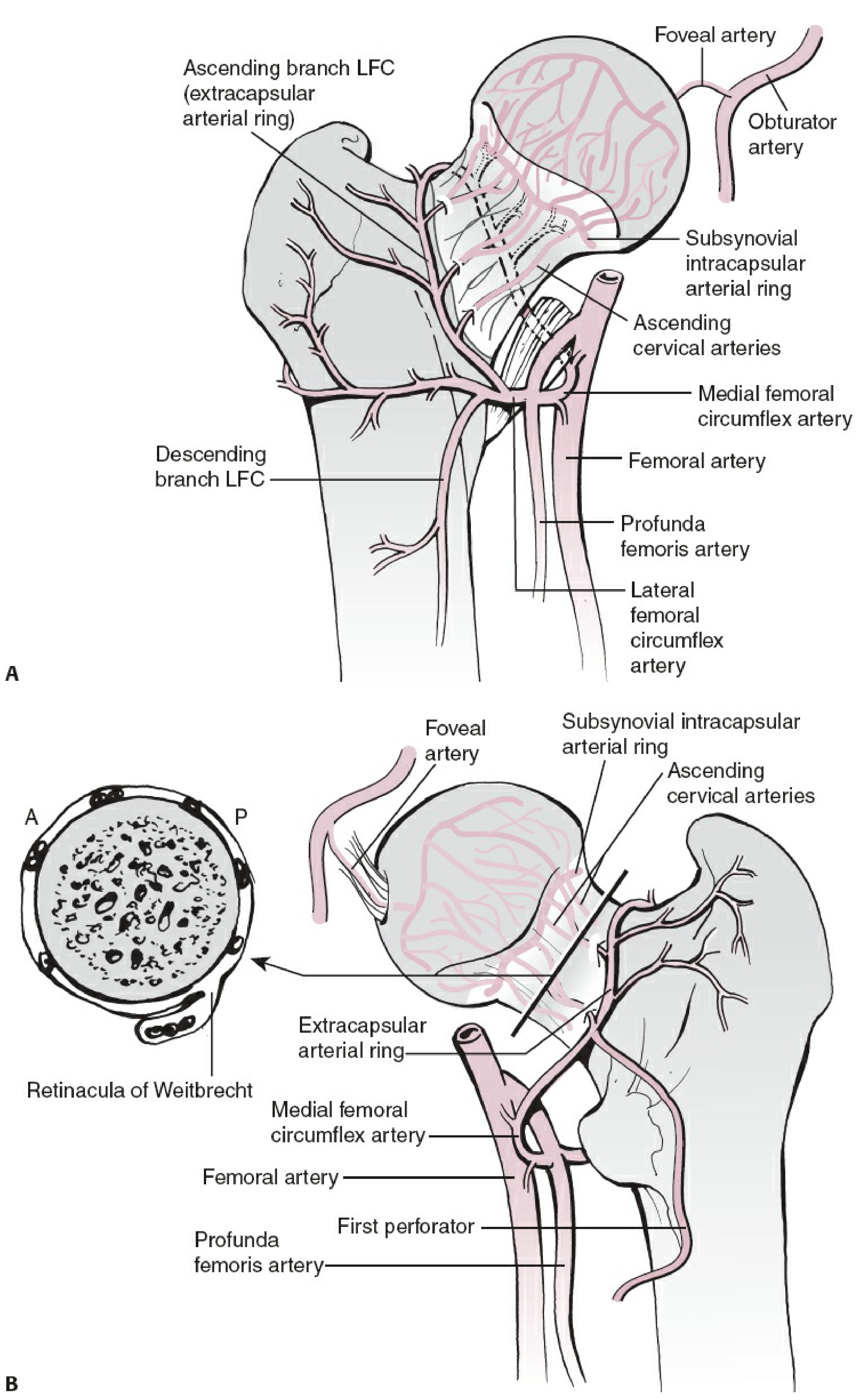
Detailed vascular anatomy showing the extracapsular ring, ascending cervical arteries, subsynovial intracapsular ring, retinacula of Weitbrecht, and the foveal (obturator) artery - Rockwood and Green's Fractures in Adults 10th Ed
Course of the MFCA - Key Surgical Anatomy
The deep branch of the MFCA (the critical branch) winds around the femoral neck posteriorly. It passes:
- Between the iliopsoas tendon and hip capsule anteriorly
- Superior to the obturator externus
- Inferior to the superior gemellus and distal to the piriformis tendon posteriorly
The main terminal branch (the superior retinacular artery) divides into 2-4 terminal vessels that are the main supply to the weight-bearing area of the femoral head.
Surgical implication: To preserve the MFCA during posterior hip approaches, the conjoined tendon should be incised 1.5 cm medial to the trochanteric crest.
Recent Finding: Inferior Gluteal Artery Contribution
A notable recent finding (Rockwood and Green's 10th Ed, 2025) is the contribution of the inferior gluteal artery to femoral head blood supply - either via anastomosis with the MFCA along the inferior border of piriformis, or by a direct branch as a retinacular artery. This anastomosis may be compensatory after MFCA injury.
Clinical Significance
| Feature | Consequence |
|---|---|
| Retinacular vessels run along the femoral neck within the capsule | Displaced intracapsular fractures (especially subcapital) interrupt supply |
| Subcapital fracture | Highest risk of AVN |
| Basicervical fracture | Lowest risk of AVN |
| Intertrochanteric fracture | Below the capsule - blood supply preserved, no AVN risk |
| High intracapsular pressure post-fracture | Tamponade effect further compromises blood flow |
| Revascularization after displaced fracture | Occurs from areas with retained supply + ingrowth from metaphysis |
Avascular necrosis (AVN) of the femoral head occurs when the retinacular vessels are disrupted and the ligamentum teres vessels cannot compensate. The intracapsular femoral neck also lacks a periosteal cambial layer (no periosteal callus), so fracture union depends on endosteal healing alone - explaining prolonged union times.
Sources:
- General Anatomy and Musculoskeletal System, THIEME Atlas of Anatomy, p. 452
- Gray's Anatomy for Students, p. 659-660
- Rockwood and Green's Fractures in Adults 10th Ed 2025, p. 2642-2645
This is a shared conversation. Sign in to Orris to start your own chat.