Mammary glands quadrants
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Here is a complete overview of the mammary gland quadrants drawn from authoritative surgical and pathology textbooks.
Quadrants of the Mammary Gland
The breast is divided into 4 quadrants by a horizontal line and a vertical line, both passing through the nipple-areolar complex:
| Quadrant | Abbreviation | Key Features |
|---|---|---|
| Upper Outer Quadrant | UOQ | Largest quadrant; contains the most glandular tissue; extends into axilla as the axillary tail of Spence |
| Upper Inner Quadrant | UIQ | Smaller; contains less glandular tissue |
| Lower Outer Quadrant | LOQ | Less glandular; mostly fatty tissue |
| Lower Inner Quadrant | LIQ | Smallest amount of glandular tissue |
| Central/Subareolar region | - | Around the nipple; contains lactiferous ducts/sinuses |
Upper Outer Quadrant - Why It Matters
The UOQ is clinically the most important quadrant because it contains the axillary tail of Spence - an extension of breast parenchyma that projects into the axilla through an opening in the deep fascia. This gives it significantly more glandular tissue than any other quadrant.
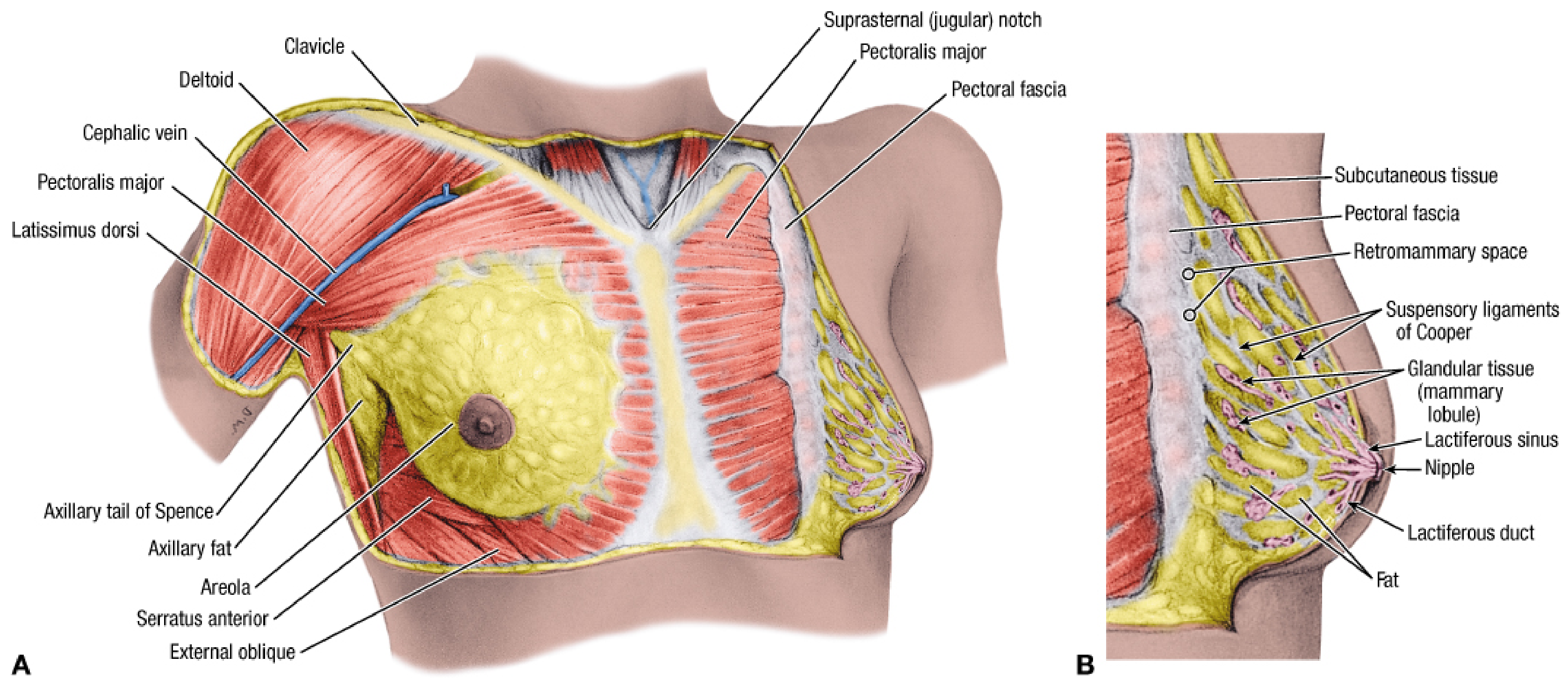
Fischer's Mastery of Surgery, Fig. 51.1 - Breast anatomy showing axillary tail of Spence in the UOQ
Clinical Significance of Quadrants
Frequency of Breast Carcinoma by Quadrant
| Location | Frequency |
|---|---|
| Upper outer quadrant | ~50% |
| Central/subareolar region | ~20% |
| Each remaining quadrant (UI, LO, LI) | ~10% each |
This predominance in the UOQ is directly related to the greater volume of glandular tissue (including the axillary tail).
Lymphatic Drainage by Quadrant
The lymphatic route from each quadrant is clinically important for predicting nodal spread:
- Outer quadrants and subareolar plexus → drain primarily to axillary lymph nodes (~75%); first to the pectoral (anterior/external mammary) Level I nodes
- Inner quadrants → may drain to parasternal (internal mammary) nodes alongside the internal thoracic vessels; also to contralateral breast and abdominal nodes
- All quadrants communicate via the subareolar plexus of Sappey
Axillary nodes are divided into 3 levels relative to pectoralis minor:
- Level I - inferior axilla (lateral to pec minor)
- Level II - midaxilla (behind pec minor)
- Level III - superior axilla (medial to pec minor)
Other Conditions by Quadrant
- Fibroadenosis (fibrocystic change) - most common in the UOQ and axillary tail
- Fibroadenoma - more commonly found in the lower half of the breast, though may occur anywhere
- Carcinoma - can occur in any quadrant including the axillary tail, but predominates in UOQ
- Retraction/dimpling of the nipple toward the UOQ is a classic sign of carcinoma in that region (tethering by Cooper's ligaments and tumor fibrosis)
Internal Organization (Lobar Architecture)
The glandular parenchyma is organized into 15-20 lobes arranged radially around the nipple, with each lobe drained by a lactiferous duct opening at the nipple apex. These pyramidal lobes:
- Are separated by the suspensory ligaments of Cooper (fibro-collagenous septa anchoring skin to deep fascia)
- Cooper's ligaments are more pronounced superiorly than inferiorly
- Glandular tissue is concentrated centrally; adipose tissue lies more peripherally
- The breast lies within the superficial fascia, which provides the surgical dissection plane; its posterior surface overlies the fasciae of pectoralis major, serratus anterior, external oblique, and rectus sheath
Sources: Fischer's Mastery of Surgery (8th ed.), Robbins & Cotran Pathologic Basis of Disease, S. Das Manual on Clinical Surgery (13th ed.)
Lesser sac Epiploic foramen applied Morrison pouch
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Here is a detailed breakdown of the Lesser Sac, Epiploic Foramen, and Morrison's Pouch with clinical applications.
1. Lesser Sac (Omental Bursa)
The lesser sac is a smaller subdivision of the peritoneal cavity located posterior to the stomach and lesser omentum and anterior to the retroperitoneal structures. It communicates with the greater sac through the epiploic (omental) foramen.
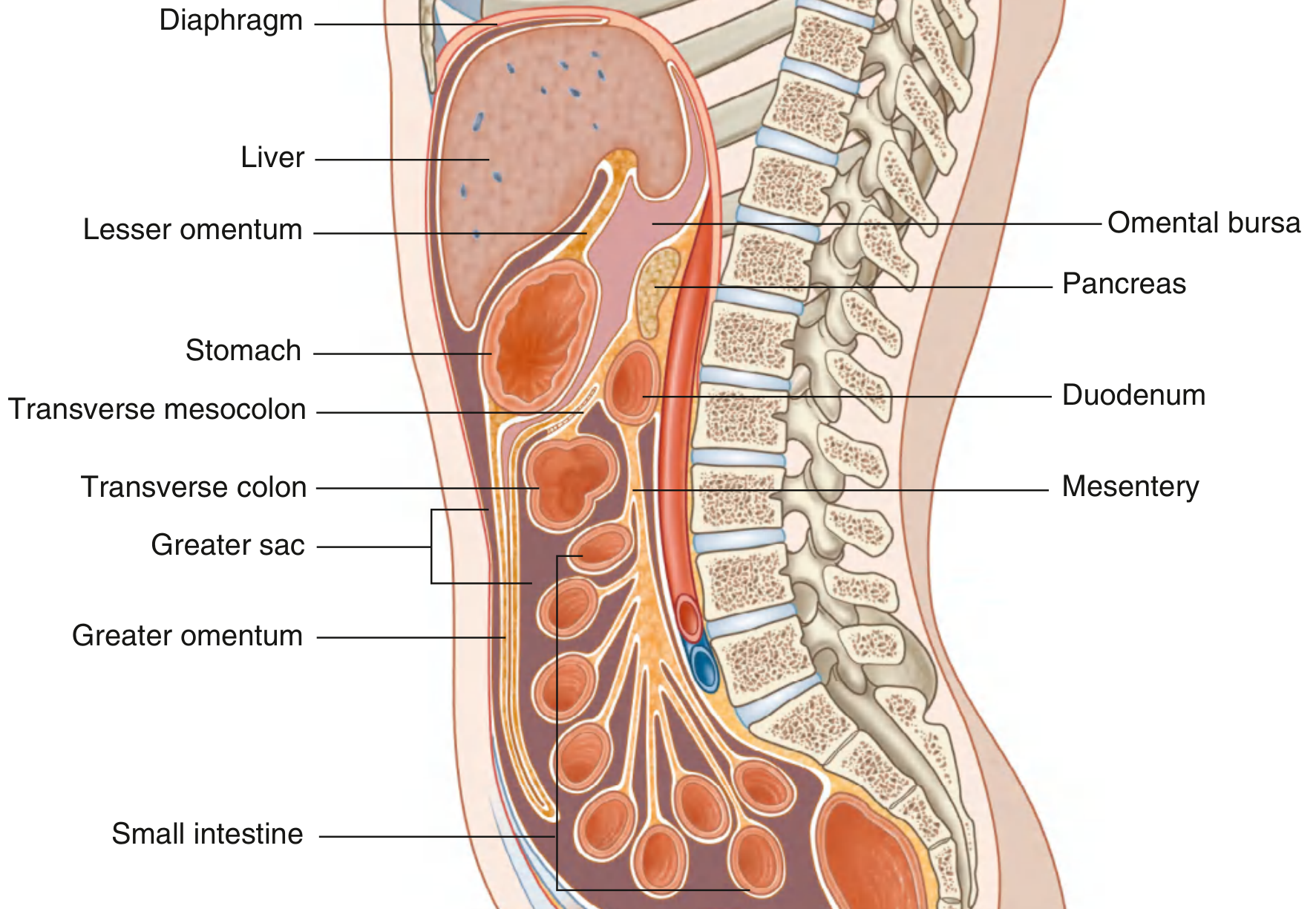
Gray's Anatomy for Students - Sagittal view: Greater sac vs. Omental bursa (lesser sac)
Boundaries of the Lesser Sac
| Wall | Structures |
|---|---|
| Anterior | Stomach, lesser omentum (hepatogastric + hepatoduodenal ligaments), posterior wall of stomach |
| Posterior | Parietal peritoneum overlying pancreas, left kidney, left suprarenal, aorta, IVC |
| Superior | Caudate lobe of liver, diaphragm |
| Inferior | Transverse colon and transverse mesocolon |
| Right | Epiploic foramen (only communication with greater sac) |
| Left | Gastrosplenic ligament, splenorenal ligament |
Recesses of the Lesser Sac
- Superior recess - extends upward behind the caudate lobe of the liver to the diaphragm
- Inferior recess - extends downward between the layers of the greater omentum
- Splenic recess - extends to the left toward the hilum of the spleen between the gastrosplenic and splenorenal ligaments
Clinical Significance of the Lesser Sac
- Posterior gastric ulcer perforation - gastric contents leak into the lesser sac, causing perigastric abscess formation contained within the bursa (rather than spreading to the greater peritoneal cavity)
- Acute pancreatitis - pancreatic enzymes/pseudocysts collect in the lesser sac (posterior relation to pancreas)
- Lesser sac abscess - presents insidiously because the sac is walled off; diagnosed by CT; drained surgically or radiologically
2. Epiploic Foramen (Foramen of Winslow / Omental Foramen)
The only communication between the lesser sac and the greater peritoneal cavity. It is a slit-like opening, about 3 cm wide, located at the right free margin of the lesser omentum.
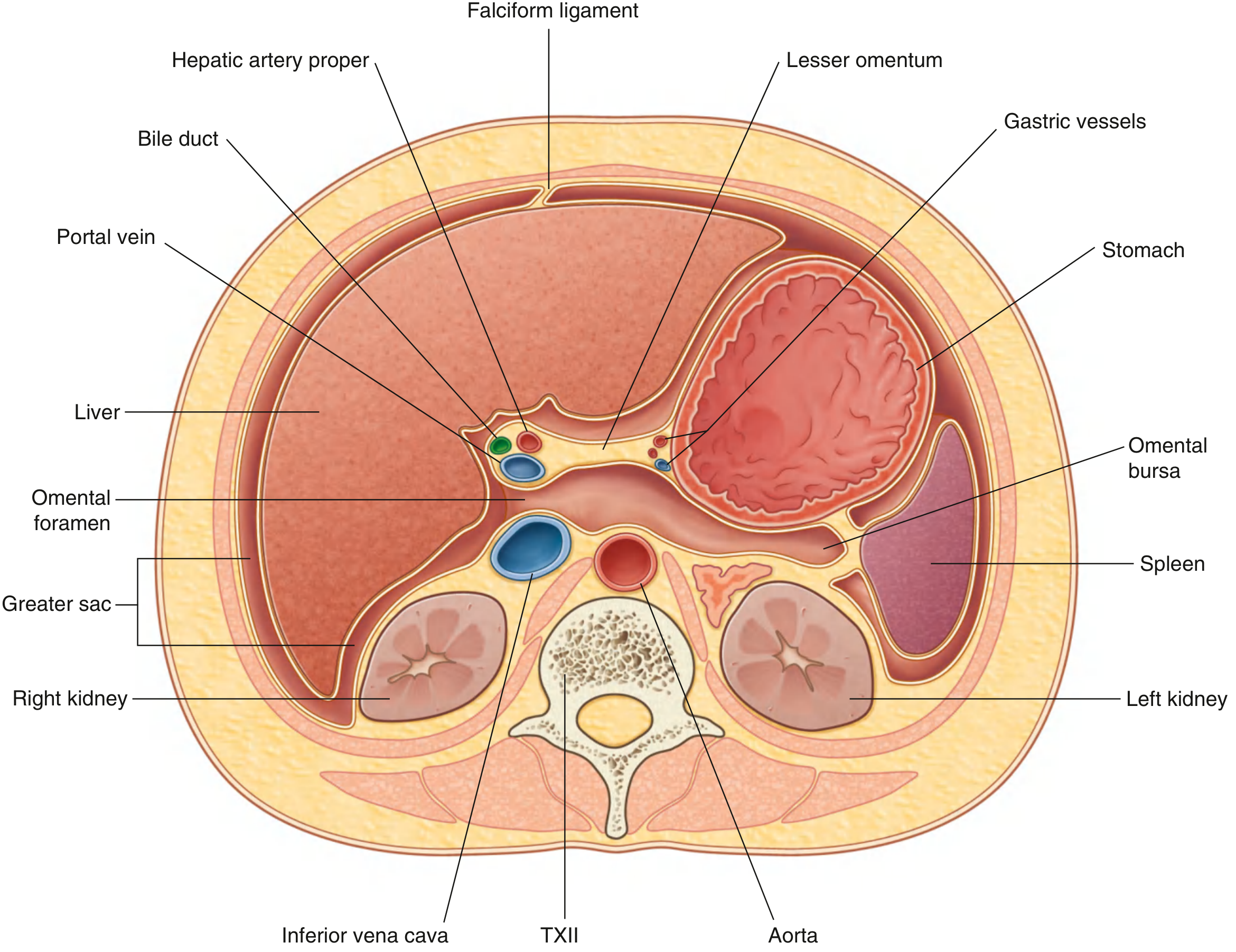
Gray's Anatomy for Students - Transverse section showing continuity between greater and lesser sacs through the omental foramen
Boundaries of the Epiploic Foramen
| Border | Structure |
|---|---|
| Anterior | Hepatoduodenal ligament (free right edge of lesser omentum), containing the portal triad: portal vein (posterior), hepatic artery proper (anterior-left), common bile duct (anterior-right) |
| Posterior | Inferior vena cava (IVC), covered by peritoneum |
| Superior | Caudate lobe (lobe 1) of the liver |
| Inferior | First part of the duodenum (D1) |
Contents of the Hepatoduodenal Ligament (Anterior Wall of Foramen)
Remembered by the mnemonic "BHA" from right to left:
- B - Bile duct (CBD) - rightmost, anterior
- H - Hepatic artery proper - left anterior
- A - portal vein (behind both, posterior)
Clinical Applications of the Epiploic Foramen
-
Pringle Maneuver - a finger is placed through the epiploic foramen to compress the hepatoduodenal ligament between thumb and index finger, occluding the portal vein and hepatic artery. This controls hepatic inflow hemorrhage during liver surgery or trauma. The common bile duct is also within the ligament so it is compressed simultaneously. - Fischer's Mastery of Surgery, p. 4493
-
Herniation through the epiploic foramen - a rare internal hernia where bowel loops (typically small intestine) prolapse through the foramen into the lesser sac, causing intestinal obstruction. It is a surgical emergency requiring manual reduction.
-
Gallstone ileus - a large gallstone can erode from the gallbladder into the duodenum (Mirizzi's area) and impact distally; the epiploic foramen region is a landmark in hepatobiliary surgery.
-
Access to lesser sac - surgeons enter the lesser sac via the epiploic foramen or by dividing the gastrocolic ligament to access the pancreatic body/tail, posterior gastric wall, or to drain collections.
3. Morrison's Pouch (Hepatorenal Recess / Hepatorenal Fossa)
Morrison's pouch is the peritoneal space between the right lobe of the liver (visceral surface) and the right kidney/right adrenal gland. It lies within the right subhepatic space.
Why it matters - Most Dependent Point
In the supine position, Morrison's pouch is the most dependent (lowest) part of the peritoneal cavity in the right upper quadrant, making it the first site where free intraperitoneal fluid accumulates. This is because:
- It lies posterior to the liver and anterior to the right kidney
- Gravity directs fluid here when the patient lies flat
- It is separated from the liver by peritoneum and from the kidney by the hepatorenal ligament
Clinical Applications of Morrison's Pouch
| Scenario | Relevance |
|---|---|
| FAST exam (Focused Assessment with Sonography in Trauma) | The RIGHT UPPER QUADRANT view directly targets Morrison's pouch; even 200-250 mL of free fluid is detectable here on ultrasound |
| Free intraperitoneal fluid (haemoperitoneum, ascites) | First or most prominent collection in supine patients |
| Subhepatic abscess | Forms in Morrison's pouch after perforation or post-operative infection (e.g., perforated duodenal ulcer, post-cholecystectomy) |
| Pneumoperitoneum | Free air is visible in the right upper quadrant adjacent to the liver; Rigler's sign (double bowel wall sign) is sought here |
| Right paracolic gutter communication | Fluid from Morrison's pouch can track down the right paracolic gutter to the right iliac fossa and pelvis - explaining why appendix/duodenal perforations cause right iliac fossa signs |
Relation of Morrison's Pouch to Other Peritoneal Recesses
SUPRAHEPATIC SPACE
↓ (right subphrenic space)
MORRISON'S POUCH (right subhepatic/hepatorenal)
↓
RIGHT PARACOLIC GUTTER
↓
PELVIS (rectouterine / rectovesical pouch = pouch of Douglas)
Fluid follows this right-sided pathway preferentially when a patient is supine, which explains why right-sided visceral perforations can present with pelvic signs - Sabiston Textbook of Surgery
Summary Table
| Structure | Key Feature | Clinical Relevance |
|---|---|---|
| Lesser sac | Behind stomach; bounded by liver, stomach, pancreas | Site of perigastric abscess, pancreatitis collections |
| Epiploic foramen | Only communication between lesser and greater sac; bounded by CBD/HA/PV (anterior), IVC (posterior), caudate lobe (superior), D1 (inferior) | Pringle maneuver; internal hernia |
| Morrison's pouch | Hepatorenal recess; most dependent point in supine position | FAST exam; first site of free fluid accumulation |
Sources: Gray's Anatomy for Students, Fischer's Mastery of Surgery (8th ed.), Color Atlas of Human Anatomy Vol. 2, Yamada's Textbook of Gastroenterology, Sabiston Textbook of Surgery, Schwartz's Principles of Surgery (11th ed.)
This is a shared conversation. Sign in to Orris to start your own chat.