Raised ICP measures
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I now have excellent content from multiple textbooks plus the key protocol flowchart image. Let me compile the comprehensive answer.
Raised Intracranial Pressure (ICP) - Management
Physiology Recap
The Monro-Kellie doctrine states the skull is a rigid compartment containing brain tissue (~80%), CSF (~10%), and blood (~10%). Any additional volume initially displaces venous blood and CSF. Once this compensation is exhausted, ICP rises exponentially - small further increases cause rapid deterioration and herniation.
Normal ICP: 5-15 mmHg
Key equation:
CPP = MAP - ICP Normal CPP = 75-105 mmHg (MAP 90-110 minus ICP 5-15)
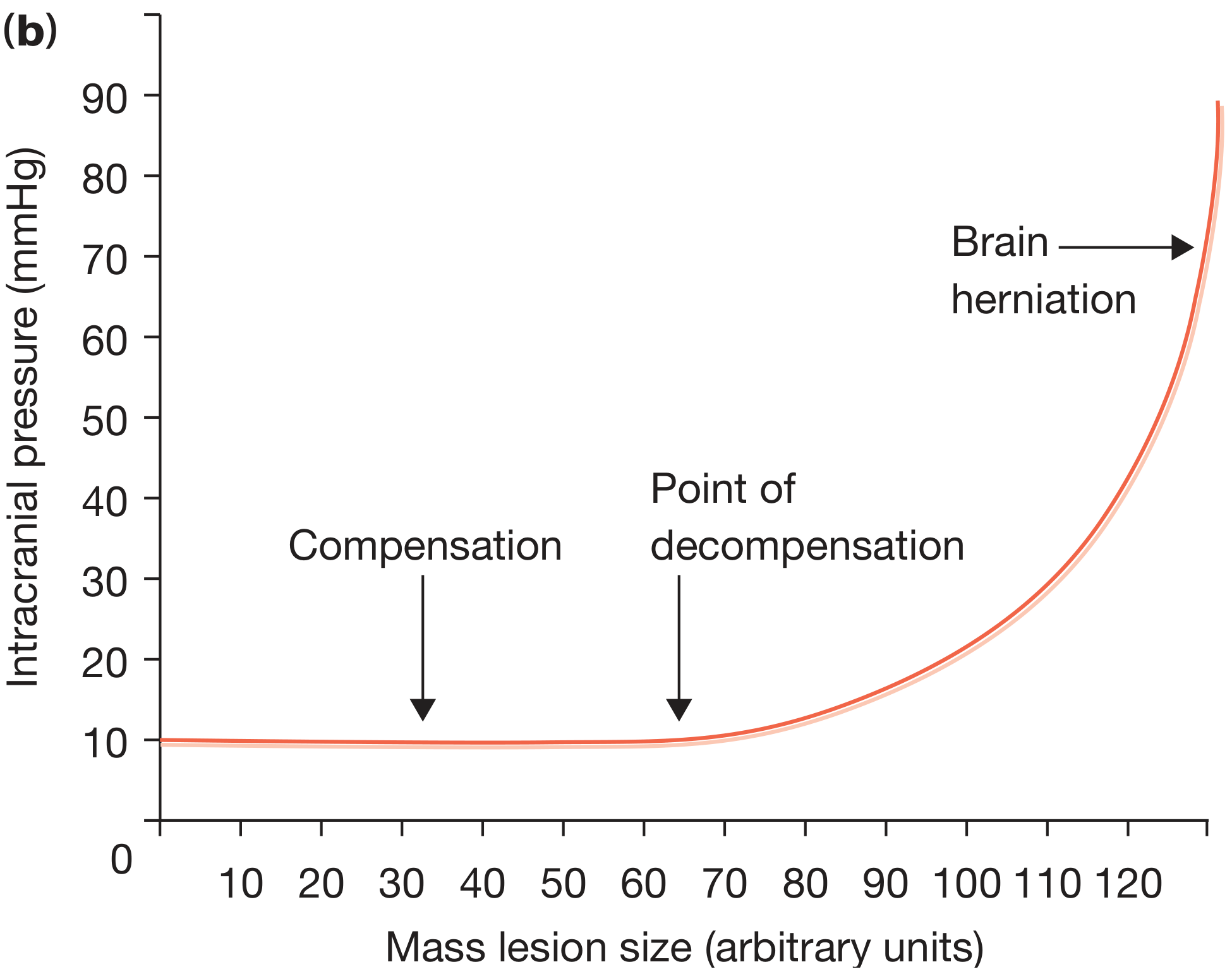
Figure: As mass lesion size increases, ICP remains near-normal during compensation, then rises exponentially past the point of decompensation, culminating in herniation. (Bailey & Love, p. 382)
Indications for ICP Monitoring
ICP monitoring is recommended in:
- Severe TBI (GCS ≤ 8) with an abnormal CT scan
- Severe TBI with normal CT if ≥ 2 of: age >40 years, unilateral/bilateral motor posturing, systolic BP <90 mmHg
- Acute subarachnoid hemorrhage with coma or neurological deterioration
- Intracranial hemorrhage with intraventricular blood
- Ischemic MCA stroke (malignant)
- Fulminant hepatic failure with coma and cerebral edema on CT
- Global cerebral ischemia/anoxia with cerebral edema on CT
ICP > 20 mmHg is associated with unfavorable outcomes in TBI. Treatment threshold is generally ICP > 20-22 mmHg or CPP < 50-60 mmHg.
ICP monitors: Ventriculostomy (gold standard - allows CSF drainage + measurement), parenchymal, subdural, or epidural transducers.
Treatment Protocol
The measures below should be administered simultaneously, not sequentially.
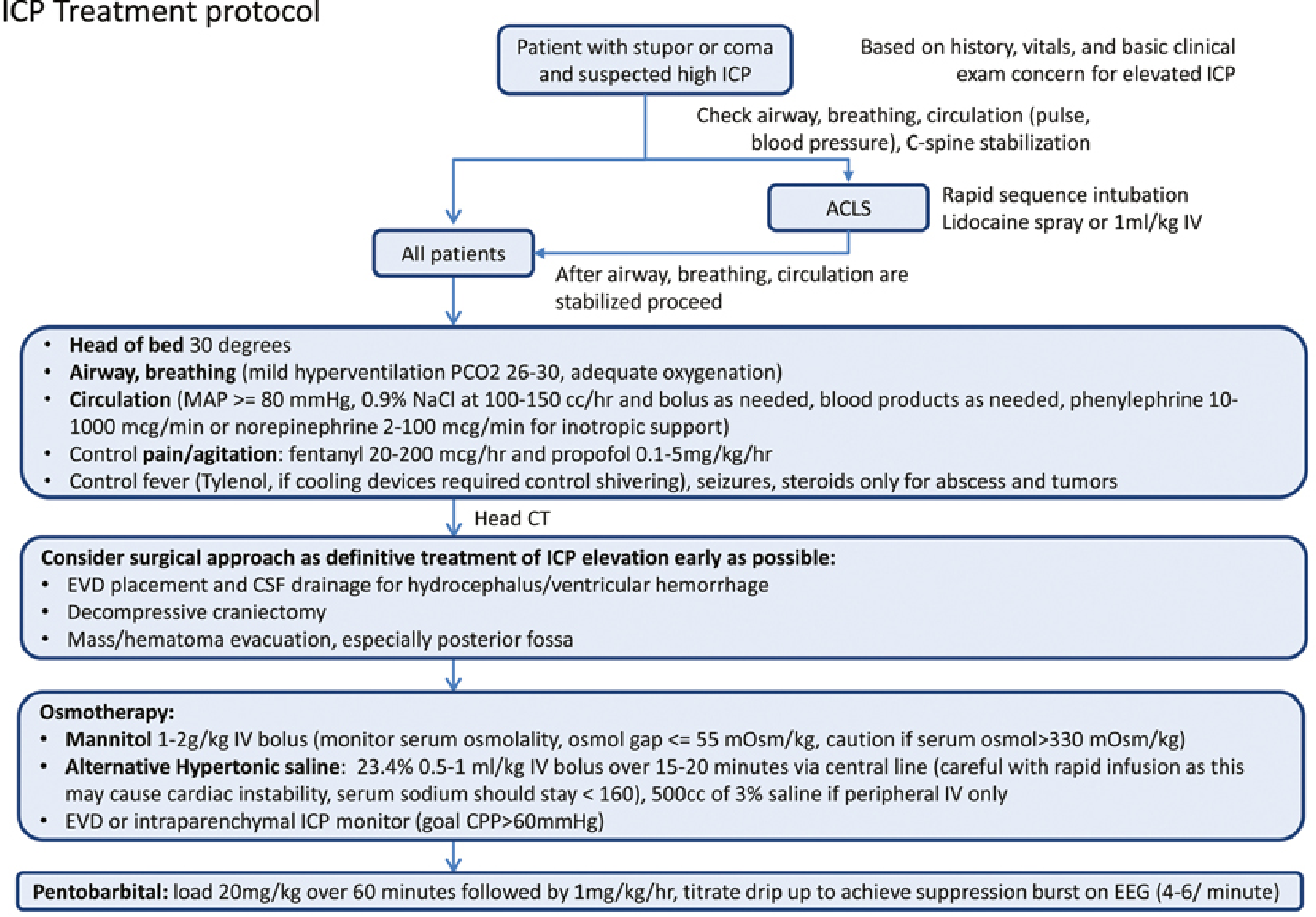
Figure: ICP treatment protocol - Plum & Posner's Diagnosis and Treatment of Stupor and Coma, p. 541
Step 1 - Immediate Stabilization (All Patients)
| Measure | Detail |
|---|---|
| Airway/C-spine | Rapid sequence intubation (RSI) with IV lidocaine premedication |
| Head positioning | HOB elevated to 30 degrees, head midline (optimizes jugular venous drainage) |
| Hyperventilation | Target PCO2 26-30 mmHg - vasoconstrictive, temporizing measure only. Never let PCO2 drop below 25 mmHg |
| Oxygenation | Maintain SpO2 >95%, confirm with ABG |
| MAP maintenance | Target MAP ≥ 80 mmHg using isotonic fluids (0.9% NaCl 100-150 cc/hr); vasopressors if needed (phenylephrine 10-1000 mcg/min or norepinephrine 2-100 mcg/min) |
| Avoid hypotonic fluids | Worsens cerebral edema |
| Pain control | Fentanyl 20-200 mcg/hr IV (short-acting, least BP effect); morphine 2-4 mg IV q2-4h as alternative |
| Sedation/agitation | Propofol 0.1-5 mg/kg/hr or benzodiazepines |
| Fever control | Antipyretics (acetaminophen); cooling devices if needed (control shivering) |
| Seizure control | Treat promptly |
| Steroids | Only for vasogenic edema (brain tumors, abscess) - NO role in TBI or cytotoxic edema |
Step 2 - Head CT and Surgical Options (Definitive Treatment)
Get urgent CT head for all patients with suspected raised ICP.
| Intervention | Indication |
|---|---|
| External ventricular drain (EVD) | Hydrocephalus, intraventricular hemorrhage - allows CSF drainage + ICP monitoring |
| Mass/hematoma evacuation | Space-occupying lesions, especially cerebellar hemorrhages |
| Decompressive craniectomy | Refractory raised ICP, malignant MCA infarct |
Do not delay empiric pharmacological treatment while awaiting imaging when herniation is clinically suspected.
Step 3 - Osmotherapy
Used when general measures are insufficient.
Mannitol (first-line osmotic agent):
- Dose: 0.5-1 g/kg (some sources: 1-2 g/kg) IV over 15 minutes as bolus
- Replaces urinary losses with normal saline
- Monitor serum osmolality - caution if >330 mOsm/kg; osmol gap should stay ≤ 55 mOsm/kg
- Mechanism: osmotic gradient draws water from brain into vasculature; also reduces blood viscosity
Hypertonic saline (alternative):
- 23.4%: 0.5-1 mL/kg IV bolus over 15-20 minutes via central line
- 3%: 500 mL IV if only peripheral access
- Caution in: chronic hyponatremia, cardiac instability, pulmonary edema
- Target serum sodium <160 mEq/L
- Check serum Na+ and osmolality regularly for both agents
Step 4 - Refractory ICP (Last Resort)
Barbiturate coma:
- Pentobarbital: load 20 mg/kg IV over 60 minutes, then 1 mg/kg/hr maintenance
- Titrate up to 3 mg/kg/hr to achieve burst suppression on EEG (4-6 bursts/min)
- Major side effect: hypotension - monitor closely
- Alternative: thiopental
Hypothermia: Role in TBI is unclear; not routinely recommended.
Brain Herniation Syndromes (Consequence of Uncorrected Raised ICP)
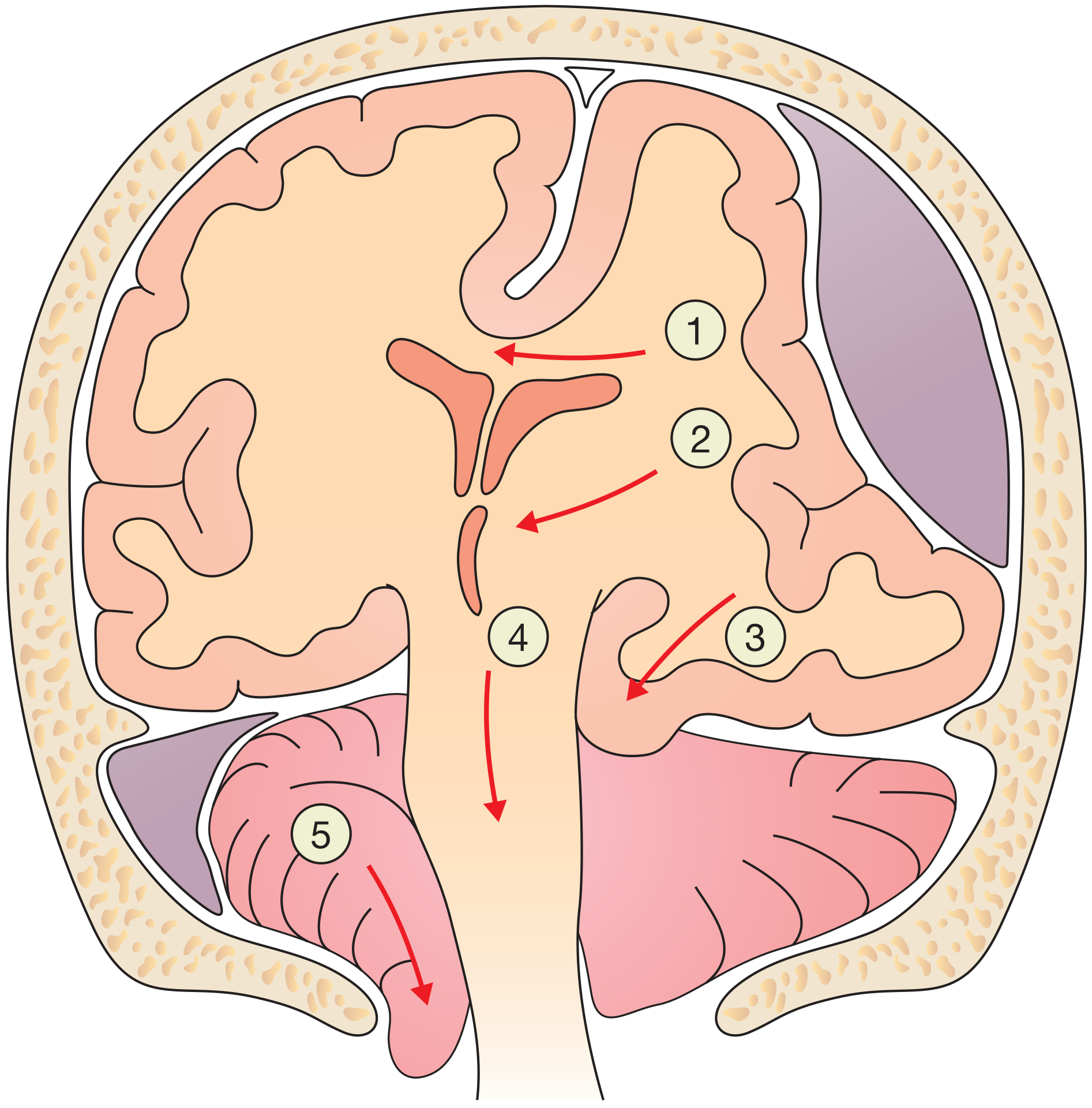
Figure: Brain herniation. (1) Subfalcine - cingulate gyrus under falx. (2) Midline shift. (3) Uncal - temporal lobe over tentorium, compresses CN III (pupil dilation). (4) Central herniation. (5) Tonsillar - cerebellar tonsils through foramen magnum, compresses medullary vasomotor and respiratory centres. (Bailey & Love, p. 382-383)
| Syndrome | Location | Key Sign |
|---|---|---|
| Subfalcine | Cingulate under falx | Midline shift |
| Uncal (transtentorial) | Temporal lobe over tentorium | Ipsilateral dilated pupil (CN III palsy) |
| Central | Downward displacement | Bilateral signs, Cushing's triad |
| Tonsillar | Cerebellar tonsils through foramen magnum | Cushing's triad: hypertension + bradycardia + irregular respiration |
Cerebral Perfusion Pressure (CPP) Targets
- Target CPP 50-70 mmHg (exact target debated; Brain Trauma Foundation recommends 60-70 mmHg)
- Can increase CPP by raising MAP (vasopressors) or by reducing ICP (measures above)
- CPP <50 mmHg = cerebral ischemia risk
- Cerebral autoregulation normally maintains constant CBF with MAP 50-150 mmHg, but this is impaired in trauma
Sources: Plum & Posner's Diagnosis and Treatment of Stupor and Coma (pp. 541-543); Bailey & Love's Short Practice of Surgery, 28th ed. (pp. 382-383); Schwartz's Principles of Surgery, 11th ed. (pp. 475-476)
This is a shared conversation. Sign in to Orris to start your own chat.