What are extra articular and intra articular fractures
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Finding Sources
Reading File
Finding Sources
Finding Sources
I now have comprehensive information from authoritative orthopedic textbooks. Let me compile a thorough answer.
Extra-Articular vs. Intra-Articular Fractures
This is a fundamental classification in orthopedic trauma that determines how a fracture is treated and what complications to expect.
The Core Distinction
The key question in classifying any fracture near a joint is: does the fracture line enter the joint surface?
- Extra-articular fracture - the fracture line does NOT enter the articular (joint) surface
- Intra-articular fracture - the fracture line enters and disrupts the articular (joint) surface
The diagram below (from Rockwood and Green's Fractures in Adults, 10th ed.) illustrates all three types in the OTA/AO system:
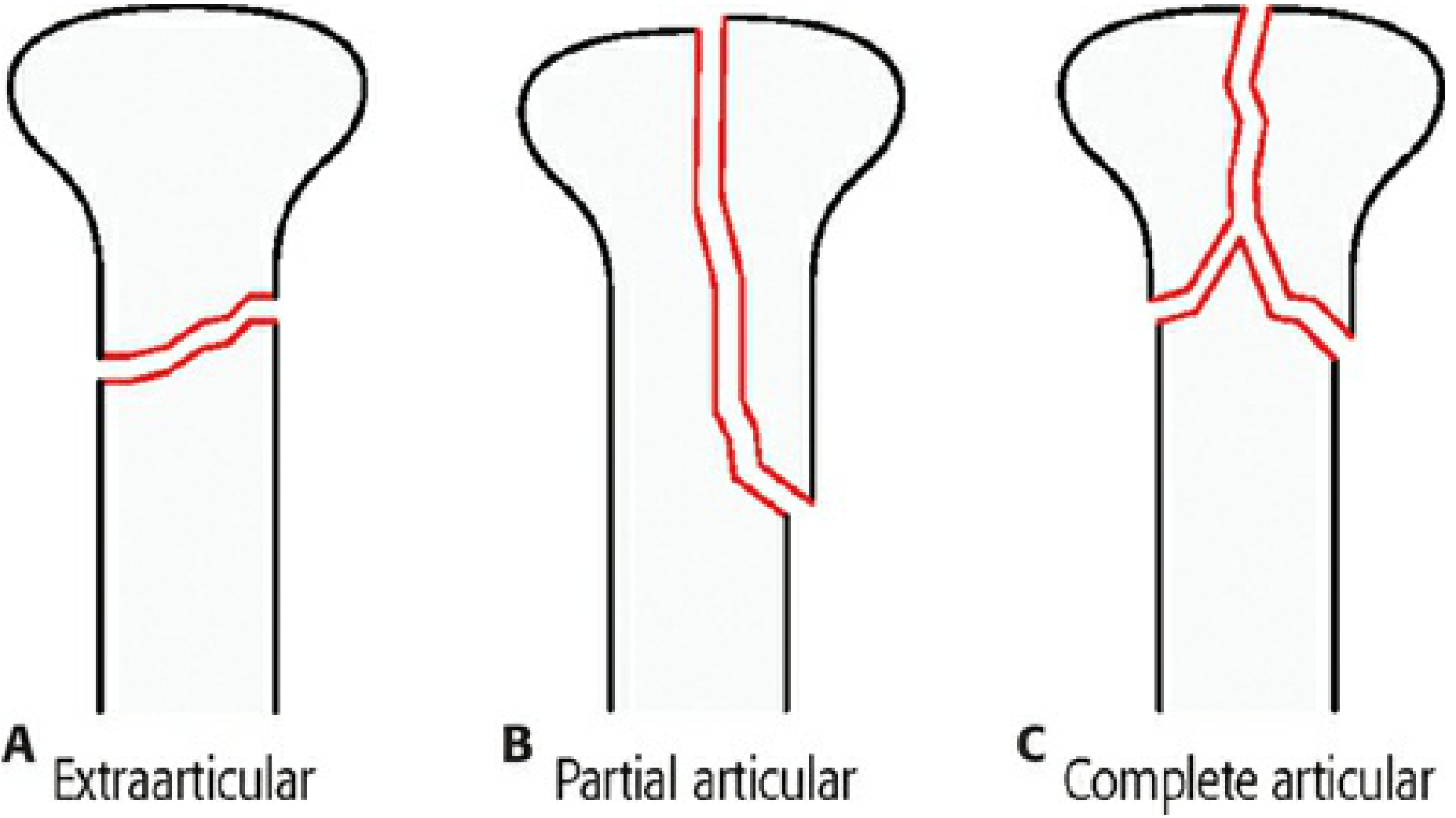
OTA/AO Classification of End-Segment Fractures
The OTA/AO classification system (the global standard) categorizes end-segment (metaphyseal/epiphyseal) fractures into three types based on articular involvement:
| Type | Name | Definition |
|---|---|---|
| A | Extra-articular | No fracture lines enter the articular surface |
| B | Partial articular (intra-articular) | Part of the articular surface is fractured; the remainder is intact and still connected to the diaphysis |
| C | Complete articular (intra-articular) | The articular surface is completely separated from the diaphysis - the most severe type |
"Type A: Extra-articular. There are no fracture lines that enter the articular surface. Type B: Partial articular. The fracture involves only part of the articular surface, and the remainder of the joint is intact and connected to the supporting end segment. Type C: Complete articular. The fracture or fractures disrupt the articular surface such that the articular surface is completely separated from the diaphysis."
- Rockwood and Green's Fractures in Adults, 10th ed.
Extra-Articular Fractures
Definition: The fracture line lies within the metaphysis or epiphysis but does not breach the joint surface.
Examples:
- Colles' fracture (most distal radius fractures)
- Metacarpal shaft/neck fractures
- Surgical neck of humerus fractures (Neer A-type)
- Supracondylar humerus fractures (in children)
- Stress fractures of the pubic rami
Goals of treatment:
- Restore mechanical alignment of the joints above and below
- Achieve acceptable length, alignment, and rotation
- Perfect anatomical reduction of individual fragments is NOT required
- Secondary bone healing (relative stability) is acceptable
Key point in children: Extra-articular fractures have remodeling potential, so a greater degree of displacement can be accepted - particularly in the plane of the joint and near growth plates.
Intra-Articular Fractures
Definition: The fracture line enters and disrupts the joint (articular) surface.
Examples:
- Bennett's fracture (intra-articular base of thumb metacarpal)
- Rolando's fracture (comminuted intra-articular base of thumb metacarpal)
- Tibial plateau fractures
- Pilon (distal tibia) fractures
- Calcaneal fractures (Sanders classification)
- Distal radius intra-articular fractures
- Femoral head/neck fractures extending into the hip joint
- Acetabular fractures
Goals of treatment (stricter):
- Anatomic reduction of the articular surface - step-off or gap must be minimized
- Interfragmentary compression for absolute stability
- Early range of motion to prevent joint stiffness
- The acceptable residual displacement depends on the joint: e.g., 2 mm may be acceptable at the patella or tibial plateau, but is NOT acceptable at the condylar joints of the fingers
"The goals of surgical treatment of an intra-articular fracture include anatomic reduction and interfragmentary compression of the articular surface with absolute stability and early range of motion."
- Rockwood and Green's Fractures in Adults, 10th ed.
Why This Distinction Matters
| Feature | Extra-Articular | Intra-Articular |
|---|---|---|
| Fracture line | Outside joint | Enters/crosses joint |
| Reduction goal | Mechanical alignment | Anatomic (near-perfect) reduction |
| Stability needed | Relative stability acceptable | Absolute stability required |
| Bone healing | Primary or secondary | Primary (compression + rigid fixation) |
| Main complication | Malunion, limb shortening | Post-traumatic arthritis, joint stiffness |
| Fixation urgency | Lower | Higher - articular congruity is time-sensitive |
| Children | Remodeling potential - more displacement accepted | Joint surface does NOT remodel reliably |
Surgical strategy: When a complete articular (OTA C) fracture is fixed, surgeons first reduce and compress the articular surface, effectively converting it back to an extra-articular (OTA A) or partial articular (OTA B) fracture. They then apply extra-articular fracture principles (restore length, alignment, rotation) to the remaining metaphyseal component.
Why Intra-Articular Fractures Are More Serious
- Post-traumatic arthritis - even small (1-2 mm) step-offs in the articular cartilage cause uneven load distribution, accelerating cartilage wear
- Joint stiffness - hemarthrosis and prolonged immobilization damage hyaline cartilage
- Avascular necrosis - certain intra-articular fractures (e.g., femoral neck, talus) disrupt blood supply to the joint
- Harder to reduce - comminuted articular fragments ("die-punch" fragments) may not hold fixation
- More demanding surgery - requires visualization of the joint surface, often with fluoroscopy or arthroscopy to confirm reduction
Sources: Rockwood and Green's Fractures in Adults, 10th ed. (2025), pp. 958-960, 1382-1386; Bailey and Love's Short Practice of Surgery, 28th ed., pp. 4927-4959
This is a shared conversation. Sign in to Orris to start your own chat.