: Etiology, Pathophysiology, and Clinical Features* Topics to cover: - Causes of congenital hydrocephalus - Causes of acquired hydrocephalus - Pathophysiology - Clinical features in infants - Clinical features in older children - Differential diagnosis of enlarged head
Etiology, Pathophysiology, and Clinical Features* Topics to cover: - Causes of congenital hydrocephalus - Causes of acquired hydrocephalus - Pathophysiology - Clinical features in infants - Clinical features in older children - Differential diagnosis of enlarged head
Reading File
Finding Sources
Finding Sources
Searching PubMed
"hydrocephalus"[MeSH Terms] AND "etiology"[MeSH Terms]
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have comprehensive, detailed content from multiple authoritative textbooks. I have enough to write a thorough, well-structured answer. Let me now compile the final response.
Hydrocephalus: Etiology, Pathophysiology, and Clinical Features
Definition and Classification
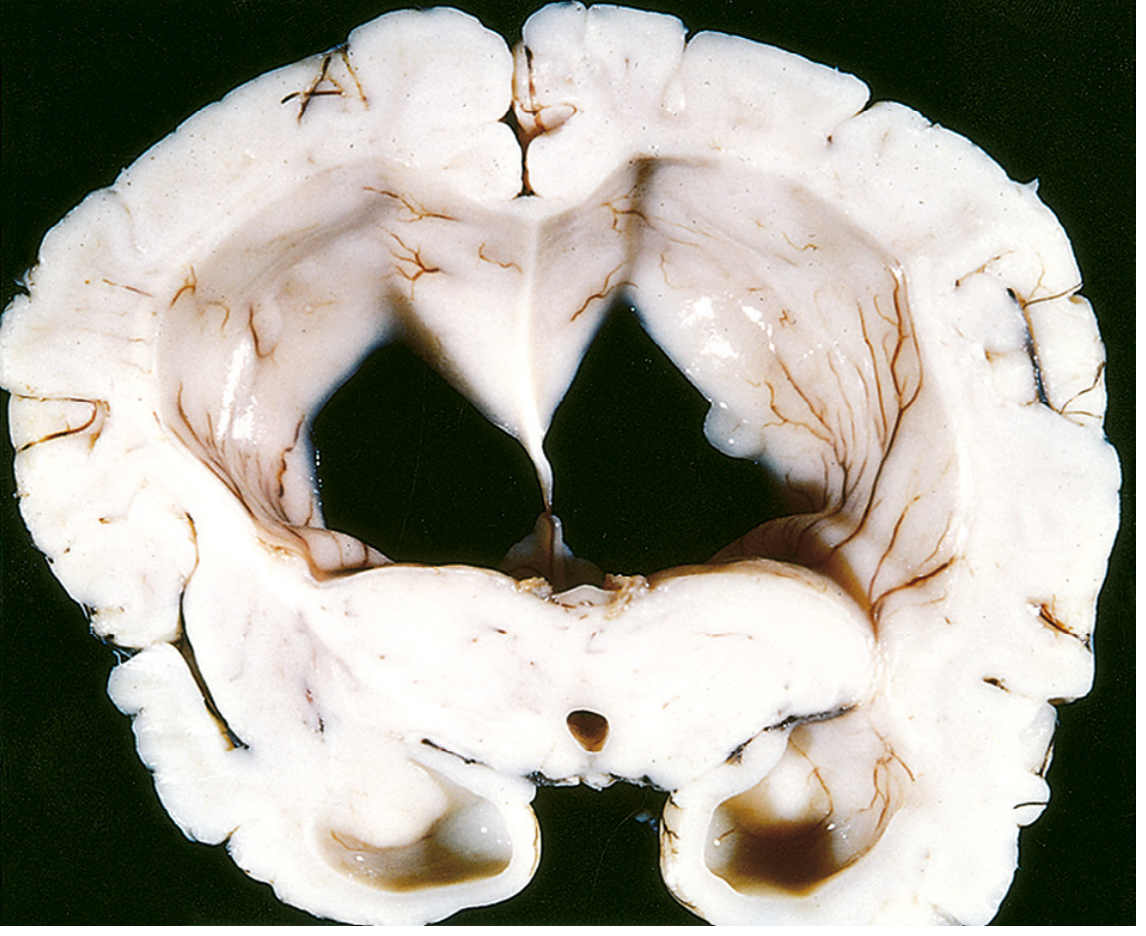
Hydrocephalus is the accumulation of excessive CSF within the ventricular system, leading to ventricular enlargement (Fig. 28.3, below). The vast majority of cases result from impaired flow or resorption of CSF; overproduction is a rare cause, seen only with choroid plexus tumors.
Two classical types:
| Type | Definition | Obstruction site |
|---|---|---|
| Noncommunicating (Obstructive) | Obstruction within the ventricular system; ventricles not in free communication with subarachnoid space | Intraventricular: foramina of Monro, aqueduct of Sylvius, foramina of Magendie/Luschka |
| Communicating | Obstruction outside the ventricular system; CSF still reaches subarachnoid space | Basal cisterns, arachnoid granulations, subarachnoid space |
| Hydrocephalus ex vacuo | Compensatory ventricular enlargement due to loss of brain parenchyma; NOT true hydrocephalus | Not obstructive - no raised ICP |
1. Causes of Congenital Hydrocephalus
Congenital hydrocephalus is present at birth or develops in the first months of life, before cranial suture fusion.
Obstructive (Noncommunicating) Causes
Aqueductal Stenosis / Gliosis
- The most common congenital cause
- The cerebral aqueduct (of Sylvius) is narrow or replaced by several minute channels
- In a few cases, transmitted as an X-linked recessive trait (L1CAM gene mutation)
- Most cases result from fetal viral infection - especially cytomegalovirus (CMV) or Toxoplasma gondii
- Results in dilatation of lateral ventricles and third ventricle, with normal-sized fourth ventricle
Chiari Malformations
- Chiari II malformation: downward displacement of cerebellar structures through the foramen magnum; almost always associated with lumbosacral myelomeningocele. Hydrocephalus typically becomes manifest after surgical repair of the myelomeningocele
- Chiari I malformation: less commonly associated with hydrocephalus
Dandy-Walker Malformation
- Congenital failure of opening of the foramina of Luschka and Magendie
- Cystic dilation of the fourth ventricle, hypoplasia/absence of the cerebellar vermis
- Causes noncommunicating hydrocephalus with enlargement of all ventricles
Other Structural Malformations
- Congenital midline tumors (e.g., tectal glioma)
- Vein of Galen malformation (arteriovenous malformation causing venous hypertension)
- Holoprosencephaly with single ventricle
Communicating Congenital Causes
- Congenital absence or deficient number of arachnoid villi
- Intrauterine subarachnoid hemorrhage causing basal cisternal fibrosis
- Intraventricular hemorrhage in premature infants: premature infants < 1500 g have a high risk of intraventricular hemorrhage; approximately 25% develop progressive ventricular enlargement, and 5% ultimately require shunting
2. Causes of Acquired Hydrocephalus
Acquired hydrocephalus develops after birth, with a previously normal CSF circulation.
Post-Infectious (Postinfective)
- Bacterial meningitis - the most common acquired cause; fibrinous exudate causes scarring at the basal cisterns and foramina of Magendie/Luschka, blocking CSF flow
- Tuberculous meningitis - creates dense basal exudate that obliterates cisterns
- Viral encephalitis - can cause ependymitis and aqueductal obstruction
- Fungal meningitis (e.g., Cryptococcus) - granulomatous occlusion of subarachnoid pathways
Post-Hemorrhagic
- Intraventricular hemorrhage (IVH) - blood in CSF triggers arachnoid fibrosis; the most common acquired cause in neonates (from germinal matrix hemorrhage in prematurity)
- Subarachnoid hemorrhage (SAH) - ruptures into cisterns, fibrin blocks CSF absorption
- Cerebellar hemorrhage or infarct - directly compresses fourth ventricle outlet
Neoplastic
- Posterior fossa tumors are the most common cause in older children: medulloblastoma, ependymoma, cerebellar astrocytoma - all obstruct the fourth ventricular outflow or aqueduct
- Colloid cyst of third ventricle - blocks both foramina of Monro, causing bilateral lateral ventricular dilatation
- Tectal plate glioma - causes aqueductal stenosis
- Choroid plexus papilloma - rare cause by overproduction of CSF (often with concurrent obstruction)
Inflammatory / Other
- Normal pressure hydrocephalus (NPH) - adults; communicating; associated with prior SAH, meningitis, or idiopathic; classic triad: gait apraxia, dementia, urinary incontinence
- Craniosynostosis - premature fusion of sutures restricts brain growth (note: does NOT cause hydrocephalus per se, but can cause raised ICP)
3. Pathophysiology
CSF Dynamics
CSF is produced mainly by the choroid plexuses within the ventricles (approximately 0.35 mL/min, ~500 mL/day). It flows through the ventricular system - from lateral ventricles → third ventricle → aqueduct of Sylvius → fourth ventricle → exits via foramina of Magendie (median) and Luschka (lateral apertures) → into the subarachnoid space → circulates over cerebral convexities → absorbed at arachnoid granulations (Pacchionian bodies) into the superior sagittal sinus. Cerebrovascular pulsations also influence this net flow.
Mechanism of Ventricular Enlargement
When obstruction occurs, CSF accumulates proximal to the blockage. The key principle (Ayer's adage): the ventricle closest to the obstruction enlarges the most. For example:
- Aqueductal obstruction → disproportionate enlargement of lateral + third ventricles; fourth ventricle remains normal
- Fourth ventricle obstruction → dilatation includes the aqueduct
- Basal cisternal obstruction → entire ventricular system including fourth ventricle enlarges
Acute Phase
- Ventricular enlargement is rapid: 80% of maximal enlargement within 6 hours of acute noncommunicating obstruction
- Continued CSF production despite raised ICP
- Elevated intracranial pressure (ICP)
- Transependymal (periventricular interstitial) edema - CSF is forced across the ependymal lining into the periventricular white matter, visible on MRI as periventricular T2 signal
Chronic Phase
- After ventricular enlargement stabilizes, CSF production is balanced by transependymal absorption
- ICP may normalize - this is the basis of normal-pressure hydrocephalus
- Long-term monitoring reveals intermittent ICP spikes
- White matter atrophy surrounds the ventricles; gray matter is relatively spared
- Stretching of corticospinal tracts (which descend from motor cortex around the lateral ventricles) → lower limb spasticity
Infant vs. Older Child
- In infants (before suture fusion, typically before age 3): expanding ventricles separate cranial sutures → head enlargement is the primary manifestation; ICP elevation is buffered
- After sutures close: ventricles expand against a rigid skull → raised ICP is the dominant consequence; no head enlargement
4. Clinical Features in Infants (Before Suture Fusion, < 2 Years)
The key feature is progressive macrocephaly (head circumference crossing centile lines on growth charts), since the skull can expand to accommodate the increased CSF volume.
Head and Skull Signs
- Accelerated head growth - head circumference increasing faster than expected for age; the most reliable early sign
- Frontal bossing - prominent, disproportionately large forehead (brachycephalic skull)
- Tense, bulging anterior fontanelle - fontanelle does not pulsate normally; feels tense even when the infant is sitting upright
- Sutural diastasis - palpable widening of sutures, especially the sagittal suture
- Calvarial thinning - may be seen on imaging; "beaten copper" or "digital markings" on skull X-ray from gyral impressions
- Dilated scalp veins - venous collaterals from raised venous pressure
Eye Signs
- "Sunset" sign (Setting-sun sign): forced downward deviation of the eyes with sclera visible above the iris; caused by pressure on the dorsal midbrain (pretectal area) from the dilated third ventricle, producing a Parinaud-like syndrome
- Failure of upward gaze
- Lateral rectus palsy (CN VI palsy) - false localizing sign from raised ICP
Neurological Signs
- Irritability - common early symptom; infant is fretful
- Poor feeding, lethargy
- Spasticity of lower limbs - from stretching of the corticospinal tracts descending around the lateral ventricles
- Nausea and vomiting (in acute enlargement)
Late / Severe Signs (if untreated)
- Abnormal eye movements and optic atrophy (if diagnosis delayed)
- Developmental regression
- In severely advanced cases: loss of white matter, cortical atrophy
5. Clinical Features in Older Children (After Suture Fusion, > 3 Years)
Once the sutures close, the head cannot expand, so rising ICP becomes the primary problem. Features are those of raised intracranial pressure.
Symptoms
- Headache - classically worse in the morning (positional, from nocturnal ICP surges) and on waking, often frontal or global; may wake the child from sleep
- Nausea and vomiting - often projectile; worse in the morning
- Diplopia - due to CN VI (abducens) palsy; a false localizing sign from raised ICP; occurs on one or both sides
- Blurred vision - from papilloedema and/or impaired accommodation
- Altered level of consciousness - drowsiness, decreased responsiveness in severe cases
Signs
- Papilloedema - on fundoscopy; the hallmark of chronic raised ICP; may be absent in rapidly developing hydrocephalus
- CN VI palsy (lateral rectus palsy, convergent squint)
- Spasticity of lower limbs - broad-based, ataxic gait; from periventricular white matter stretching around the lateral ventricles
- Wide-based ataxic gait - from frontal lobe fiber tract distortion
- Endocrine dysfunction (in long-standing cases): short stature, precocious or delayed puberty, menstrual irregularities, diabetes insipidus - from hypothalamic/pituitary compression
- Cognitive changes and memory impairment - in chronic cases
- Cushing response (bradycardia, hypertension, irregular respiration) - in critically raised ICP
Specific Features by Cause
- Posterior fossa tumor-related hydrocephalus (medulloblastoma, ependymoma): acute onset, headache, vomiting, ataxia, and cranial nerve palsies, particularly CN VI; papilloedema; lower limb spasticity
- Aqueductal stenosis in older children: may present insidiously with slow cognitive decline, gait disturbance, and endocrine problems
6. Differential Diagnosis of Enlarged Head (Macrocephaly)
An enlarged head in an infant or child is not always due to hydrocephalus. The differential includes:
| Category | Causes |
|---|---|
| True hydrocephalus | All forms listed above (obstructive, communicating) |
| Constitutional / Familial Macrocrania | Autosomal dominant "benign familial macrocephaly"; head large but neurologically normal; often a parent also has a large head |
| Megalencephaly (enlarged brain substance) | - Anatomical megalencephaly: unilateral or bilateral overgrowth (often with hemimegalencephaly, causing seizures and hemiplegia) - Metabolic/storage megalencephaly: Krabbe disease, Alexander disease (leukodystrophy), Tay-Sachs disease, Canavan spongy degeneration of the brain |
| Subdural collections | - Subdural hematoma (traumatic or non-accidental injury) - Subdural hygroma (clear fluid, post-meningitic or spontaneous) - External hydrocephalus (enlarged subarachnoid spaces + mild ventricular enlargement) |
| Bone abnormalities | - Craniosynostosis with preferential unidirectional skull growth (can give a large head circumference without hydrocephalus - important caveat: always measure in all directions) - Rickets (frontal bossing from softened calvaria) - Osteopetrosis |
| Structural lesions | - Large arachnoid cysts (temporal, posterior fossa) - Neonatal ventricular hemorrhage with clot - Large porencephalic cysts |
| Hydranencephaly | Essentially absent cerebral hemispheres replaced by CSF; large fluid-filled skull, absent cortex; transillumination positive |
| Holoprosencephaly | Failure of forebrain division; single monoventricle |
Key caution: In craniosynostosis, premature suture fusion may cause an asymmetric skull or growth preferentially in one direction, giving a spuriously large head circumference - never diagnose hydrocephalus on circumference alone. Always correlate with imaging.
Summary: Key Distinguishing Features by Age
| Feature | Infant (< 2 yrs, open sutures) | Older Child (> 3 yrs, closed sutures) |
|---|---|---|
| Skull | Enlarging head circumference crossing centiles | Normal head size |
| Fontanelle | Tense, bulging, full | Fused - not assessable |
| Sutures | Diastasis | Fused |
| Eye signs | Sunset sign, upward gaze failure | Papilloedema, CN VI palsy |
| Dominant symptom | Head growth, irritability, poor feeding | Morning headache, vomiting |
| ICP | Buffered by skull expansion | Elevated, symptomatic |
| Most common cause | Post-hemorrhagic, post-infective, aqueductal stenosis, Chiari II | Posterior fossa tumors, aqueductal stenosis |
Sources:
- Adams and Victor's Principles of Neurology, 12th Ed. - "Syndromes of Hydrocephalus," p. 635
- Bradley and Daroff's Neurology in Clinical Practice - "Hydrocephalus in Children," p. 1854
- Grainger & Allison's Diagnostic Radiology - "HYDROCEPHALUS," p. 2028
- Robbins & Kumar Pathologic Basis of Disease - "Hydrocephalus," p. 1149
- The Developing Human: Clinically Oriented Embryology - "Hydrocephalus," p. 1082
This is a shared conversation. Sign in to Orris to start your own chat.