Paracetamol posioning
Reading File
Finding Sources
Finding Sources
Searching PubMed
"paracetamol" AND "poisoning" AND "acetylcysteine"
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from the textbooks. Let me compile the full answer.
Paracetamol (Acetaminophen) Poisoning
Pharmacokinetics
- Absorbed rapidly from the GI tract; peak plasma levels in 30-60 minutes
- Plasma half-life ~2 hours under therapeutic conditions
Mechanism of Toxicity
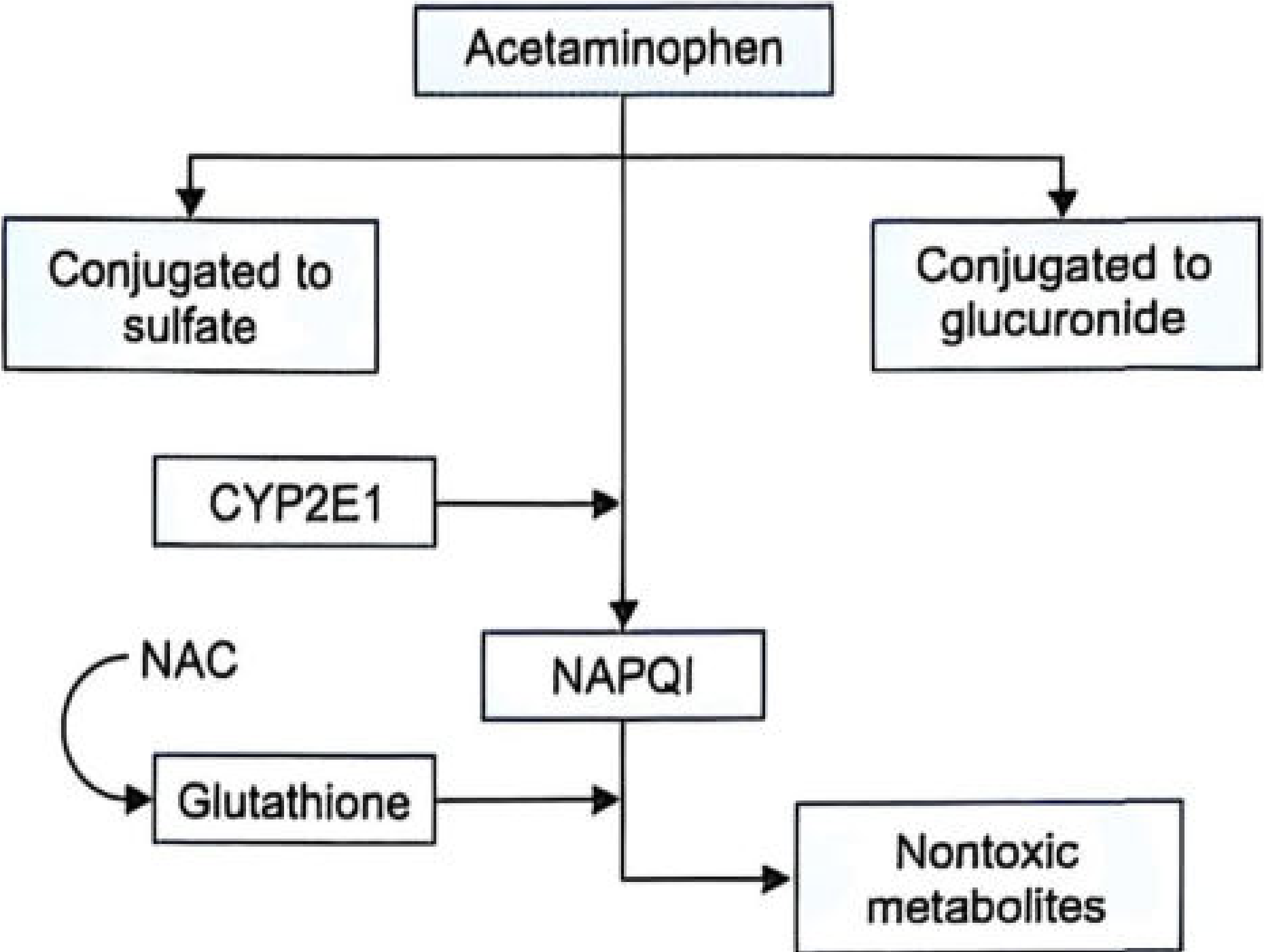
Under normal conditions, ~90% of paracetamol is conjugated with glucuronic acid and sulfuric acid to form nontoxic metabolites. The remaining ~10% is metabolized by CYP2E1 into NAPQI (N-acetyl-p-benzoquinone imine), a highly reactive toxic compound.
Normally, NAPQI is rapidly neutralized by glutathione and excreted safely. In overdose, hepatic glutathione reserves are exhausted, allowing NAPQI to accumulate. It binds covalently to liver cell proteins - particularly in the centrilobular region - causing oxidative stress and hepatocyte necrosis.
- The Essentials of Forensic Medicine and Toxicology, 36th Ed. (2026)
Fatal Dose
Ingestion of 20 tablets of 500 mg (i.e., 10 g) is usually fatal within 3-5 days.
Clinical Stages
| Stage | Timeframe | Clinical Features |
|---|---|---|
| Stage I | 0-24 hours | Nausea, vomiting, anorexia, malaise, pallor, diaphoresis. Often asymptomatic; LFTs usually normal. Patient may feel deceptively well. |
| Stage II | 24-72 hours | Right upper quadrant pain, rising AST/ALT and bilirubin, prolonged PT, possible early renal involvement |
| Stage III | 72-96 hours | Peak hepatotoxicity: jaundice, coagulopathy, hypoglycemia, hepatic encephalopathy, renal failure, metabolic acidosis, possible multi-organ failure |
| Stage IV | 4-14 days | Clinical improvement if survived; gradual normalization of LFTs; full recovery possible due to liver regeneration |
Key point: Stage I may create a false sense of security - a patient apparently well at 12 hours may still die of acute hepatic failure up to 5 days later.
Management
1. Decontamination
- Gastric lavage: Consider within 1 hour of ingestion (some sources say up to 4 hours)
- Activated charcoal: Give within 1-2 hours post-ingestion; note that it can reduce the effectiveness of oral NAC if co-administered
2. Antidotal Therapy - N-Acetylcysteine (NAC)
NAC is the antidote of choice - most effective when given within 8-10 hours of overdose. It acts as a glutathione precursor, replenishing stores to neutralize NAPQI.
Oral NAC:
- Loading dose: 140 mg/kg, then 70 mg/kg every 4 hours
- Duration: minimum 24 hours (6 doses) up to 72 hours (18 doses)
- Dilute to ~5% with water, soda, or juice
Intravenous NAC (preferred if vomiting):
- FDA-approved 3-bag protocol: 150 mg/kg over 1 hour (loading), then 50 mg/kg over 4 hours, then 100 mg/kg over 16 hours (total 21-hour regimen)
- A 2025 systematic review (PMID: 40013897) compared two-bag vs three-bag regimens and found the simplified two-bag protocol has fewer adverse drug reactions
Methionine (oral glutathione precursor):
- 2.5 g every 4 hours for up to 4 doses (some sources: 10 g over 12 hours in 4 doses)
- Useful when NAC is unavailable, especially in remote settings; effective if given within 10 hours
3. Supportive Care
- Complications (hypoglycemia, metabolic acidosis, coagulopathy): treat with dextrose, bicarbonate, Vitamin K1, fresh whole blood/plasma
- IV fluid caution: >2.5 L/day is risky due to paracetamol-induced fluid retention
- Hemodialysis: for severe overdose with very high serum levels, metabolic complications, or acute renal failure
4. Liver Transplantation
Indicated by (King's College Criteria):
- Severe metabolic acidosis
- Prothrombin time >100 seconds
- Serum creatinine >300 μmol/L
5. Rumack-Matthew Nomogram
Plots serum paracetamol concentration against time since ingestion to guide treatment decisions - determines whether NAC treatment is needed.
Postmortem Findings
- Centrilobular hepatic necrosis (characteristic)
- Acute tubular necrosis (kidneys)
- Myocardial damage
- Cerebral edema
Medico-legal Aspects
- Paracetamol overdose is frequently associated with intentional self-harm
- In fatal cases, organ donation may still be possible depending on clinical and legal criteria
Sources:
- The Essentials of Forensic Medicine and Toxicology, 36th Ed. (2026), pp. 542-543
- Parikh's Textbook of Medical Jurisprudence, Forensic Medicine and Toxicology, p. 714
- Two-bag vs three-bag NAC regimens - systematic review 2025 (PMID: 40013897)
King college criteria
Finding Sources
Finding Sources
Searching PubMed
"King's College criteria" AND "acute liver failure"
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have all the detail needed. Also noting from Sleisenger the Box 95.1 reference - let me also check the Sleisenger Box for the full criteria text seen briefly earlier.
The data from multiple surgical/GI textbooks is consistent and complete. Here is the comprehensive answer:
King's College Criteria (KCC) for Liver Transplantation in Acute Liver Failure
The King's College Hospital (KCH) criteria, originally published in 1989, are the most widely accepted prognostic tool for identifying patients with acute liver failure (ALF) unlikely to survive without liver transplantation. They have separate criteria for paracetamol (acetaminophen) and non-paracetamol causes.
A. Paracetamol (Acetaminophen)-Induced ALF
Meet either of the following:
Option 1 (Single criterion - high specificity):
Arterial pH < 7.3 - irrespective of encephalopathy grade
(Subsequent modification adds: arterial lactate > 3.0 mmol/L or serum lactate > 3.5 mmol/L after adequate fluid resuscitation)
Option 2 (Triple criterion - all three must be present):
| Parameter | Threshold |
|---|---|
| Prothrombin time | > 100 seconds (INR > 6.5) |
| Serum creatinine | > 3.4 mg/dL (> 300 μmol/L) |
| Hepatic encephalopathy | Grade III or IV |
B. Non-Paracetamol ALF
Meet either of the following:
Option 1 (Single criterion):
Prothrombin time > 100 seconds (INR > 6.5) - irrespective of encephalopathy grade
Option 2 (Any 3 of the following 5):
| Parameter | Threshold |
|---|---|
| Age | < 10 years or > 40 years |
| Etiology | Drug toxicity, cryptogenic hepatitis, or undetermined |
| Jaundice-to-encephalopathy interval | > 7 days |
| Prothrombin time | > 50 seconds (INR > 3.5) |
| Serum bilirubin | > 17-17.5 mg/dL (> 300 μmol/L) |
Performance Characteristics
| Paracetamol ALF | Non-Paracetamol ALF | |
|---|---|---|
| Specificity | ~95% | ~82-93% |
| Sensitivity | ~58% | ~58-85% |
| Positive predictive value | ~84% | ~98% |
| Negative predictive value | ~86% | ~82% |
Key point: KCC has high specificity but low sensitivity - if criteria ARE met, there is at least an 80% chance of death without transplant. However, failing to meet criteria does NOT exclude poor outcome (up to 50% still die).
Important Notes
- KCC does not replace clinical judgment - it is a decision aid, not a binary decision tool
- Alternative/Complementary tools include:
- MELD score (>30.5 predicts need for transplant; more sensitive but less specific than KCC)
- Clichy criteria (France): Factor V < 20% (age < 30) or < 30% (age ≥ 30) once grade II encephalopathy develops
- ALFSG Prognostic Index: Newer app-based tool (area under ROC = 0.843 vs KCC's 0.56-0.655), based on encephalopathy grade, etiology, vasopressor use, INR, and bilirubin
- Any patient meeting KCC should be urgently transferred to a liver transplant center
- KCC is NOT applied if there is irreversible brain damage (transplant is contraindicated)
- Paracetamol overdose patients meeting KCC are given highest transplant priority in the UNOS/organ allocation system
Sources: Mulholland and Greenfield's Surgery, 7th Ed. (Table 58.4); Schwartz's Principles of Surgery, 11th Ed. (Table 31-2); Sleisenger and Fordtran's Gastrointestinal and Liver Disease; Yamada's Textbook of Gastroenterology, 7th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.