Non neoplastic salivary gland diseases. Ms ent University exam pattern for 20 marks. No abbreviations, with relevant diagrams. As per standard ENT textbooks.
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
Loading Image
I now have comprehensive content from Cummings and Scott-Brown's. I have all the major sections covered. Let me now compile the complete 20-mark MS ENT university exam answer.
NON-NEOPLASTIC SALIVARY GLAND DISEASES
(MS ENT University Examination - 20 Marks)
INTRODUCTION
Non-neoplastic diseases of the salivary glands are a heterogeneous group of conditions that produce two cardinal presentations: salivary gland swelling and oral dryness (xerostomia). Understanding their classification, pathophysiology, clinical features, investigations, and management is essential for ENT surgical practice.
CLASSIFICATION
I. Inflammatory Diseases (Sialadenitis)
- A. Infectious
-
- Acute bacterial sialadenitis
-
- Viral sialadenitis (Mumps/Epidemic parotitis)
-
- Granulomatous (Tuberculosis, Actinomycosis, Cat-scratch disease)
-
- B. Non-infectious
-
- Chronic recurrent (obstructive) sialadenitis
-
- Chronic sclerosing sialadenitis (Kuttner tumour)
-
- Recurrent parotitis of childhood
-
- Autoimmune: Sjogren syndrome
-
- Sarcoidosis (Heerfordt syndrome)
-
- Radioiodine/radiation-induced sialadenitis
-
- IgG4-related sialadenitis
-
II. Obstructive Salivary Gland Disease
- Sialolithiasis (salivary calculi)
- Salivary duct strictures
III. Salivary Gland Hypofunction
- Xerostomia (drug-induced, post-radiation, Sjogren)
IV. Salivary Gland Cysts
- Mucoceles (extravasation and retention types)
- Ranula
V. Miscellaneous
- Sialosis (sialadenosis)
- Necrotizing sialometaplasia
- Frey syndrome (gustatory sweating)
I. SIALOLITHIASIS (SALIVARY CALCULI)
Definition
Sialolithiasis is the formation of calculi (sialoliths) within the ductal system of the salivary glands. It is the most common cause of salivary gland inflammation.
(Cummings Otolaryngology, 7th Ed.)
Incidence and Distribution
- Submandibular gland: 80-90% (most common) - due to Wharton's duct
- Parotid gland: 10-20% - within Stensen's duct
- Sublingual and minor glands: 1%
- Peak age: fifth to eighth decades; males more commonly affected than females
- Lifetime prevalence of symptomatic calculi: 0.45%
Composition
Salivary stones are composed predominantly of calcium phosphate and carbonate combined with an organic matrix of glycoproteins and mucopolysaccharides. Small amounts of magnesium, potassium, and ammonium are also present.
Why Submandibular Gland is Predominantly Affected
The following anatomical and physiological factors predispose the submandibular gland:
┌─────────────────────────────────────────────────────────┐
│ FACTORS FAVOURING SMG CALCULUS FORMATION │
├─────────────────────────────────────────────────────────┤
│ Wharton's duct: longer, wider, more tortuous │
│ Flow against gravity (courses round mylohyoid) │
│ Saliva: more alkaline, mucoid, viscous │
│ Higher calcium and phosphate concentration in saliva │
│ Slower flow rate → increased stasis │
└─────────────────────────────────────────────────────────┘
(Cummings Otolaryngology)
Pathogenesis
Intermittent salivary stasis causes alteration of the mucoid elements of saliva, leading to formation of an organic gel. This gel acts as a nidus for deposition of calcium salts, resulting in progressive calculus formation. Serum calcium and phosphate levels are not related to stone formation.
Clinical Features
- Recurrent postprandial pain and swelling of the affected gland (salivary colic)
- Swelling appears at mealtimes (gustatory stimulus) and slowly resolves over hours
- History of multiple episodes of acute suppurative sialadenitis
- On examination: bimanual palpation may reveal a palpable stone in the floor of mouth (Wharton's duct)
- Absence or diminished salivary flow from the duct orifice
- Long-standing cases may show signs of chronic sialadenitis
Radiology Notes
- 90% of submandibular stones are radio-opaque (high calcium content)
- 90% of parotid stones are radiolucent (lower calcium content)
- Up to 15% of all calculi are radiolucent on plain radiographs
Imaging of Sialolithiasis:
(a) Orthopantomogram (OPG) showing right submandibular gland hiloparenchymal calculus projected over the posterior mandible (red arrow):

(b) Coronal CT scan confirming submandibular calculus (red arrow):

(c) Digital subtraction sialography showing right submandibular duct with partially obstructing luminal calculus causing proximal ductal dilatation (red arrow):
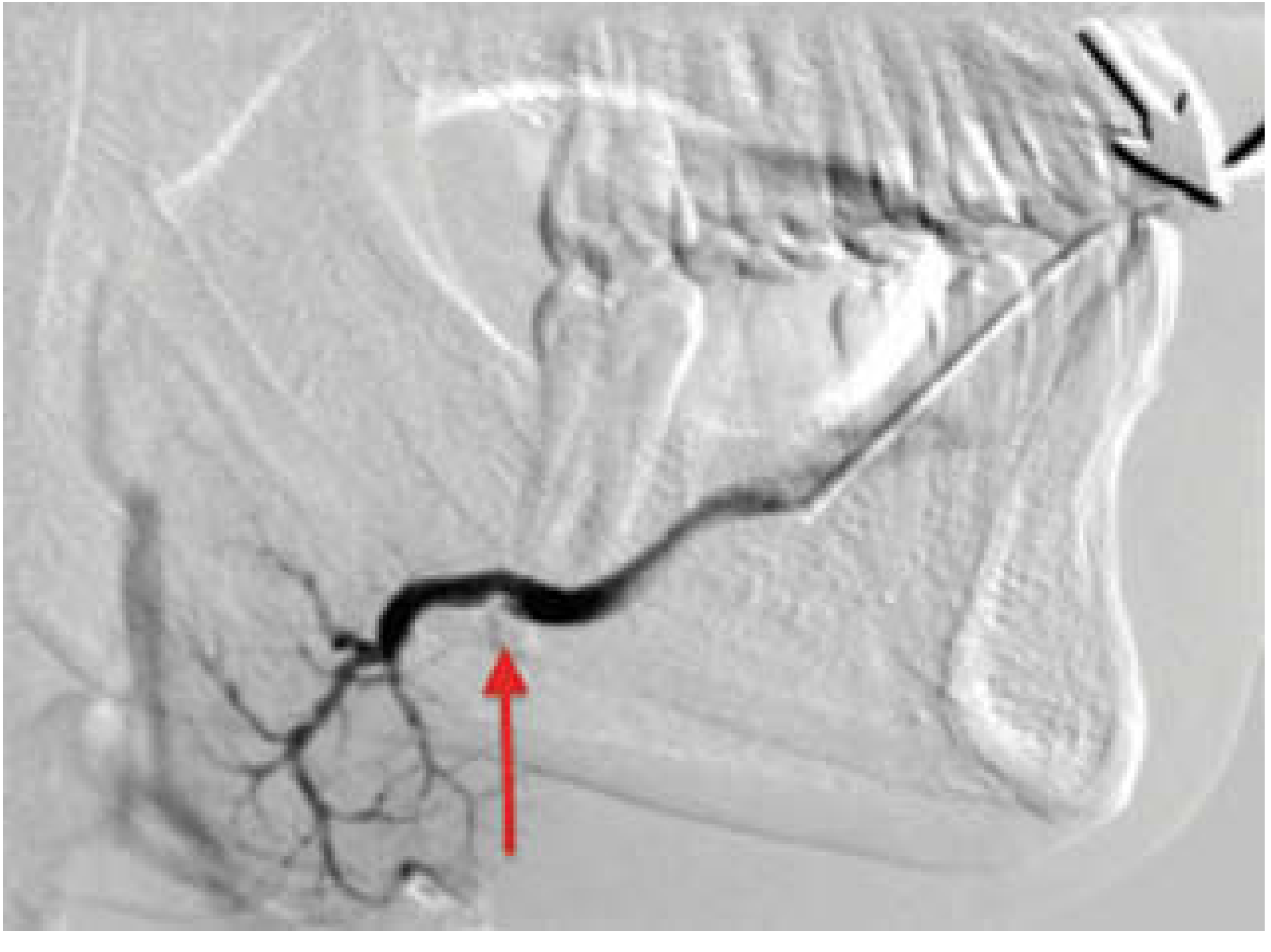
Scott-Brown's Otorhinolaryngology Head & Neck Surgery, 8th Ed.
Investigations
- Plain radiograph (Floor of mouth/Occipitomental view/OPG) - for radio-opaque stones
- Ultrasound - most commonly used; identifies stones >2 mm, shows gland echogenicity and ductal dilatation
- Computed Tomography - more sensitive; identifies all stone types including radiolucent
- Sialography - instillation of contrast into duct (4-15% failure rate, risk of provoking acute sialadenitis); demonstrates ductal anatomy, strictures, and filling defects
- Magnetic resonance sialography - non-invasive; relies on T2-weighted signal from inherent salivary fluid; no cannulation or contrast needed
Management
┌──────────────────────────────────────────────────────────────┐
│ MANAGEMENT OF SIALOLITHIASIS │
├──────────────────────────────────────────────────────────────┤
│ CONSERVATIVE (all cases initially) │
│ • Adequate hydration, sour candy/lemon to stimulate flow │
│ • Massage the gland from posterior to anterior │
│ • Warm compresses │
│ • Analgesics, anti-inflammatory agents │
│ • Antibiotics if acute sialadenitis present │
├──────────────────────────────────────────────────────────────┤
│ MINIMALLY INVASIVE / INTERVENTIONAL │
│ • Surgical milking/manual extraction (distal duct stones) │
│ • Sialoendoscopy (diagnostic and therapeutic) │
│ • Extracorporeal shock wave lithotripsy (ESWL) │
│ • Interventional sialography (basket retrieval) │
├──────────────────────────────────────────────────────────────┤
│ SURGICAL (failed conservative, large/multiple stones) │
│ • Intraoral incision over duct for anterior floor-of-mouth │
│ stones (submandibular duct stone) │
│ • Submandibulectomy - for recurrent/intraglandular stones │
│ • Parotidectomy - rare, for intraglandular parotid stones │
└──────────────────────────────────────────────────────────────┘
(Cummings Otolaryngology)
II. ACUTE BACTERIAL SIALADENITIS
Pathogenesis
Acute bacterial sialadenitis occurs predominantly in the parotid gland. The main mechanism is retrograde bacterial migration from the oral cavity due to salivary stasis. This is facilitated by:
- Dehydration (post-operative, elderly, bedridden patients)
- Malnutrition
- Poor oral hygiene
- Medications causing xerostomia (anticholinergics, diuretics, antidepressants)
- Ductal obstruction from a sialolith
┌────────────────────────────────────────────────────────┐
│ PATHOGENESIS OF ACUTE BACTERIAL │
│ PAROTID SIALADENITIS │
│ │
│ Dehydration / Salivary stasis │
│ ↓ │
│ Reduced salivary flow & antimicrobial activity │
│ ↓ │
│ Retrograde ascent of oral bacteria via Stensen duct │
│ ↓ │
│ Acute suppurative parotitis │
│ ↓ │
│ If untreated → Abscess formation │
└────────────────────────────────────────────────────────┘
Common Organisms
- Staphylococcus aureus - most common (including methicillin-resistant strains)
- Streptococcus viridans
- Haemophilus influenzae
- Anaerobes (Bacteroides, Peptostreptococcus) - in mixed infections
Clinical Features
- Sudden onset tender, firm swelling of the parotid gland
- Trismus may be present (indicating parapharyngeal extension)
- Erythema and oedema of overlying skin
- Pus expressible from Stensen's duct orifice
- Systemic features: fever, malaise, raised white cell count
- Medial tonsillar displacement or trismus suggests deeper parapharyngeal space involvement
Investigations
- Full blood count, blood cultures
- Pus culture and sensitivity from duct orifice
- Ultrasound - confirms parotid involvement, identifies abscess, excludes obstructing calculus
- Computed tomography - for deep space involvement (parapharyngeal abscess)
Management
- Intravenous antibiotics (anti-staphylococcal: flucloxacillin or co-amoxiclav) - adjusted according to culture sensitivities
- Adequate hydration (intravenous fluid replacement)
- Oral hygiene measures
- Gland massage
- Sialogogues
- Surgical drainage for abscess formation (incision with facial nerve preservation)
III. VIRAL SIALADENITIS - MUMPS (EPIDEMIC PAROTITIS)
Epidemiology
Mumps is caused by Paramyxovirus (RNA virus). It is primarily a disease of childhood (5-15 years), transmitted via respiratory droplets. The incubation period is 14-21 days. It is now rare in vaccinated populations (Measles-Mumps-Rubella vaccine).
Clinical Features
- Prodrome: fever, malaise, anorexia, headache (1-2 days)
- Parotid swelling: painful, bilateral in 75% of cases (may start unilateral, become bilateral within 1-5 days)
- The swelling lifts the ear lobe outwards (pathognomonic appearance)
- Erythema around Stensen's duct orifice
- Trismus may be present
- Clear saliva (not purulent) - differentiates from bacterial sialadenitis
Complications
┌──────────────────────────────────────────────────────────┐
│ COMPLICATIONS OF MUMPS │
├──────────────────────────────────────────────────────────┤
│ Orchitis (most common in post-pubertal males - 25%) │
│ → may cause infertility │
│ Oophoritis (in post-pubertal females - 5%) │
│ Meningoencephalitis (most common complication overall) │
│ Pancreatitis │
│ Deafness (sensorineural - unilateral, permanent) │
│ Myocarditis │
│ Arthritis │
└──────────────────────────────────────────────────────────┘
Diagnosis
- Raised serum amylase (salivary isoenzyme)
- Complement fixation tests (S and V antibodies)
- Mumps IgM antibody (ELISA)
- Virus isolation from saliva, urine, cerebrospinal fluid
Management
- Supportive: analgesics, adequate hydration, soft diet
- No specific antiviral treatment
- Prevention: MMR vaccination (two-dose schedule)
IV. CHRONIC SIALADENITIS
Chronic Recurrent (Obstructive) Sialadenitis
Repeated episodes of acute sialadenitis from ductal obstruction lead to progressive parenchymal damage and ductal ectasia (sialectasia). The gland becomes progressively atrophied and fibrotic.
On sialography: the ductal system shows sausage-link dilatation (sialectasia) with progressive loss of normal arborization.
On ultrasound: the gland appears bulky, hyperaemic early; later becomes echo-reflective and atrophied.
Management:
- Treat acute episodes with antibiotics
- Salivary duct dilation or sialoendoscopy
- Gland excision (submandibulectomy or parotidectomy) for recurrent/refractory cases
Chronic Sclerosing Sialadenitis (Kuttner Tumour)
A chronic inflammatory condition almost exclusively affecting the submandibular gland, producing a firm tumour-like mass that mimics malignancy. It is histopathologically characterized by dense lymphoplasmacytic infiltrate, fibrosis, and acinar atrophy. It is now recognized as a manifestation of IgG4-related disease.
Clinical features: Hard, painless submandibular swelling; may be bilateral; often mistaken clinically and on imaging for a neoplasm.
Management: Submandibulectomy (often required for diagnosis and treatment). Systemic corticosteroids may be effective in IgG4-related cases.
V. SJOGREN SYNDROME
Definition
Sjogren syndrome is a chronic systemic autoimmune disorder of the exocrine glands characterized by a lymphoplasmacytic infiltration with resulting glandular hypofunction, leading to xerostomia (dry mouth) and keratoconjunctivitis sicca (dry eyes).
(Cummings Otolaryngology, 7th Ed.)
Epidemiology
- Estimated prevalence: 1-3% of the population
- Peak onset: fourth to fifth decade of life
- More than 90% of patients are women (strong female preponderance)
- Second most common autoimmune rheumatic disease after rheumatoid arthritis
Classification
┌──────────────────────────────────────────────────────────────┐
│ CLASSIFICATION OF SJOGREN SYNDROME │
├─────────────────────┬────────────────────────────────────────┤
│ PRIMARY │ SECONDARY │
│ (isolated) │ (associated with another │
│ │ autoimmune disease) │
│ Exocrine gland │ Rheumatoid arthritis │
│ involvement only │ Systemic lupus erythematosus │
│ (sicca complex) │ Systemic sclerosis (scleroderma) │
│ │ Primary biliary cirrhosis │
│ │ Polymyositis │
└─────────────────────┴────────────────────────────────────────┘
Pathogenesis
┌────────────────────────────────────────────────────────────┐
│ PATHOGENESIS OF SJOGREN SYNDROME │
│ │
│ Genetic predisposition (HLA-B8, HLA-DR3 alleles) │
│ ↓ │
│ Environmental trigger (likely viral - Epstein-Barr │
│ virus, Coxsackie, Hepatitis C) │
│ ↓ │
│ Aberrant autoimmune activation │
│ ↓ │
│ B-cell overstimulation → excess immunoglobulins + │
│ autoantibodies (anti-Ro/SS-A, anti-La/SS-B) │
│ ↓ │
│ Dense lymphocytic (CD4+ T-cell) infiltration of │
│ exocrine glands │
│ ↓ │
│ Formation of germinal centres → autoreactive B-cell │
│ clones escape tolerance checkpoints │
│ ↓ │
│ Progressive acinar destruction + ductal obstruction │
│ ↓ │
│ Salivary and lacrimal hypofunction │
└────────────────────────────────────────────────────────────┘
Clinical Features
Oral manifestations (Xerostomia):
- Difficulty chewing, swallowing, and phonation
- Adherence of food to the buccal mucosa
- Intolerance to acidic and spicy foods
- Multiple dental caries (rampant caries)
- Smooth, fissured tongue with atrophy of filiform papillae
- Absence of pooled saliva in the floor of mouth
- Oral candidiasis (Candida albicans overgrowth)
- Scant/cloudy saliva expressible from ducts
Ocular manifestations:
- Foreign body sensation ("gritty" or "sandy" eyes)
- Keratoconjunctivitis sicca
Salivary gland enlargement:
- Bilateral parotid enlargement in 25-66% of patients (recurrent, episodic or chronic, fixed)
- Submandibular gland may also be enlarged
Systemic manifestations:
- Arthralgia/arthritis
- Vasculitis
- Peripheral neuropathy
- Renal tubular acidosis
- Thyroid disease
- Lymphoma (5-fold increased risk) - a serious complication; secondary mucosa-associated lymphoid tissue (MALT) lymphoma
Diagnostic Criteria (American-European Consensus Group 2002 - as referenced in standard texts)
┌────────────────────────────────────────────────────────────────┐
│ DIAGNOSTIC CRITERIA FOR SJOGREN SYNDROME │
├────────────────────────────────────────────────────────────────┤
│ 1. Ocular symptoms (dry eye, foreign body sensation) │
│ 2. Oral symptoms (dry mouth, recurrent salivary swelling) │
│ 3. Objective ocular signs: Schirmer test ≤5 mm/5 min OR │
│ Rose Bengal staining score ≥4 │
│ 4. Salivary gland histopathology: focal lymphocytic │
│ sialadenitis (focus score ≥1 per 4 mm²) │
│ 5. Objective evidence of salivary gland involvement: │
│ - Unstimulated whole saliva flow ≤1.5 mL/15 min, OR │
│ - Parotid sialography showing punctate/globular/ │
│ cavitary pattern, OR │
│ - Salivary scintigraphy showing delayed uptake/ │
│ reduced concentration │
│ 6. Serology: anti-Ro (SS-A) or anti-La (SS-B) antibodies │
│ │
│ Primary SS: ≥4 criteria; criteria 4 or 6 must be positive │
│ Secondary SS: criteria 1 or 2 PLUS any 2 of criteria 3-5 │
└────────────────────────────────────────────────────────────────┘
Investigations
- Serology: Raised erythrocyte sedimentation rate, raised immunoglobulins, anti-nuclear antibodies (ANA), anti-Ro (SS-A), anti-La (SS-B) antibodies, rheumatoid factor
- Schirmer test: Filter paper placed under lower eyelid; <5 mm wetting in 5 minutes indicates reduced lacrimal secretion
- Slit-lamp examination: Rose Bengal staining for keratoconjunctivitis sicca
- Salivary flow rate measurement (Lashley cup cannula)
- Lip biopsy (minor salivary gland biopsy): Gold standard histological test - shows focal lymphocytic sialadenitis with focus score >1
- Parotid sialography/scintigraphy
- Ultrasound of salivary glands
Histopathology
Minor salivary gland biopsy shows:
- Focal lymphocytic sialadenitis
- Foci (aggregates) of >50 lymphocytes per 4 mm² (focus score)
- Acinar atrophy and replacement by lymphocytes
- Ductal changes with epimyoepithelial islands
Management
┌──────────────────────────────────────────────────────────────┐
│ MANAGEMENT OF SJOGREN SYNDROME │
├──────────────────────────────────────────────────────────────┤
│ LOCAL (symptomatic) │
│ • Artificial saliva substitutes / frequent water sips │
│ • Sugar-free chewing gum (increases salivary flow) │
│ • Fluoride applications (prevent dental caries) │
│ • Artificial tears (eye lubricants) for dry eyes │
│ • Antifungals (nystatin/fluconazole) for oral candidiasis │
├──────────────────────────────────────────────────────────────┤
│ SYSTEMIC (sialagogues) │
│ • Pilocarpine (muscarinic M1/M3 agonist) 5 mg four times │
│ daily - licensed for Sjogren syndrome │
│ • Cevimeline 30 mg three times daily │
│ • Side effects: sweating, flushing, urinary frequency │
├──────────────────────────────────────────────────────────────┤
│ IMMUNOMODULATORY (systemic disease) │
│ • Hydroxychloroquine │
│ • Methotrexate │
│ • Biologics: rituximab (anti-CD20) for systemic disease │
│ • Corticosteroids (for acute exacerbations) │
└──────────────────────────────────────────────────────────────┘
VI. RECURRENT PAROTITIS OF CHILDHOOD
Definition
Recurrent parotitis of childhood is a distinct entity characterized by recurrent, non-obstructive, non-suppurative inflammation of the parotid gland, occurring between 3 and 6 years of age, with spontaneous resolution at puberty.
Aetiology
Multifactorial and often unilateral. Theories include congenital duct abnormalities, immune deficiency, and ascending infection. Sialectasia (punctate sialectasis) follows repeated infections.
Clinical Features
- Recurrent episodes of unilateral (less commonly bilateral) parotid swelling
- Each episode lasts 3-7 days, resolving spontaneously
- Mild fever and malaise
- Serous (not purulent) saliva from Stensen's duct
- Attacks decrease in frequency and severity as puberty approaches
Diagnosis
- Sialography: punctate sialectasis ("cherry blossom" or "fruit-laden tree" appearance)
- Ultrasound: multiple hypoechoic foci within parotid parenchyma
Management
- Antibiotics during acute episodes
- Analgesics, hydration, massage
- Sialoendoscopy and therapeutic interventional sialography (early intervention may avoid glandular destruction)
- Reassurance: the condition typically resolves at puberty
- Parotidectomy is rarely required
VII. SIALOSIS (SIALADENOSIS)
Definition
Sialosis is a chronic, non-inflammatory, non-neoplastic, bilateral enlargement of the parotid glands (rarely other glands), associated with systemic conditions.
Causes
┌──────────────────────────────────────────────────────┐
│ CAUSES OF SIALOSIS │
├──────────────────────────────────────────────────────┤
│ Nutritional/Metabolic: │
│ • Chronic alcoholism (most common) │
│ • Malnutrition, kwashiorkor, anorexia nervosa │
│ • Obesity │
│ • Vitamin deficiency │
├──────────────────────────────────────────────────────┤
│ Endocrine: │
│ • Diabetes mellitus │
│ • Hypothyroidism, acromegaly │
│ • Ovarian and pituitary disorders │
├──────────────────────────────────────────────────────┤
│ Drug-induced: │
│ • Antihypertensives (guanethidine) │
│ • Antipsychotics (phenothiazines) │
│ • Iodine-containing drugs │
└──────────────────────────────────────────────────────┘
Pathology
Acinar hypertrophy due to abnormal accumulation of secretory granules and lipid vacuoles. No inflammation, no fibrosis.
Management
- Treatment of underlying systemic cause
- Surgical parotidectomy is reserved for cosmetically unacceptable bilateral enlargement
VIII. GRANULOMATOUS SIALADENITIS
Sarcoidosis (Heerfordt Syndrome)
Sarcoidosis can involve the salivary glands, most commonly the parotid gland. The triad of Heerfordt syndrome consists of:
- Bilateral parotid enlargement (parotitis)
- Anterior uveitis
- Facial nerve palsy
- Low-grade fever
Histopathology shows non-caseating granulomas. Management: corticosteroids.
Tuberculosis
- Rare; presents as a firm parotid or submandibular mass
- May mimic malignancy
- Caseating granulomas on histopathology; Acid-fast bacilli on Ziehl-Neelsen stain
- Management: standard anti-tuberculosis therapy
IX. MUCOCELES AND RANULA
Mucoceles
Mucoceles are the most common disorder of the minor salivary glands.
Types:
- Extravasation mucocele (most common): Duct rupture causes pooling of mucus in adjacent connective tissue. Not lined by epithelium.
- Retention mucocele (less common): Partial or complete ductal obstruction causes retention of secretions and ductal dilatation. True cyst lined by epithelium.
Clinical features:
- Single, recurrent, fluctuant, painless, bluish swelling
- Lower lip is the most common site (lateral aspect)
- Other sites: floor of mouth, ventral surface of tongue
- Peak age: 10-29 years
- Ruptures easily releasing viscid saliva
Management:
- Surgical excision with the associated minor gland
- Marsupialization for recurrence
- Cryotherapy/laser ablation in selected cases
Ranula
A ranula is a mucocele involving the sublingual gland (occasionally minor salivary glands of the floor of mouth). The name is derived from its appearance resembling the underbelly of a frog ("rana").
Types:
┌────────────────────────────────────────────────────────┐
│ TYPES OF RANULA │
├──────────────────────┬─────────────────────────────────┤
│ SIMPLE (oral) │ PLUNGING (diving/cervical) │
├──────────────────────┼─────────────────────────────────┤
│ Confined to floor │ Herniates through or around │
│ of mouth │ mylohyoid muscle into neck │
│ Bluish translucent │ Presents as neck swelling │
│ swelling │ (no floor-of-mouth swelling │
│ │ may be present) │
└──────────────────────┴─────────────────────────────────┘
Management:
- Marsupialization (for simple ranula) - wide excision of the roof with sublingual gland removal
- Sublingual gland excision (definitive; reduces recurrence)
- For plunging ranula: sublingual gland excision ± cervical approach
X. XEROSTOMIA (DRY MOUTH)
Definition
Xerostomia is the subjective sensation of dry mouth due to reduced or absent salivary secretion (salivary hypofunction).
Causes
- Drug-induced (most common): Anticholinergics, antidepressants (tricyclics), antihypertensives, antihistamines, diuretics, antipsychotics
- Sjogren syndrome
- Radiation therapy to head and neck (dose-dependent; permanent if >26 Gray to parotid tissue)
- Systemic diseases: Sarcoidosis, amyloidosis, human immunodeficiency virus (diffuse infiltrative lymphocytosis syndrome), graft-versus-host disease
- Dehydration, anxiety
Consequences
- Rampant dental caries
- Oral candidiasis
- Difficulty with mastication, deglutition, and speech
- Mucositis, oral ulcers
- Dysgeusia (altered taste)
Management
- Identify and treat/modify the causative drug or condition
- Artificial saliva substitutes (carboxymethylcellulose-based sprays)
- Frequent sips of water, ice chips
- Sugar-free chewing gum (stimulates residual flow)
- Pilocarpine or cevimeline (sialagogues) for Sjogren syndrome
- Meticulous oral hygiene and fluoride applications
- Acupuncture (some evidence for radiation-induced xerostomia)
XI. FREY SYNDROME (AURICULOTEMPORAL NERVE SYNDROME / GUSTATORY SWEATING)
Definition
Frey syndrome is characterized by facial warmth, flushing, and sweating over the distribution of the auriculotemporal nerve in response to a gustatory stimulus (eating).
Pathogenesis (Aberrant Nerve Regeneration)
┌──────────────────────────────────────────────────────────────┐
│ PATHOGENESIS OF FREY SYNDROME │
│ │
│ Parotidectomy/parotid surgery/trauma │
│ ↓ │
│ Division of parasympathetic secretomotor fibres of │
│ auriculotemporal nerve to parotid gland │
│ ↓ │
│ Aberrant regeneration of these fibres │
│ ↓ │
│ Parasympathetic fibres reinnervate sweat glands and │
│ blood vessels of the overlying skin (instead of gland) │
│ ↓ │
│ Gustatory stimulus → sweating and flushing of skin │
│ (in distribution of auriculotemporal nerve) │
└──────────────────────────────────────────────────────────────┘
Clinical Features
- Onset: months to years after parotid surgery
- Sweating and flushing over the cheek during eating
- Minor's starch-iodine test (sweating area turns blue-black) is the gold standard for diagnosis
Management
- Minor topical treatments (antiperspirants)
- Botulinum toxin A injection (current most effective treatment) - subcutaneous infiltration; benefit lasts approximately 1.5 years in 60% of patients
- Surgical: sternocleidomastoid muscle flap interposition (limited benefit)
SALIVARY GLAND INVESTIGATIONS - SUMMARY TABLE
| Investigation | Indications | Key Finding |
|---|---|---|
| Plain radiograph (OPG, floor of mouth) | Sialolithiasis (radio-opaque) | Calculus |
| Ultrasound | First-line investigation; stone, abscess, gland assessment | Stone with acoustic shadow; gland echogenicity |
| Computed Tomography | Complex/deep stones; parapharyngeal involvement | All stone types; deep extension |
| Sialography | Ductal anatomy, strictures, sialectasis | Filling defect (stone), punctate sialectasis (parotitis/Sjogren) |
| Magnetic Resonance Imaging/sialography | Soft tissue, non-contrast stone, deep extension | T2 signal from duct fluid |
| Salivary scintigraphy | Sjogren syndrome, gland function assessment | Delayed/reduced uptake |
| Fine-needle aspiration biopsy | Salivary mass lesion (neoplastic vs non-neoplastic distinction) | Cytology |
| Lip (minor salivary gland) biopsy | Sjogren syndrome | Focal lymphocytic sialadenitis (focus score) |
| Serology (ANA, anti-Ro, anti-La) | Sjogren syndrome, autoimmune disease | Positive auto-antibodies |
| Schirmer test | Sjogren syndrome (lacrimal function) | <5 mm wetting in 5 minutes |
| Sialoendoscopy | Therapeutic and diagnostic for ductal disease | Direct visualization of duct, stone retrieval |
CONCLUDING SUMMARY
Non-neoplastic salivary gland diseases span a wide spectrum from simple obstructive calculous disease to complex autoimmune conditions. The key principles for examination:
- Sialolithiasis - submandibular gland most common (80-90%); postprandial pain and swelling; management is now gland-conservative (sialoendoscopy, lithotripsy) before surgical gland removal.
- Acute bacterial sialadenitis - parotid, retrograde bacterial migration; Staphylococcus aureus; treat with hydration and appropriate antibiotics.
- Mumps - paramyxovirus; bilateral parotitis; complications include orchitis and deafness.
- Sjogren syndrome - chronic autoimmune exocrinopathy; anti-Ro/SS-A and anti-La/SS-B antibodies; minor salivary gland biopsy is gold standard; increased lymphoma risk.
- Sialosis - bilateral painless parotid enlargement; associated with alcoholism, diabetes, malnutrition.
- Ranula - sublingual gland mucocele; simple vs. plunging types; treated by sublingual gland excision.
- Frey syndrome - post-parotidectomy gustatory sweating; managed with botulinum toxin.
Sources: Cummings Otolaryngology Head and Neck Surgery, 7th Ed. | Scott-Brown's Otorhinolaryngology Head & Neck Surgery, 8th Ed. | K.J. Lee's Essential Otolaryngology, 11th Ed. | Bailey and Love's Short Practice of Surgery, 28th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.