Ecg
Asking for Preferences
Reading File
Finding Sources
Searching Images
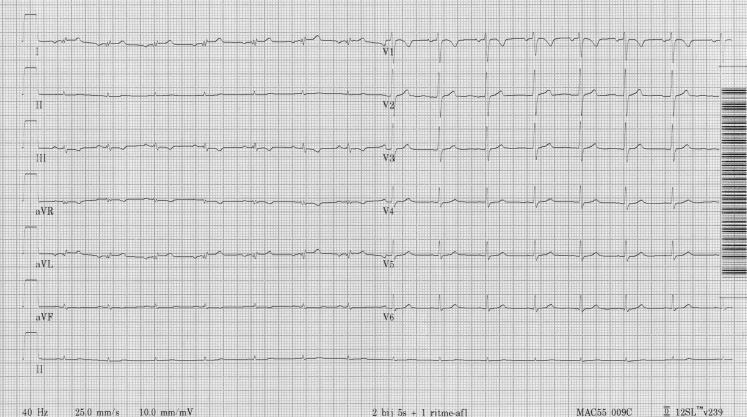
ECG electrocardiogram waves P QRS T interpretation
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Now I have comprehensive information from the textbooks. Let me compile a complete, well-structured ECG basics guide.
ECG Basics & Interpretation
What is an ECG?
The electrocardiogram (ECG/EKG) is a measurement of tiny potential differences on the body surface that reflect the electrical activity of the heart. These voltages are detectable because the atria and ventricles depolarize and repolarize in a specific sequence, creating potential differences between cardiac regions that surface electrodes can detect.
— Costanzo Physiology 7th Edition; Goldman-Cecil Medicine
The ECG Paper

Standard calibration (25 mm/sec, 10 mm/mV):
- Small box (1 mm) = 0.04 sec (40 ms) horizontally; 0.1 mV vertically
- Large box (5 mm) = 0.2 sec (200 ms) horizontally; 0.5 mV vertically
- A standard ECG runs for 10 seconds, with 12 leads recorded simultaneously
The Waveforms

| Wave / Interval | What it represents |
|---|---|
| P wave | Atrial depolarization |
| PR interval | Atrial depolarization + AV node + His-Purkinje conduction delay |
| PR segment | AV node conduction (isoelectric) |
| QRS complex | Ventricular depolarization |
| ST segment | Early ventricular repolarization (normally isoelectric) |
| T wave | Ventricular repolarization |
| QT interval | Total ventricular activity (depolarization + repolarization) |
| U wave | Rarely visible; possibly Purkinje repolarization or M-cell activity |
| J point | Junction between end of QRS and start of ST segment |
Note: Atrial repolarization is not visible — it is buried under the QRS complex because ventricular mass far exceeds atrial mass.
Normal Intervals
| Parameter | Normal Range |
|---|---|
| Heart rate | 50–100 bpm |
| P wave duration | < 120 ms (< 3 small boxes) |
| PR interval | 90–200 ms (2.5–5 small boxes) |
| QRS duration | 75–110 ms (< 3 small boxes) |
| QTc (males) | 390–450 ms |
| QTc (females) | 390–460 ms |
| QRS axis | −30° to +90° |
— Goldman-Cecil Medicine, Table 42-1
Heart Rate Calculation
Regular rhythm:
- HR = 300 ÷ number of large boxes between R waves
- Quick method: 300 → 150 → 100 → 75 → 60 → 50 (for 1 to 5 large boxes)
Irregular rhythm (e.g. AF):
- Count beats in 10-second strip × 6
The 12 Leads
Limb Leads (Frontal Plane)
- Lead I: Right arm (−) vs. Left arm (+)
- Lead II: Right arm (−) vs. Left leg (+)
- Lead III: Left arm (−) vs. Left leg (+)
- aVR, aVL, aVF: Augmented unipolar leads
In normal sinus rhythm, P waves and QRS complexes are positive in I, II, III, aVF and negative in aVR because depolarization moves from right to left and craniocaudally.
Precordial Leads (Transverse Plane)
Electrodes V1–V6 are positioned across the chest wall.
- V1 (right of sternum): Dominant S wave (activation moving away)
- V6 (mid-axillary): Dominant R wave (activation moving toward it)
- Normal R-wave progression: R wave grows from V1 → V6 (transition at V3–V4)
Systematic Interpretation Approach
A reliable stepwise method:
- Rate — Is it normal (60–100), bradycardic (<60), or tachycardic (>100)?
- Rhythm — Is it regular or irregular? Is there a P wave before every QRS?
- Axis — Normal (−30° to +90°)? Left axis deviation (<−30°)? Right axis deviation (>+90°)?
- P wave — Present? Upright in I and II (confirms sinus)? Duration < 120 ms?
- PR interval — 90–200 ms? Prolonged = 1st-degree AV block. Short = pre-excitation?
- QRS complex — Duration < 110 ms? Pathological Q waves? R-wave progression?
- ST segment — Isoelectric? Elevation = injury/STEMI? Depression = ischemia/NSTEMI?
- T wave — Concordant with QRS? Inversion = ischemia, strain? Peaked = hyperkalemia?
- QT interval — Calculate QTc. Prolonged > 450 ms (♂) / 460 ms (♀)?
Key Abnormality Patterns (Quick Reference)
| Finding | Possible Cause |
|---|---|
| Wide QRS (>110 ms) | Bundle branch block, hyperkalemia, pre-excitation |
| PR > 200 ms | 1st-degree AV block |
| ST elevation | STEMI, pericarditis, Brugada, early repolarization |
| ST depression | NSTEMI/ischemia, digitalis effect, LVH strain |
| Peaked symmetrical T waves | Hyperkalemia |
| T-wave inversion | Ischemia, PE, LVH strain, Takotsubo |
| Absent P waves + irregular R-R | Atrial fibrillation |
| QTc prolongation | Drugs (e.g. antiarrhythmics, antibiotics), electrolyte disturbance |
| J wave (Osborn wave) | Hypothermia, hypercalcemia |
Sources: Goldman-Cecil Medicine International Edition (Ch. 42); Costanzo Physiology 7th Ed.; Braunwald's Heart Disease
Hindi explain
ECG – हिंदी में समझें (Basics & Interpretation)
ECG क्या है?
ECG (Electrocardiogram) एक ऐसी जांच है जो दिल की बिजली की गतिविधि (electrical activity) को शरीर की सतह पर लगे इलेक्ट्रोड्स से रिकॉर्ड करती है।
दिल की मांसपेशियां जब सिकुड़ती और फैलती हैं, तो बिजली के संकेत (signals) निकलते हैं — ECG इन्हीं को कागज पर लहरों (waves) के रूप में दिखाता है।
ECG Paper कैसे पढ़ें?
| Box | समय (Time) | वोल्टेज |
|---|---|---|
| छोटा खाना (1 mm) | 0.04 sec | 0.1 mV |
| बड़ा खाना (5 mm) | 0.2 sec | 0.5 mV |
- क्षैतिज (Horizontal) → समय (Time)
- ऊर्ध्वाधर (Vertical) → वोल्टेज (Voltage / ऊंचाई)
- एक standard ECG = 10 सेकंड की रिकॉर्डिंग
ECG की लहरें (Waves) — क्या दर्शाती हैं?
🔵 P Wave
- आलिंद (Atria) का depolarization यानी ऊपरी चैंबर का सिकुड़ना
- छोटी, गोल लहर
- सामान्य अवधि: < 120 ms (3 छोटे खाने)
🟣 PR Interval
- P wave की शुरुआत से QRS की शुरुआत तक
- इसमें AV node की देरी शामिल होती है
- सामान्य: 120–200 ms
- बढ़ा हुआ PR → 1st Degree AV Block
🔴 QRS Complex
- निलय (Ventricles) का depolarization — नीचे के चैंबर का सिकुड़ना
- तीन लहरें: Q (नीचे), R (ऊपर), S (नीचे)
- सामान्य अवधि: 75–110 ms
- चौड़ा QRS (>110 ms) → Bundle Branch Block या Hyperkalemia
🟡 ST Segment
- QRS के बाद, T wave से पहले की सपाट रेखा
- सामान्यतः isoelectric (सपाट)
- ऊपर उठा (Elevation) → दिल का दौरा (STEMI) / Pericarditis
- नीचे दबा (Depression) → Ischemia / NSTEMI
🟢 T Wave
- निलय का repolarization (दिल का फिर से तैयार होना)
- सामान्यतः QRS की दिशा में उठी हुई
- उल्टी T (Inversion) → Ischemia, PE, Strain
- नुकीली T (Peaked) → Hyperkalemia (पोटेशियम ज़्यादा)
⚪ QT Interval
- QRS शुरू से T wave खत्म तक
- पूरे ventricular activity का समय
- QTc सामान्य: पुरुष < 450 ms, महिला < 460 ms
- लंबा QTc → अचानक cardiac arrest का खतरा
Heart Rate कैसे निकालें?
नियमित (Regular) Rhythm में:
HR = 300 ÷ R-R के बीच बड़े खानों की संख्या
| बड़े खाने (Large Boxes) | Heart Rate |
|---|---|
| 1 | 300 bpm |
| 2 | 150 bpm |
| 3 | 100 bpm |
| 4 | 75 bpm |
| 5 | 60 bpm |
| 6 | 50 bpm |
अनियमित (Irregular) Rhythm में (जैसे AF):
10 सेकंड की strip में जितने QRS → उसे 6 से गुणा करें
12 Leads — कहाँ से देखती हैं?
अंग लीड्स / Limb Leads (सामने का नज़रिया):
| Lead | देखता है |
|---|---|
| I | बायीं तरफ (Left lateral) |
| II | नीचे-बायीं ओर |
| III | नीचे |
| aVR | दाहिने ऊपर (हमेशा negative) |
| aVL | बायीं ऊपर |
| aVF | नीचे (inferior) |
छाती के Leads / Precordial Leads (V1–V6):
| Lead | स्थान |
|---|---|
| V1–V2 | दाहिना वेंट्रिकल |
| V3–V4 | Septum / Anterior |
| V5–V6 | Left Ventricle (lateral) |
R-wave progression: V1 से V6 की तरफ R wave बड़ी होती जाती है — यह सामान्य है।
ECG पढ़ने का क्रम (Systematic Approach)
1. Rate → कितनी धड़कन प्रति मिनट?
2. Rhythm → नियमित है? हर QRS से पहले P है?
3. Axis → Normal: -30° से +90°
4. P Wave → मौजूद? सामान्य आकार?
5. PR → 120–200 ms के बीच?
6. QRS → चौड़ाई < 110 ms? Q waves?
7. ST → सपाट है? ऊपर/नीचे तो नहीं?
8. T Wave → सीधी है? उल्टी तो नहीं?
9. QTc → लंबा तो नहीं?
जरूरी Abnormalities — एक नज़र में
| ECG में दिखे | सोचें |
|---|---|
| PR > 200 ms | 1st Degree AV Block |
| P wave नहीं + अनियमित R-R | Atrial Fibrillation (AF) |
| चौड़ा QRS | BBB / Hyperkalemia |
| ST ऊपर (Elevation) | STEMI / Pericarditis |
| ST नीचे (Depression) | Ischemia / NSTEMI |
| नुकीली T wave | Hyperkalemia |
| उल्टी T wave | Ischemia / Strain / PE |
| लंबा QTc | Drug effect / Electrolyte problem |
| J wave (Osborn) | Hypothermia (ठंड लगना) |
सामान्य ECG कैसी दिखती है?
- हर QRS से पहले P wave है ✅
- Narrow QRS (< 110 ms) ✅
- ST segment सपाट ✅
- सीधी T waves ✅
- Regular rhythm ✅
याद रखें: ECG एक tool है — इसे हमेशा patient की clinical condition के साथ मिलाकर देखें। अकेला ECG कभी पूरी picture नहीं देता।
स्रोत: Goldman-Cecil Medicine; Costanzo Physiology; Braunwald's Heart Disease
This is a shared conversation. Sign in to Orris to start your own chat.