Pain pathway and pain reflex pathway
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information from Harrison's Principles of Internal Medicine (22E) and Ganong's Review of Medical Physiology to give a thorough answer. Here is the full explanation:
Pain Pathway and Pain Reflex Pathway
PART 1: THE PAIN PATHWAY
1. Peripheral Mechanisms - The Primary Afferent Nociceptor
A peripheral nerve contains three types of neurons: primary sensory afferents, motor neurons, and sympathetic postganglionic neurons. Primary sensory afferent cell bodies sit in the dorsal root ganglia (DRG) within the vertebral foramina.
Fiber types involved in pain:
| Fiber | Diameter | Myelination | Conduction | Pain Quality |
|---|---|---|---|---|
| A-beta (Aβ) | Large | Heavy | Fast | Touch only (not pain) |
| A-delta (Aδ) | Small | Thin myelin | Medium | Sharp, fast, well-localized ("first pain") |
| C fibers | Smallest | Unmyelinated | Slow | Dull, burning, diffuse ("second pain") |
Aδ and C fiber afferents are the true nociceptors - pain is completely abolished when their conduction is blocked.
What activates nociceptors:
- Intense heat or cold
- Intense mechanical distortion (pinch)
- Acidic pH (low pH → H⁺ activates TRPV1)
- Chemical mediators: ATP, serotonin, bradykinin (BK), histamine
- TRPV1 (vanilloid receptor) - activated by heat, acidic pH, endogenous mediators, and capsaicin
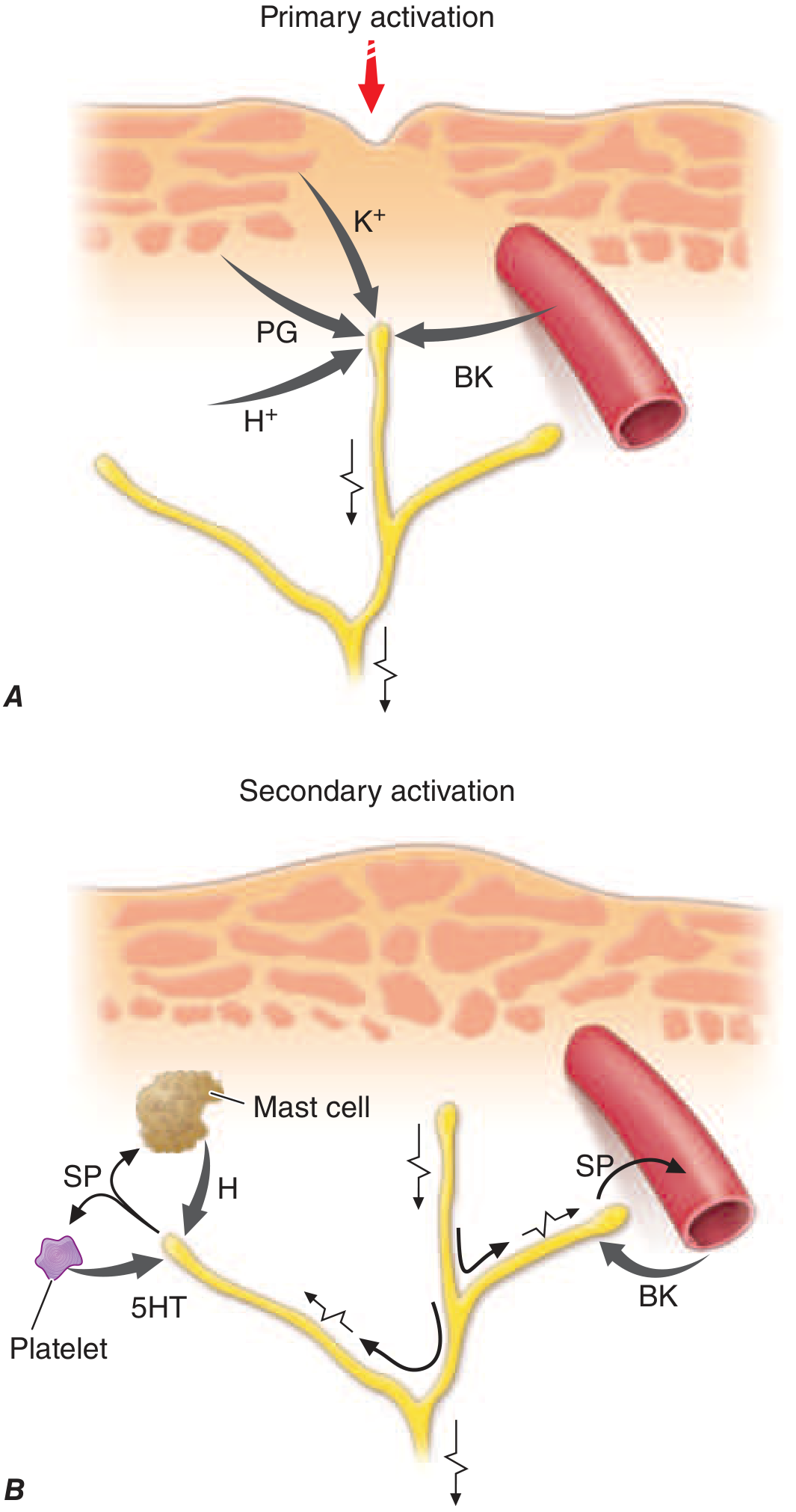
Sensitization: Repeated or intense noxious stimuli lower the threshold of nociceptors (peripheral sensitization). This is mediated by prostaglandins, bradykinin, and substance P, which increase receptor sensitivity and contribute to hyperalgesia and allodynia.
Neurogenic inflammation: Activated nociceptors release substance P, CGRP, and cholecystokinin from their peripheral terminals. Substance P causes vasodilation, mast cell degranulation, leukocyte chemotaxis, and increased release of inflammatory mediators - a neuroeffector function that amplifies local tissue inflammation.
2. Spinal Cord (Central Mechanisms)
Primary afferent nociceptor axons enter the spinal cord via the dorsal root and terminate in the dorsal horn of the spinal gray matter.
- The main neurotransmitter released is glutamate - rapidly excites second-order dorsal horn neurons
- Nociceptors also release substance P and CGRP - produce slower, longer-lasting excitation
- Each primary afferent contacts many spinal neurons; each spinal neuron receives convergent inputs from many primary afferents
Referred Pain: Visceral and somatic afferents converge on the same dorsal horn neurons. The brain cannot distinguish the true source and "projects" the sensation to the somatic structure innervated by the same spinal segment. Example: C3/C4 dorsal root ganglia supply both the central diaphragm and the shoulder/lower neck skin - hence diaphragmatic irritation is felt as shoulder pain.
3. Ascending Pain Pathways
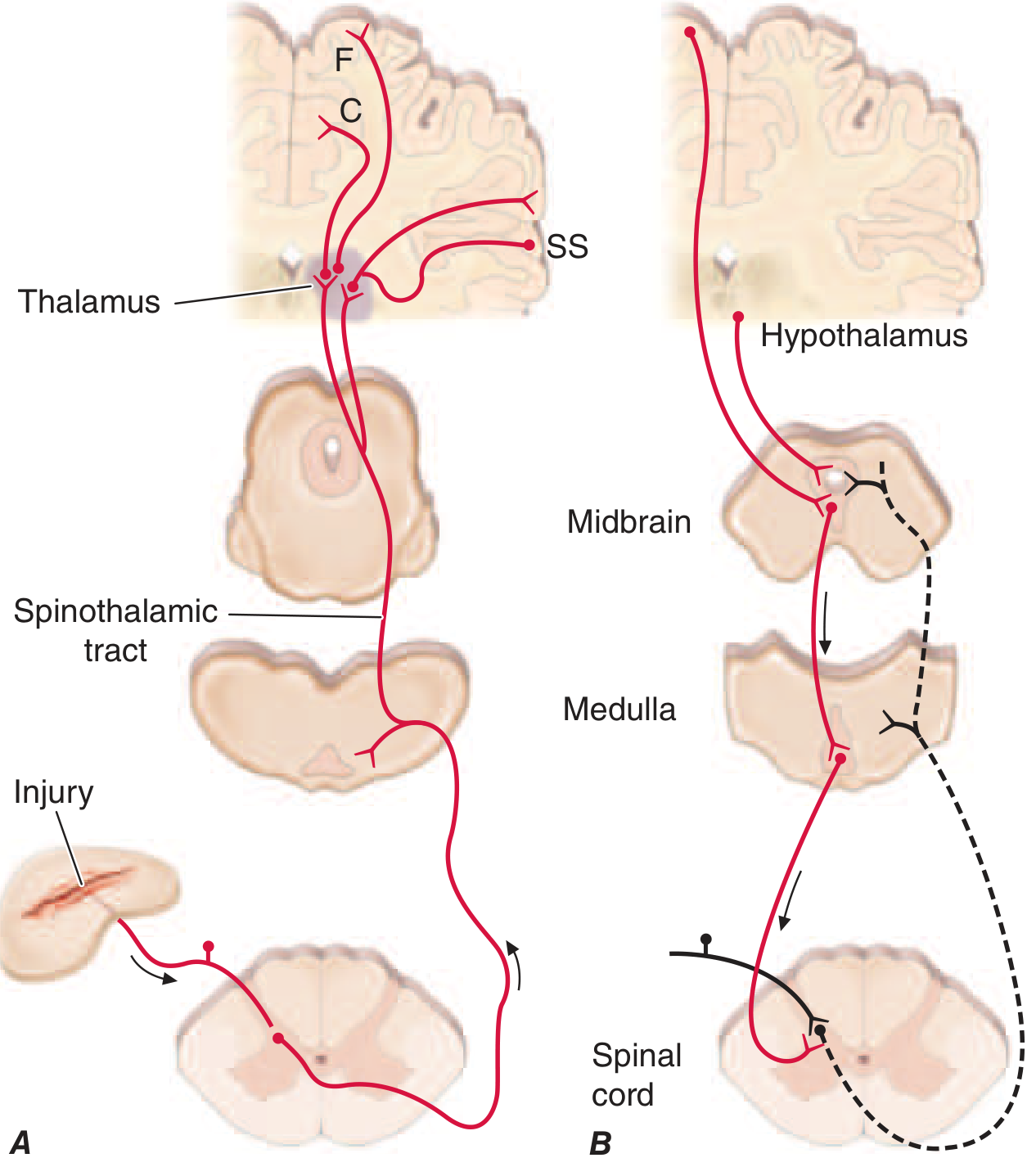
Most second-order dorsal horn neurons send axons to the contralateral thalamus, forming the:
Spinothalamic Tract (STT) - the major ascending pain pathway:
- Lies in the anterolateral white matter of the spinal cord
- Passes through the lateral edge of the medulla, lateral pons and midbrain
- Terminates in the thalamus
- Interruption of this pathway produces permanent deficits in pain and temperature discrimination
From the Thalamus - Divergence to Cortex:
| Projection | Cortical Area | Function |
|---|---|---|
| First | Somatosensory cortex (SS) | Sensory-discriminative: location, intensity, quality |
| Second | Anterior cingulate cortex (C) | Affective/emotional dimension - suffering, fear |
| Third | Frontal insular cortex (F) | Emotional and autonomic responses |
This explains why pain has two components - a sensory component (where does it hurt, how much) and an emotional component (the suffering and fear). Surgical lesions to frontal cortex areas can reduce emotional suffering while preserving the ability to localize pain.
4. Pain Modulation - The Descending System
The perceived intensity of pain is powerfully modulated by a descending circuit:
Descending modulatory pathway:
Frontal cortex / Hypothalamus → Midbrain (PAG) → Medulla (RVM) → Spinal dorsal horn
- This system selectively controls spinal pain-transmission neurons
- All component nuclei contain opioid receptors and endogenous opioid peptides (enkephalins, β-endorphin)
- The most reliable activator is suggestion of pain relief or intense emotion directed away from the pain source (basis for placebo analgesia, stress-induced analgesia)
- This is also the target of opioid analgesic drugs
PART 2: PAIN REFLEX PATHWAY (Withdrawal Reflex)
The withdrawal reflex is the body's protective reflex response to a noxious stimulus. It is a spinal, polysynaptic reflex that does not require cortical involvement.
Components of the Reflex Arc
Noxious stimulus
↓
Nociceptor (Aδ/C fibers in skin/subcutaneous tissue/muscle)
↓
Afferent nerve → Dorsal horn (spinal cord)
↓
Interneurons (polysynaptic pathway)
↓
Motor neurons (anterior horn)
↓
Effectors: Flexor muscle contraction + Extensor inhibition
↓
WITHDRAWAL of body part
Key Features
- Polysynaptic - multiple interneurons are interposed between the afferent input and motor output
- Flexor response - flexors contract, extensors are inhibited (reciprocal inhibition) → limb is flexed and withdrawn from the stimulus
- Crossed extensor response - when a strong noxious stimulus hits one limb, there is simultaneous extension of the opposite limb to support the body. This is properly part of the withdrawal reflex
- Irradiation - very strong stimuli cause activity to spread through the interneuron pool to all four extremities
- After-discharge - strong stimuli cause prolonged, repeated firing of motor neurons due to continued bombardment through circuitous polysynaptic paths - resulting in prolonged or repeated flexion movements
Stimulus Intensity-Response Relationship
| Stimulus Strength | Response |
|---|---|
| Weak noxious | Minimal, quick flexion of one limb |
| Moderate | Greater flexion, longer duration |
| Strong | Prolonged flexion, after-discharge, crossed extensor response |
| Very strong | Mass reflex - all four limbs involved |
Why it is Protective
- Flexion of the stimulated limb gets it away from the source of irritation
- Extension of the opposite limb supports the body (so it doesn't fall)
- The reflex does not need to wait for cortical processing - it occurs at the spinal level, making it rapid
Clinical Significance
- Spinal cord injury (SCI): After complete transection, the withdrawal reflex threshold becomes very low. Even minor noxious stimuli can produce prolonged withdrawal of one extremity with marked flexion-extension patterns in all four limbs. Autonomic neurons are also activated (bladder/bowel evacuation, sweating, blood pressure swings) - this is the mass reflex. This can be used to give some patients with paraplegia voluntary bladder and bowel control by intentionally triggering the mass reflex
- Incomplete cord section: Flexor spasms from noxious stimuli can be associated with painful bursts - treated with baclofen (GABA-B receptor agonist)
- Upper motor neuron lesion: Loss of descending inhibition causes hyperactive stretch reflexes and can contribute to clonus
Summary Comparison
| Feature | Pain (Ascending) Pathway | Pain Reflex (Withdrawal) Pathway |
|---|---|---|
| Purpose | Conscious perception of pain | Protective reflex withdrawal |
| Cortex required? | Yes | No (spinal reflex) |
| Pathway | Nociceptor → STT → Thalamus → Cortex | Nociceptor → Dorsal horn → Interneurons → Motor neuron → Muscle |
| Fiber type | Aδ and C fibers | Aδ and C fibers |
| Synapses | 3 neuron chain (1st, 2nd, 3rd order) | Polysynaptic (multiple interneurons) |
| Side | Crosses to contralateral at spinal cord | Ipsilateral flexion + contralateral extension |
| Speed | Slower (involves brain) | Fast (spinal level) |
| Modulation | Yes (descending opioidergic system) | Limited at spinal level |
Sources: Harrison's Principles of Internal Medicine, 22E (2025), Ch. 14 - Pain: Pathophysiology and Management; Ganong's Review of Medical Physiology, 26th Ed., Ch. 12 - Withdrawal Reflex and Spinal Integration
This is a shared conversation. Sign in to Orris to start your own chat.