Junctional vs extrajunctional receptors
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Here is a thorough comparison of junctional vs. extrajunctional acetylcholine receptors (AChRs), drawn from Miller's Anesthesia, Katzung's Pharmacology, and Morgan & Mikhail's Clinical Anesthesiology.
Junctional vs. Extrajunctional Receptors at the Neuromuscular Junction
Overview
Three postjunctional nicotinic AChR isoforms exist at the NMJ:
- Junctional (mature/adult) receptor
- Extrajunctional (immature/fetal) receptor
- Neuronal α7 receptor (expressed during pathological upregulation)
Structural Differences
| Feature | Junctional (Mature) | Extrajunctional (Immature/Fetal) |
|---|---|---|
| Subunit composition | α1₂ β1 δ ε | α1₂ β1 δ γ |
| Key difference | Contains ε-subunit | Contains γ-subunit (replaces ε) |
| Molecular mass | ~250 kDa | ~250 kDa |
| ACh binding sites | 2 (on both α1 subunits) | 2 (on both α1 subunits) |
The γ- and ε-subunits differ only slightly in amino acid homology, but these differences are enough to significantly alter the receptor's physiologic and pharmacologic behavior.
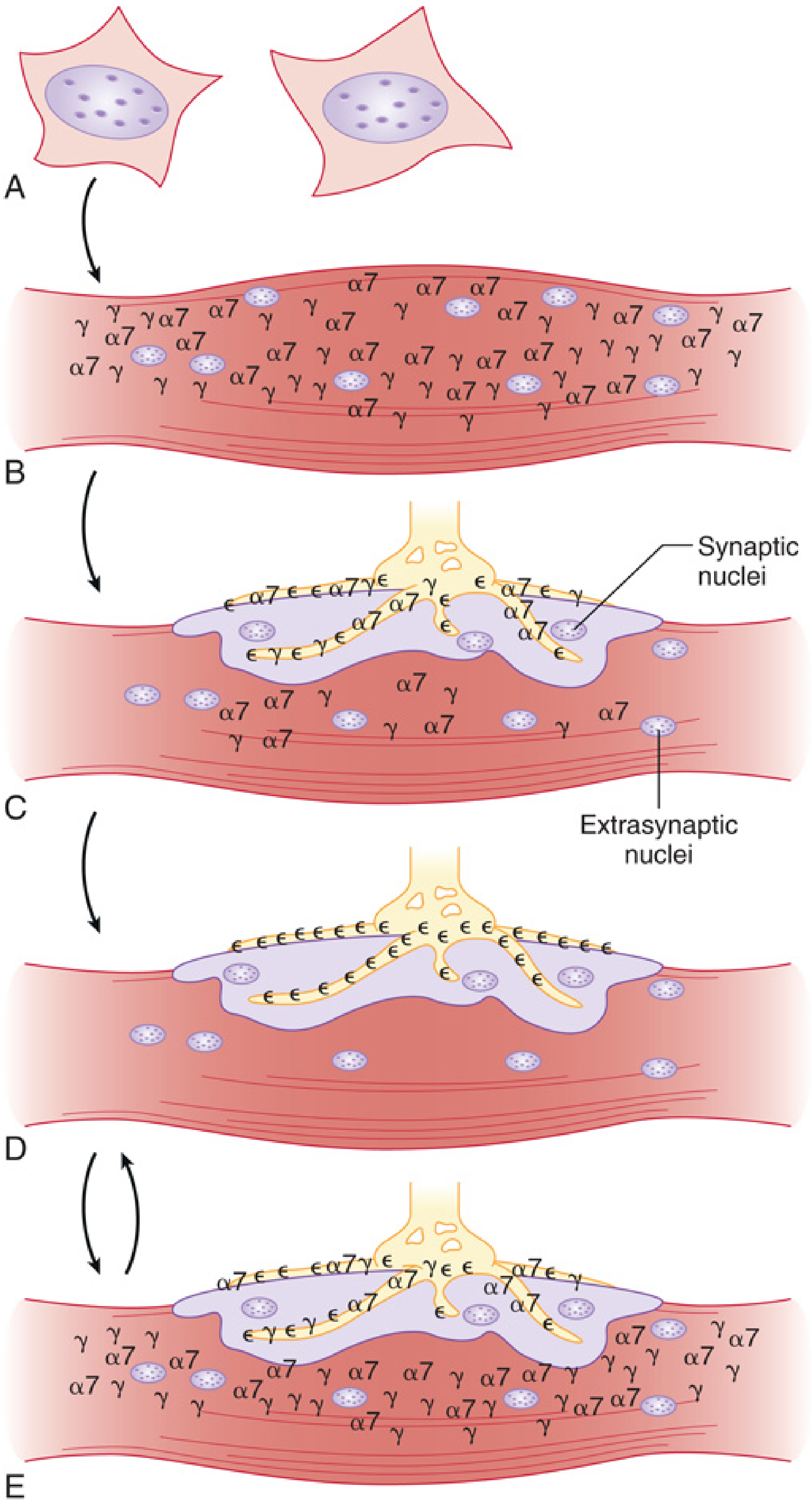
Figure from Miller's Anesthesia: (A-B) Early fetal stage - γ and α7 receptors scattered throughout muscle membrane. (C) Nerve contact - clustering at synapse. (D) Mature innervated muscle - ε-subunit receptors confined to end-plate, no extrajunctional receptors. (E) Denervation/pathological state - re-expression of γ and α7 receptors throughout extrajunctional areas.
Location
| Junctional | Extrajunctional | |
|---|---|---|
| Normal adult muscle | Confined strictly to the end-plate (NMJ) | Absent (or negligible) |
| Fetal/developing muscle | Absent (before innervation) | Scattered throughout entire muscle membrane |
| Pathological states | Present at end-plate | Proliferate widely across the entire muscle membrane, including perijunctional area |
Physiological Differences
| Feature | Junctional | Extrajunctional |
|---|---|---|
| Channel open time | Shorter (~1 ms) | Longer (several ms) - the γ-subunit prolongs channel opening |
| Conductance | Higher | Lower |
| Turnover rate | Slow (half-life ~2 weeks) | Fast (half-life ~24 hours) |
| Sensitivity to ACh | Normal | Increased sensitivity |
When Extrajunctional Receptors Appear (Upregulation)
Extrajunctional receptors proliferate whenever muscle is deprived of normal neural activity or undergoes catabolism:
- Denervation (upper or lower motor neuron injury, spinal cord injury)
- Thermal burns
- Prolonged immobilization (ICU patients, bed rest)
- Stroke, encephalitis, Guillain-Barre syndrome
- Severe sepsis / generalized inflammation
- Closed head injury
- Myopathies (e.g., Duchenne muscular dystrophy)
Key point: This is NOT the same as simple malnutrition - pure malnutrition/wasting without neural disruption does not trigger extrajunctional upregulation.
Pharmacological Significance
1. Succinylcholine and Hyperkalemia - The Critical Danger
Normal depolarization by succinylcholine raises serum K⁺ by ~0.5 mEq/L. In patients with extrajunctional upregulation, succinylcholine can depolarize millions of receptors spread across the entire muscle surface, releasing massive amounts of intracellular K⁺:
- Can cause life-threatening hyperkalemia sufficient to precipitate cardiac arrest
- The α7 receptors (also upregulated) are depolarized by succinylcholine AND its metabolite choline (a full agonist at α7), with minimal desensitization - prolonging K⁺ leak
- Not reliably prevented by pretreatment with a non-depolarizing agent
- Risk peaks at 7-10 days after injury; minimal risk in the first 48 hours after spinal cord or burn injury
Treatment of hyperkalemic cardiac arrest from succinylcholine requires calcium, insulin+glucose, bicarbonate, and potentially cardiopulmonary bypass.
2. Response to Non-Depolarizing Relaxants (NDMRs)
Extrajunctional upregulation causes resistance to NDMRs (e.g., rocuronium, vecuronium). More drug is needed to block the greatly increased total number of receptors. This is the basis for "resistant" neuromuscular blockade in burn patients and chronic ICU patients.
3. Summary Table
| Drug class | Junctional (normal) | Extrajunctional (upregulated) |
|---|---|---|
| Succinylcholine | Normal ~0.5 mEq/L K⁺ rise | Massive hyperkalemia, cardiac arrest |
| NDMRs | Normal dose | Resistance - larger doses needed |
The α7 Receptor - A Third Isoform
During the same upregulating conditions (burns, immobilization, sepsis, denervation), α7 homomeric receptors also appear. These are pentamers of five identical α7 subunits (no conventional α1/β1/δ/ε subunits). Their key features:
- Choline is a full agonist at α7 (vs. weak agonist at conventional AChRs)
- Succinylcholine depolarizes α7 AChRs
- Minimal desensitization means prolonged K⁺ leakage
- They contribute significantly to succinylcholine-induced hyperkalemia
Clinical Bottom Line
| Situation | Receptors present | Clinical risk |
|---|---|---|
| Normal innervated adult muscle | Junctional (ε) only, at end-plate | None |
| First 48h after burn/cord injury | Primarily junctional still | Low (succinylcholine relatively safe) |
| >48h-72h after denervation/burn/prolonged immobility | Junctional + widespread extrajunctional (γ) + α7 | Avoid succinylcholine; use rocuronium |
| Recovery/re-innervation | Extrajunctional gradually resolve | Risk decreasing |
Sources: Miller's Anesthesia 10e, pp. 1170-1200; Katzung's Basic & Clinical Pharmacology 16e, p. 745; Morgan & Mikhail's Clinical Anesthesiology 7e, p. 385-386
Burn and suchol when can we use
Finding Sources
Finding Sources
Reading File
Reading File
The textbooks give slightly different cutoffs - here is the complete picture reconciled across sources:
Succinylcholine in Burn Patients: When Is It Safe?
The Core Rule
Succinylcholine is safe early, dangerous later. The danger window is driven by how long it takes for extrajunctional receptors to proliferate to dangerous levels.
Safe Window
| Source | Safe to use |
|---|---|
| Rosen's Emergency Medicine | < 5 days after burn |
| Morgan & Mikhail's Clinical Anesthesiology | < 2 days after burn (minimal risk) |
| Miller's Anesthesia | < 48-72 hours after burn |
| Tintinalli's Emergency Medicine | < 5 days after burn |
Practical consensus: Succinylcholine is considered safe within the first 24-48 hours (some say up to 5 days), and remains the drug of choice for RSI in that early window - including for difficult airway management in acute burns.
"Succinylcholine remains the agent of choice for RSI in acute burn, trauma, stroke, and spinal cord injury if intubation occurs earlier than 5 days after onset of the condition." - Rosen's Emergency Medicine
Dangerous Window
| Condition | Period of danger |
|---|---|
| Burns >10% BSA | >5 days after injury until wounds are fully healed |
| Crush injury | >5 days until wounds healed |
| Denervation (stroke, spinal cord injury) | >5 days until ~6 months post-injury |
| ALS, MS, Muscular Dystrophy | Indefinitely (from onset of disease) |
| Intraabdominal sepsis | >5 days until infection resolves |
Key facts about the danger period:
- Receptor upregulation starts as early as 3 days but does not reach dangerous levels until >5 days
- In burns, risk persists until wounds are healed (can be months in large burns)
- Resistance to NDMRs (rocuronium, vecuronium) has been reported even 463 days after burn injury in pediatric patients - meaning the extrajunctional receptor upregulation can persist far longer than most clinicians assume
- Aggravating factors (immobilization, malnutrition, ICU myopathy, contractures) prolong and worsen the hyperkalemic risk
What to Use Instead (After the Safe Window)
- Rocuronium is the drug of choice for RSI in burn patients when succinylcholine is contraindicated
- Dose must be significantly increased (burn patients are resistant to NDMRs due to receptor upregulation)
- Onset time is prolonged, duration is shortened
- Sugammadex can reverse rocuronium if needed
- NDMRs in general require higher doses in burn patients - the degree of resistance correlates with burn size and time after injury
If Timing Is Uncertain
"If doubt exists regarding the onset time, succinylcholine should be replaced with rocuronium." - Rosen's Emergency Medicine
When in doubt, default to rocuronium + sugammadex availability.
Sources: Rosen's Emergency Medicine, p. 34; Morgan & Mikhail's Clinical Anesthesiology 7e, p. 386; Miller's Anesthesia 10e, p. 12383-12384; Tintinalli's Emergency Medicine
When can we use suchol agsin
Based on what we already have in context from the previous searches, here is the direct answer:
When Can Succinylcholine Be Used Again After Burns?
Burns
Succinylcholine can be used again once the burn wounds are fully healed.
The danger period is: >5 days after injury → until wounds are completely healed
There is no fixed number of weeks/months - it depends entirely on wound healing. Large burns (e.g., >40% BSA) may take months to heal, meaning succinylcholine stays contraindicated for that entire period.
Comparison with Other Conditions
| Condition | Danger period | Safe again when? |
|---|---|---|
| Burns >10% BSA | >5 days post-injury | After wounds fully healed |
| Crush injury | >5 days post-injury | After wounds fully healed |
| Spinal cord injury / Stroke | >5 days post-injury | ~6 months after the original insult (upregulated receptors eventually regress with re-innervation) |
| ALS, MS, Muscular Dystrophy | From disease onset | Never - risk is indefinite |
| Intraabdominal sepsis | >5 days | After infection fully resolves |
Key Points
- For burns, there is no fixed time like "6 months" - the endpoint is wound healing, not a calendar date
- For neurological injuries (stroke, spinal cord), re-innervation eventually causes extrajunctional receptors to regress, making succinylcholine safe again around 6 months post-injury
- For degenerative neuromuscular diseases (ALS, Duchenne MD, MS), receptor upregulation is ongoing and permanent - succinylcholine is never safe in these patients regardless of apparent stability of symptoms
Bottom line for burns: Safe early (first 24-48h), dangerous from day 5 onward, and safe again only after the burn wounds are completely healed.
Source: Rosen's Emergency Medicine; Morgan & Mikhail's Clinical Anesthesiology 7e
This is a shared conversation. Sign in to Orris to start your own chat.