Imaging techniques of heart murmurs
Reading File
Finding Sources
Finding Sources
Searching PubMed
heart murmur echocardiography imaging evaluation
Searching the Web
imaging techniques heart murmurs echocardiography cardiac MRI 2024 2025
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive, high-quality content from multiple authoritative textbooks. Let me compile the full answer.
Imaging Techniques for Heart Murmurs
Heart murmurs are investigated through a stepwise multimodality imaging strategy. The approach begins with non-invasive bedside and basic imaging, progressing to advanced cross-sectional modalities when needed. The goal is to determine: (1) which valvular or structural abnormality is present, (2) its severity, (3) the degree of ventricular impairment, and (4) whether coronary artery disease co-exists.
Echocardiographic Differential Diagnosis of a Murmur
The echocardiographic workup is organized anatomically, since the clinician often has limited auscultatory data at the time of referral:
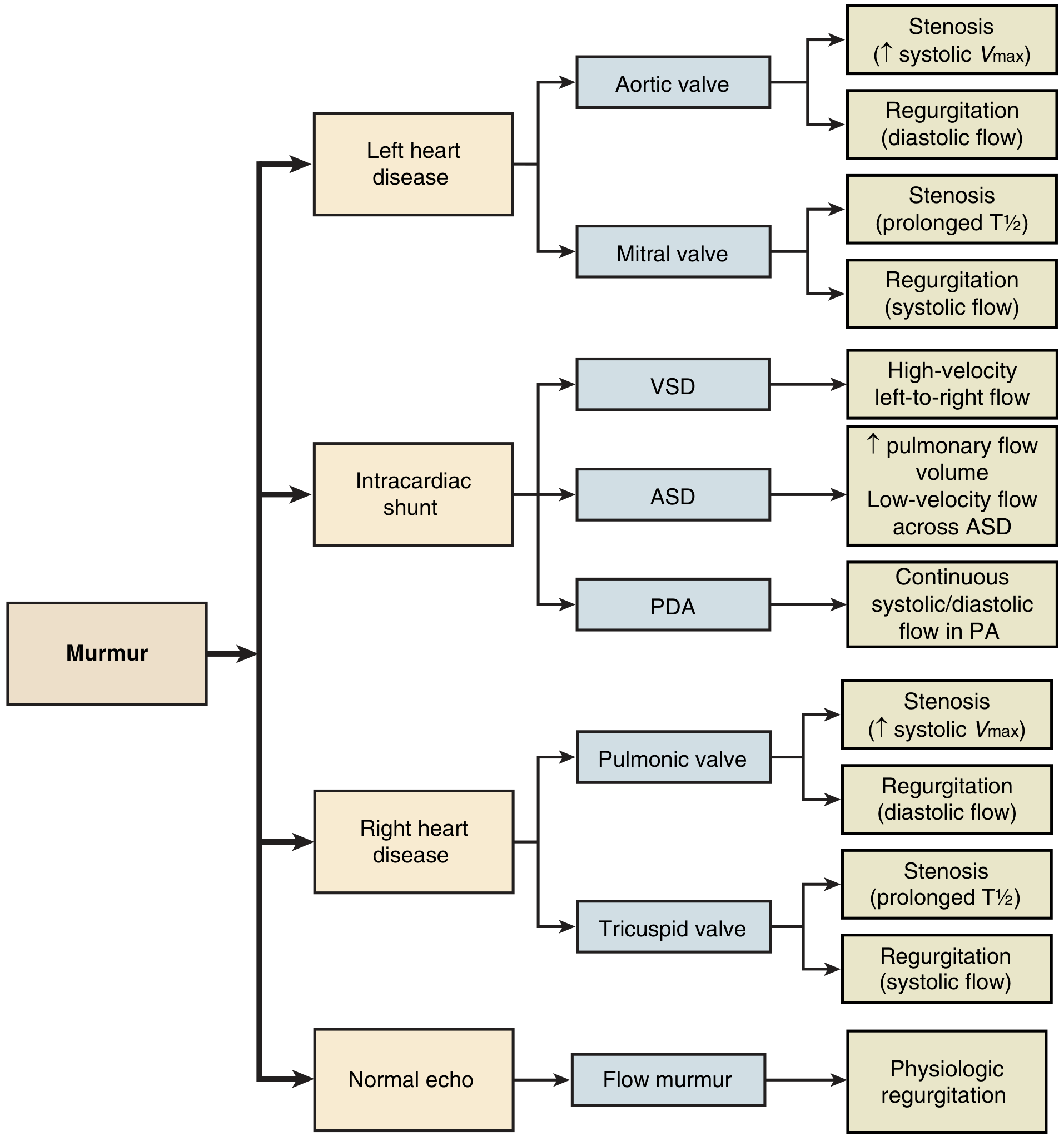
Echocardiographic differential diagnosis of a murmur — arranged by anatomy (left heart, intracardiac shunts, right heart, or normal echo). — Textbook of Clinical Echocardiography, Fig. 5.8
1. Chest Radiograph (CXR)
The first-line plain imaging study. It provides:
- Cardiac silhouette size — cardiomegaly suggests dilated cardiomyopathy or large pericardial effusion
- Pulmonary vascularity — increased flow in ASD/VSD; pulmonary venous congestion in mitral stenosis
- Calcification — calcified aortic valve or ductal calcification in older PDA patients
- Aortic root / ascending aorta dilation — seen in aortic stenosis or regurgitation
A systolic murmur grade ≥3, any diastolic murmur, or an abnormal CXR mandates echocardiography. — Harrison's Principles of Internal Medicine 22E, p. 291
2. Transthoracic Echocardiography (TTE) — Mainstay of Diagnosis
TTE is the primary diagnostic test for virtually all heart murmurs. It provides simultaneous anatomic and physiologic information. Common indications include:
| Clinical Setting | Role of TTE |
|---|---|
| New murmur (grade ≥3 or diastolic) | Initial evaluation of etiology and severity |
| Valve regurgitation | Routine reassessment every 6–12 months |
| Valve stenosis | Routine reassessment every 1–3 years |
| Suspected endocarditis | New murmur + fever/positive blood cultures |
| Prosthetic valve | Baseline postoperative study; reassessment for dysfunction |
TTE Modalities within Echocardiography
| Modality | What it shows |
|---|---|
| 2D imaging | Valve morphology, leaflet structure, chamber size, wall motion |
| M-mode | Precise timing of valve opening/closure, LV dimensions |
| Color flow Doppler | Direction and turbulence of regurgitant jets; shunt detection |
| Continuous-wave (CW) Doppler | Peak velocity and pressure gradient across stenotic valves |
| Pulsed-wave (PW) Doppler | Localization of flow disturbances; pulmonary venous patterns |
Key findings by etiology:
- Aortic stenosis → elevated systolic Vmax; reduced valve area by planimetry
- Aortic regurgitation → diastolic regurgitant flow on color Doppler; holodiastolic reversal in descending aorta
- Mitral stenosis → prolonged pressure half-time (T½); doming leaflets
- Mitral regurgitation → systolic color flow into LA; vena contracta width
- VSD → high-velocity left-to-right flow in interventricular septum
- ASD → increased pulmonary flow volume; low-velocity flow across the defect
- PDA → continuous systolic/diastolic flow in pulmonary artery
Important limitation: When the Doppler beam is not well aligned with the velocity jet, the severity of stenosis will be underestimated. — Fuster and Hurst's The Heart, 15th Ed.
Stress Echocardiography
Exercise or pharmacologic (dobutamine) stress echo reveals hemodynamically significant lesions that are equivocal at rest, particularly in low-gradient aortic stenosis with impaired LV function. — Textbook of Clinical Echocardiography
3. Transesophageal Echocardiography (TEE)
TEE is indicated when:
- TTE windows are limited (obesity, chest deformity, COPD)
- Posterior structures need superior resolution
- Endocarditis is suspected — TEE has convincingly superior sensitivity for paravalvular abscess detection
- Detailed mitral valve anatomy for repair planning
- Intraoperative guidance during valve surgery
TEE should not be reflexively ordered; its slight but definite procedural risk must be weighed against the incremental diagnostic yield. — Textbook of Clinical Echocardiography
4. Cardiac Magnetic Resonance (CMR) Imaging
CMR provides quantitative information not achievable by echo alone:
| Parameter | CMR Capability |
|---|---|
| Regurgitant volume and fraction | Precise phase-contrast velocity mapping |
| Regurgitant orifice area | Planimetry on cine images |
| LV/RV volumes and ejection fraction | Gold standard |
| Myocardial perfusion and fibrosis | Late gadolinium enhancement |
| Aortic valve leaflet number (bi- vs. tricuspid) | When TTE is ambiguous |
| Aortic root and ascending aortic anatomy | Pre-TAVI/pre-surgery planning |
| Shunt quantification | Qp:Qs ratio |
CMR has largely supplanted cardiac catheterization for invasive hemodynamic assessment when there is a discrepancy between clinical and echocardiographic findings in regurgitant valve disease (MR or AR). — Harrison's Principles of Internal Medicine 22E, p. 291
In aortic regurgitation, CMR permits precise assessment of regurgitant volume and assessment of the volume/function of the eccentrically hypertrophied LV — beyond what semiquantitative color Doppler provides. — Grainger & Allison's Diagnostic Radiology
5. Cardiac Computed Tomography (CT / CTA)
| Application | Details |
|---|---|
| Aortic valve anatomy | Leaflet count, calcification, annulus sizing for TAVI |
| Aortic root and ascending aorta | Aneurysm screening (especially with bicuspid valve — ~1/3 develop aortic aneurysm) |
| Coronary CT angiography (CCTA) | Exclude CAD before valve surgery in low-to-intermediate pretest probability patients |
| Paravalvular leak assessment | Post-TAVI evaluation |
Both CMR and cardiac CT provide aortic valve leaflet number assessment when TTE is uncertain about bi- vs. tricuspid morphology. Coronary CTA to exclude CAD prior to valve surgery has gained wide acceptance. — Harrison's Principles of Internal Medicine 22E, p. 291; Goldman-Cecil Medicine
6. Cardiac Catheterization and Invasive Hemodynamics
Now reserved for cases where non-invasive imaging is discordant with clinical findings or inconclusive. Questions addressed:
- Which valvular abnormality is hemodynamically dominant?
- What is the true severity of the lesion?
- What degree of ventricular impairment is present?
- Is there significant coronary artery disease?
Invasive angiography and hemodynamic assessment may still be required for a complete preoperative evaluation in select cases. — Morgan & Mikhail's Clinical Anesthesiology, 7e; Goldman-Cecil Medicine
Summary: Stepwise Imaging Approach
Murmur detected
│
├─ CXR + ECG (first-line)
│
├─ TTE with Doppler (mainstay — evaluates all 4 valves, shunts)
│ ├─ Diagnostic → graded follow-up per severity
│ └─ Non-diagnostic / limited windows
│ │
│ ├─ TEE (posterior structures, endocarditis)
│ ├─ CMR (quantitative regurgitation, shunts, LV/RV function)
│ └─ Cardiac CT (valve anatomy, aorta, coronary exclusion)
│
└─ Cardiac catheterization (if clinical–echo discordance persists)
Key references:
- Textbook of Clinical Echocardiography — TTE/TEE indications, Figs. 5.7–5.8
- Harrison's Principles of Internal Medicine 22E — Integrated murmur workup, pp. 284–291
- Goldman-Cecil Medicine — Valvular heart disease multimodality imaging
- Grainger & Allison's Diagnostic Radiology — CMR/CT in valvular and congenital heart disease
- Morgan & Mikhail's Clinical Anesthesiology, 7e — Preoperative murmur evaluation
This is a shared conversation. Sign in to Orris to start your own chat.