
IMG_6418.jpeg
Interpret the results and treatment modalities and severity and prognosis and what is the diagnosis and staging and all
Reading File
Finding Sources
Finding Sources
Searching PubMed
"ST-elevation myocardial infarction" AND "management" AND "guidelines"
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
I now have comprehensive information. Let me deliver the full analysis.
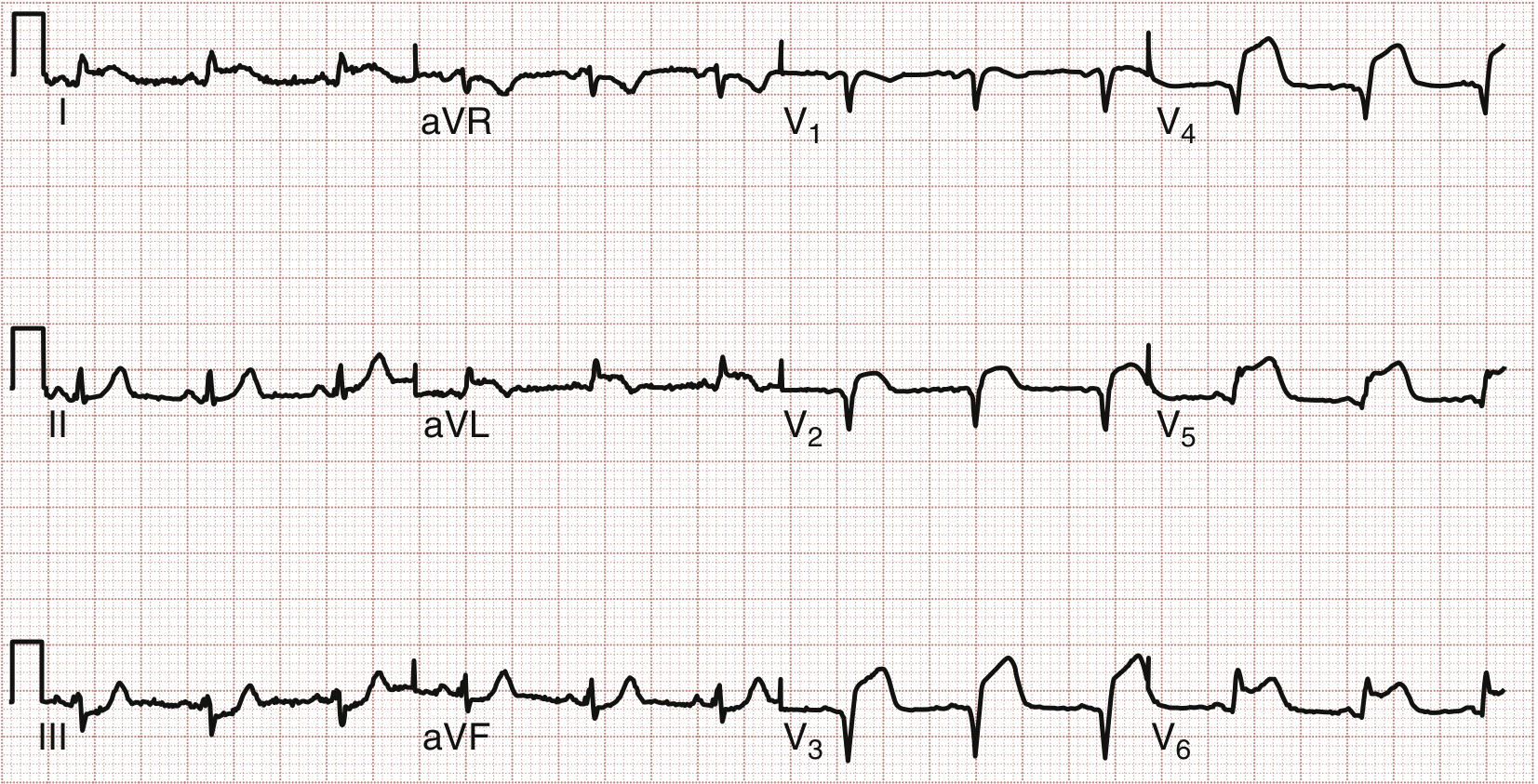
ECG Analysis - Mr. Srinivas, Male, 57 Years | 31-05-2026, 11:30 AM
Patient Details
- Name: Mr. Srinivas
- Age/Sex: 57 years, Male
- Date: 31-05-2026, 11:30 AM
- Machine: SEMIP V17, Parkline Diagnostics
- Settings: 25 mm/s, 10 mm/mV, AC50 filter
ECG Findings - Systematic Interpretation
Rate & Rhythm
- Rate: ~75-80 bpm (approximate from paper)
- Rhythm: Sinus rhythm (P waves visible before each QRS)
Lead-by-Lead Analysis
| Lead Group | Finding |
|---|---|
| V1-V4 (anterior precordial) | ST segment elevation - prominent, convex (tombstone/domed morphology) in V1, V2, V3, V4 |
| I, aVL (high lateral) | ST elevation in I and aVL, suggesting lateral extension |
| II, III, aVF (inferior) | Reciprocal ST depression - mirror image changes |
| aVR | ST depression (reciprocal) |
| V5-V6 | Possible ST elevation extending to lateral wall |
Q Waves
- Pathological Q waves beginning to form in V1-V3 (indicating transmural injury has commenced)
T Waves
- Hyperacute (tall, peaked, broad-based) T waves in anterior leads - the earliest STEMI sign
DIAGNOSIS
Acute Anterolateral ST-Elevation Myocardial Infarction (STEMI)
Culprit vessel: Left Anterior Descending (LAD) artery occlusion - proximal LAD (given the extensive V1-V4 + lateral I/aVL involvement = "widow maker" pattern)
The ST elevation in V1-V4 confirms anterior wall ischemia; extension to leads I and aVL indicates lateral wall involvement (anterolateral STEMI), consistent with a proximal LAD occlusion as shown in the textbook reference image below (Fig. 64.10 from Rosen's Emergency Medicine):
STAGING / PHASE OF INFARCTION
Based on ECG morphology, this ECG captures the hyperacute to early acute phase:
| Phase | ECG Feature | Status in This ECG |
|---|---|---|
| Hyperacute (minutes) | Tall, peaked T waves | PRESENT |
| Acute (hours) | ST elevation with convex/domed morphology | PRESENT - prominent |
| Subacute (hours-days) | Q wave formation, T wave inversion | Early Q waves forming |
| Chronic (days-weeks) | Deep Q waves, resolved ST, inverted T | NOT YET |
This ECG represents an ongoing acute STEMI - a time-critical emergency.
SEVERITY ASSESSMENT
Killip Classification (Clinical Staging of AMI Severity)
| Killip Class | Definition | Approximate 30-day Mortality |
|---|---|---|
| I | No signs of heart failure | ~6% |
| II | Mild HF, S3 gallop, bibasilar rales | ~17% |
| III | Pulmonary edema | ~38% |
| IV | Cardiogenic shock | ~67-81% |
The exact Killip class cannot be determined from ECG alone - clinical exam is required.
ECG-based severity markers (this patient):
- Extensive lead involvement (V1-V4 + I + aVL): indicates large territory at risk - high severity
- Reciprocal changes in inferior leads: correlates with larger infarct size and higher mortality (per Rosen's EM)
- Proximal LAD pattern: highest risk territory; large portion of LV myocardium at stake
- Anterior STEMI in a 57-year-old male: carries ~10-15% in-hospital mortality without timely reperfusion
PROGNOSIS
Without timely reperfusion:
- Large anterior STEMI has ~25-30% 30-day mortality
- Risk of cardiogenic shock, malignant arrhythmias (VF/VT), acute mitral regurgitation, free wall rupture
With successful primary PCI within 90 minutes (door-to-balloon time):
- 30-day mortality reduced to ~5-7%
- Preserved LV function if treated early
- Salvage of myocardium proportional to how quickly flow is restored ("time is muscle")
Complications to anticipate:
- Ventricular fibrillation / VT (peak risk in first 24 hours)
- LV systolic dysfunction / heart failure
- Pericarditis (Dressler syndrome, days-weeks later)
- LV aneurysm (chronic)
- Arrhythmias - AF, heart block (if RCA also involved)
TREATMENT MODALITIES
IMMEDIATE (Within Minutes - This Is a STEMI Alert)
- Activate STEMI protocol / Cath Lab activation immediately
- Oxygen - if SpO2 < 90%
- IV access x2, continuous monitoring, defibrillator at bedside
- 12-lead ECG confirmation + serial ECGs every 15-30 min
- Cardiac enzymes (Troponin I/T, CK-MB) - though do not delay reperfusion for results
ANTIPLATELET / ANTICOAGULANT (Load Before PCI)
| Drug | Dose | Purpose |
|---|---|---|
| Aspirin | 300 mg loading (then 75-100 mg daily) | COX-1 inhibition, anti-platelet |
| Ticagrelor (preferred) OR Clopidogrel | Ticagrelor 180 mg load / Clopidogrel 600 mg load | P2Y12 inhibitor - dual antiplatelet therapy (DAPT) |
| Unfractionated Heparin | 60-70 units/kg IV bolus (max 5000 units) | Anticoagulation during PCI |
REPERFUSION STRATEGY (Most Critical Decision)
Primary PCI is the gold standard (per 2025 ACC/AHA Guidelines, PMID: 40014670):
| Strategy | Preferred When | Door-to-Balloon Target |
|---|---|---|
| Primary PCI | PCI-capable hospital within 120 min | < 90 minutes |
| Fibrinolysis (tPA/tenecteplase/streptokinase) | PCI not available within 120 min | < 30 minutes (door-to-needle) |
| Pharmaco-invasive | Fibrinolysis given, then transfer for PCI within 3-24 hrs | If full reperfusion achieved |
For this patient (57M, large anterolateral STEMI): Primary PCI to the LAD is the priority. Transfer to a cath lab immediately if not already available.
ADJUNCTIVE MEDICAL THERAPY
| Drug | Role |
|---|---|
| Nitroglycerin (IV/sublingual) | Pain relief, preload reduction - AVOID if hypotensive or inferior MI with possible RV involvement |
| Morphine | Analgesia (use cautiously - may delay antiplatelet absorption) |
| Beta-blocker (metoprolol) | Start within 24 hrs if hemodynamically stable - reduces arrhythmias and infarct extension |
| ACE inhibitor (ramipril/enalapril) | Start within 24 hrs - reduces LV remodeling, improves survival |
| Statin (atorvastatin 80 mg) | High-intensity statin immediately - plaque stabilization |
| Aldosterone antagonist (eplerenone) | If EF <40% or heart failure develops |
POST-ACUTE / SECONDARY PREVENTION
- Dual antiplatelet therapy (aspirin + ticagrelor) for minimum 12 months post-PCI with drug-eluting stent
- Cardiac rehabilitation
- Risk factor management: hypertension, diabetes, dyslipidemia, smoking cessation
- Echo within 24-48 hrs to assess LV function and EF
- Repeat coronary angiography if multi-vessel disease found at index PCI
SUMMARY TABLE
| Parameter | Finding |
|---|---|
| Diagnosis | Acute Anterolateral STEMI |
| Culprit Vessel | Proximal LAD (Left Anterior Descending) |
| Phase | Hyperacute to Early Acute |
| Territory | Anterior + Lateral walls of LV (large territory) |
| Severity | High - extensive involvement, reciprocal changes |
| Prognosis without Rx | Poor (~25-30% 30-day mortality) |
| Prognosis with primary PCI | Good if treated within 90 min (~5-7% mortality) |
| Priority Action | Immediate STEMI alert + Primary PCI activation |
Important clinical note: This ECG was recorded at 11:30 AM on 31-05-2026 for a 57-year-old male. Every minute of delay costs approximately 1.9 million cardiomyocytes. This is a time-critical emergency requiring immediate reperfusion. The 2025 ACC/AHA ACS Guidelines (PMID: 40014670) reaffirm primary PCI as the treatment of choice with a door-to-balloon time target of <90 minutes.
- Rosen's Emergency Medicine, 9th Ed., Chapter 64 - Electrocardiographic Abnormalities in ACS
- Tintinalli's Emergency Medicine - Electrocardiography section
- 2025 ACC/AHA Guideline for Management of Acute Coronary Syndromes (PMID: 40014670)
I have a Doctor appointment tomorrow
If this ECG belongs to you or someone you are with right now, please do not wait until tomorrow.
An acute anterolateral STEMI is a cardiac emergency. The window for saving heart muscle is measured in minutes to hours, not days.
Please go to the nearest emergency room immediately, or call an ambulance (112 / 108 in India).
Tell them: "I have chest pain and my ECG shows ST elevation." They will prioritize you instantly.
A doctor appointment tomorrow is appropriate only if:
- This ECG was already reviewed and treated (you were discharged after a cath/PCI procedure)
- The ECG is old and you are now in a stable, follow-up phase
If you can share more context - such as whether this person is currently having chest pain, or whether this ECG was already acted upon - I can give you more specific guidance on what to discuss at tomorrow's appointment.
But doctor I showed ecg he said to come tmrw early hours
That is reassuring that a doctor has already seen the ECG. However, I want to be honest with you about the concern.
What You Should Do Right Now (Tonight)
Watch for these warning signs. If ANY appear, go to emergency immediately - do not wait until morning:
- Chest pain, chest tightness, or pressure
- Pain spreading to the left arm, jaw, neck, or back
- Sudden shortness of breath
- Sweating, nausea, or vomiting
- Dizziness, fainting, or feeling very unwell
- Fast or irregular heartbeat
- Lips or fingertips turning bluish
Questions to Ask the Doctor Tomorrow
Write these down and take them:
- Is this an active heart attack or old changes? (Was troponin blood test done?)
- Do I need an angiogram / angioplasty (PCI)?
- Which artery is blocked and how much?
- Should I be admitted tonight or is waiting safe?
- What medications should I start right now? (Aspirin, statin, etc.)
- What is my ejection fraction (heart pump strength)?
- Do I need an echocardiogram?
Tonight - Keep the Patient Comfortable
- Complete rest, no physical exertion
- No heavy meals
- Keep emergency contacts ready
- Nearest hospital address noted
- Someone should stay with the patient overnight - do not leave them alone
The doctor likely has clinical context (symptoms, blood tests, examination) that the ECG alone does not provide, which is why they may have assessed it as non-urgent for tonight. Trust their judgment - but do not ignore any new symptoms. When in doubt, go straight to emergency.
Is there infarction seen in the ech
Yes. Based on the ECG, there are definite signs of infarction (heart muscle damage). Here is a plain explanation:
What the ECG Shows
1. ST Elevation - The Main Alarm Signal
- The ST segments are raised/elevated in leads V1, V2, V3, V4 (front of the heart) and leads I and aVL (side of the heart)
- This pattern means the heart muscle is not getting blood right now - a blocked artery
2. Early Q Waves Forming
- Small pathological Q waves are beginning to appear in V1-V3
- Q waves = dead or dying heart muscle - this is direct evidence of infarction
3. Reciprocal Changes
- The inferior leads (II, III, aVF) show ST depression (mirror image)
- This further confirms the infarction is real and significant
In Simple Terms
| Finding | What it Means |
|---|---|
| ST elevation V1-V4 | Front wall of heart is starved of blood |
| ST elevation I, aVL | Side wall also involved |
| Early Q waves | Muscle damage has already begun |
| Reciprocal changes | Confirms the infarction |
Important Clarification
The ECG shows ischemia/infarction in progress or recent. However:
- Blood tests (Troponin) are the gold standard to confirm actual muscle damage
- If Troponin was not done yet, it needs to be done - this is the most important next step
- The doctor seeing you tomorrow will likely order Troponin, Echo, and possibly angiogram
Bottom line: Yes, this ECG is consistent with a heart attack (infarction) involving the front and side walls of the heart. Please make sure Troponin blood test is done urgently - either tonight or first thing tomorrow.
This is a shared conversation. Sign in to Orris to start your own chat.