Hernia. Clinical classification. General characteristics of hernia.Rare forms of hernia
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the material needed for a comprehensive answer. Here is the full structured overview:
Hernia: Clinical Classification, General Characteristics, and Rare Forms
1. Definition
A hernia is the protrusion of an organ, tissue, or part of an organ through an abnormal opening or weakened area in the wall of the cavity that normally contains it. Nearly 10% of the population will develop some form of hernia during their lifetime, making it among the most common surgical problems.
— Tintinalli's Emergency Medicine
2. General Characteristics of a Hernia
Every hernia has three essential anatomical components:
| Component | Description |
|---|---|
| Hernial orifice (defect/ring/neck) | The abnormal opening or weak point in the containing wall through which contents protrude |
| Hernial sac | A peritoneal pouch that has been pushed through the defect; may be absent in internal hernias |
| Hernial contents | What lies within the sac — most commonly omentum or small bowel, but any solid or hollow abdominopelvic viscus can be partly or completely contained |
Predisposing Factors
Anything that increases intraabdominal pressure or weakens the abdominal wall predisposes to hernia formation:
- Chronic cough (e.g., COPD)
- Obesity, ascites, constipation, bladder outlet obstruction, heavy lifting
- Male sex, advancing age, low BMI
- Prior surgery, trauma, congenital defects, pregnancy, collagen disorders, smoking
3. Clinical Classification
Hernias are classified along several intersecting axes:
3.1 By Anatomical Location
| Category | Types |
|---|---|
| Groin (inguinal) | Indirect inguinal, direct inguinal, femoral |
| Ventral / abdominal wall | Umbilical, epigastric, incisional, Spigelian, paramedian |
| Internal (intraperitoneal) | Paraduodenal, foramen of Winslow, mesenteric, transomental |
| Diaphragmatic | Hiatal, congenital (Bochdalek, Morgagni) |
| Pelvic | Obturator, sciatic, perineal |
| Lumbar (posterior) | Superior (Grynfeltt's triangle), inferior (Petit's triangle) |
Inguinal hernias account for ~75% of all abdominal wall hernias. The lifetime risk is 27% in men vs. 3% in women. Femoral, umbilical, epigastric, and incisional hernias account for most of the remainder.
— Yamada's Textbook of Gastroenterology
3.2 By Etiology
- Congenital — patent processus vaginalis (indirect inguinal), diaphragmatic (Bochdalek), umbilical
- Acquired — direct inguinal, incisional (up to 20% of laparotomy patients), most epigastric and femoral hernias
3.3 By Status of Contents (Clinical Urgency)
This is the most important classification for clinical management:
| Status | Definition | Clinical Features |
|---|---|---|
| Reducible | Hernia sac is soft; contents return spontaneously or with gentle manual pressure through the neck | Asymptomatic at rest; becomes apparent on standing/straining; cough impulse present |
| Irreducible (Incarcerated) | Contents cannot be returned by manipulation; hernia is firm and often painful | Not necessarily ischemic; may be chronic and minimally symptomatic |
| Strangulated | Vascular compromise (arterial, venous, or both) of incarcerated contents; can occur within 2 hours of incarceration | Severe pain, signs of bowel obstruction, toxic appearance, possible skin changes over sac — surgical emergency |
A Richter hernia is a special variant: only part of the bowel wall (not the full lumen) is incarcerated and strangulated, so complete bowel obstruction may be absent even with gangrenous bowel. Most often associated with femoral or inguinal hernias. — Mulholland & Greenfield's Surgery
3.4 By Direction (Groin Hernias)
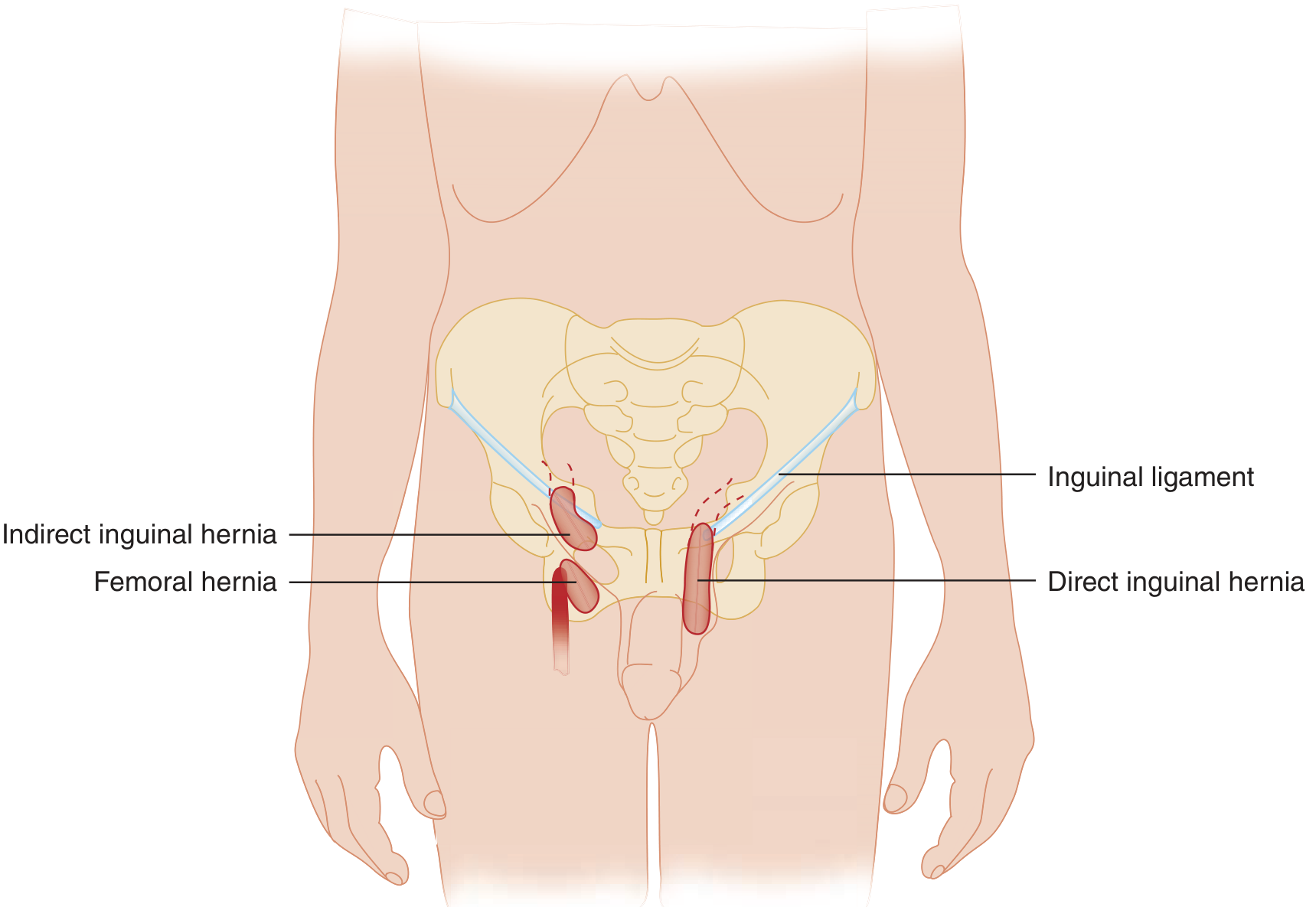
| Type | Anatomy |
|---|---|
| Indirect inguinal | Protrudes through the internal ring, lateral to the inferior epigastric vessels; lies within the spermatic cord; may descend into the scrotum; 2/3 of all inguinal hernias |
| Direct inguinal | Protrudes through the triangle of Hesselbach, medial to the inferior epigastric vessels; does not involve the cord; tends to protrude forward |
| Femoral | Protrudes through the femoral canal (bounded by inguinal ligament superiorly, lacunar ligament medially, Cooper's ligament inferiorly, femoral vein laterally); presents below the inguinal ligament |
| Sliding hernia | Part of the sac wall is formed by a viscus (left: sigmoid/bladder; right: cecum/bladder) |
| Pantaloon hernia | Simultaneous direct + indirect hernia straddling the inferior epigastric vessels |
3.5 By Recurrence Status
- Primary — first occurrence
- Recurrent — after previous repair (associated with much higher complication rates)
4. Formal Classification Systems
European Hernia Society (EHS) Groin Hernia Classification
Uses three variables:
- Location: L (lateral/indirect), M (medial/direct), F (femoral)
- Size: 0 (no defect), 1 (≤1 finger), 2 (1–2 fingers), 3 (≥3 fingers)
- Status: P (primary), R (recurrent), X (unknown)
Nyhus Classification of Groin Hernias (popular in the USA)
| Type | Description |
|---|---|
| I | Indirect; normal internal ring (infants, small adults) |
| II | Indirect; dilated internal ring; posterior wall intact; does not reach scrotum |
| IIIA | Direct; any size |
| IIIB | Indirect with dilated ring encroaching on Hesselbach triangle (massive, scrotal, sliding, or pantaloon) |
| IIIC | Femoral hernia |
| IVA–D | Recurrent: direct / indirect / femoral / combined |
EHS Ventral/Incisional Hernia Classification
Grid system based on: localization (midline vs. lateral), size of defect (width in cm), number of recurrences, and symptoms.
— Mulholland & Greenfield's Surgery; Sabiston Textbook of Surgery
5. Ventral / Abdominal Wall Hernias (Overview)
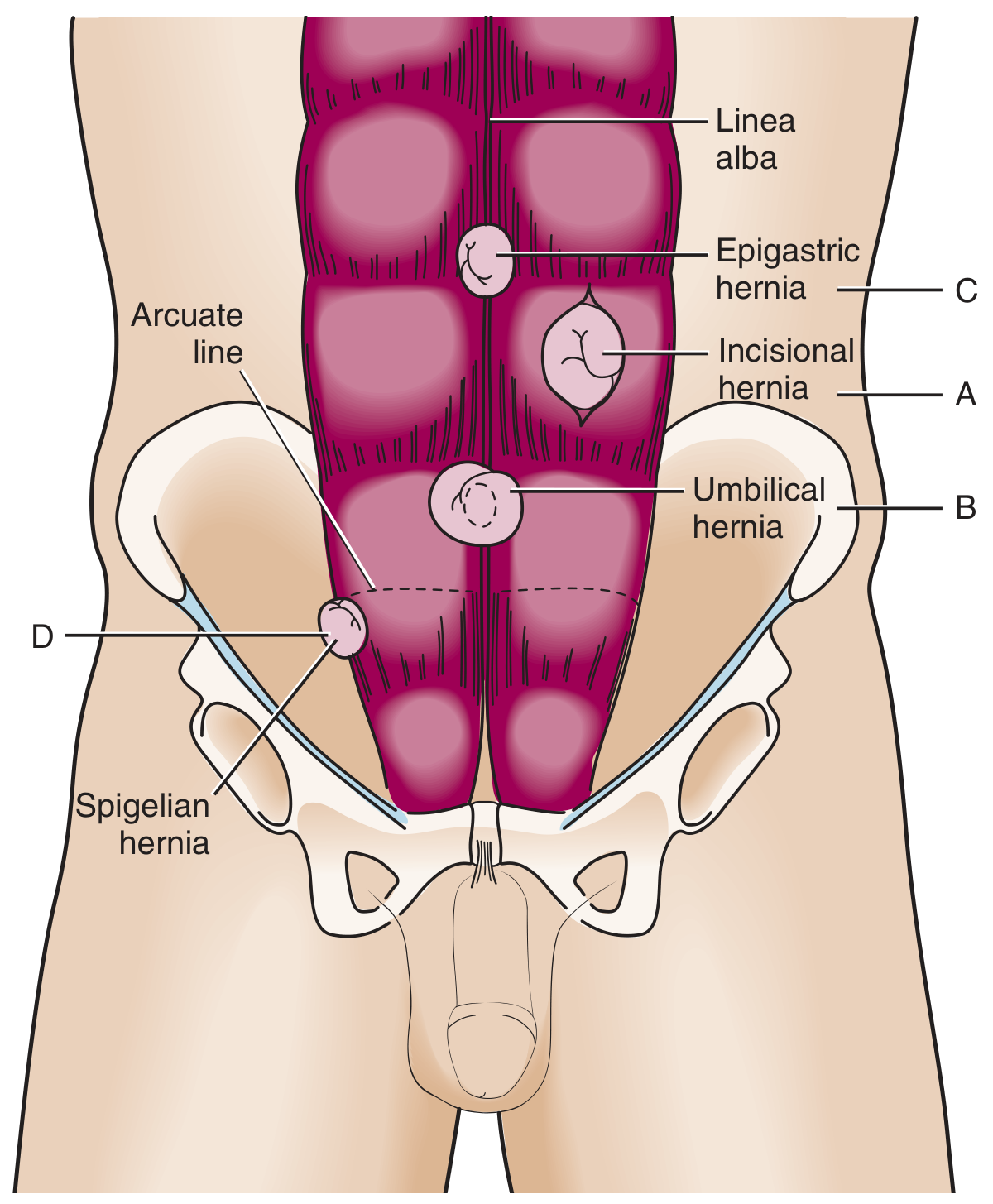
| Type | Location | Notes |
|---|---|---|
| Umbilical | Through the umbilical ring | Common in infants (often closes spontaneously); adults require repair |
| Epigastric | Midline through the linea alba, between xiphoid and umbilicus | Usually small, contains preperitoneal fat; found in 4% of pediatric hernia patients |
| Incisional | Through a previous surgical scar | Occurs in up to 20% of laparotomy patients; recurrence 20–50%; incarceration risk higher with smaller defects |
| Parastomal | Adjacent to a stoma opening | Very common complication of stoma formation |
6. Rare Forms of Hernia
Rare hernias together constitute less than 1% of all hernias (Schumpelick). The key ones are:
6.1 Spigelian (Lateral Ventral) Hernia
- Site: Defect in the Spigelian aponeurosis (membranous portions of internal oblique + transversus abdominis), at the lateral edge of the rectus muscle at the semilunar line, almost always at or below the arcuate line
- Key feature: The external oblique is intact, so the hernia is interparietal — the bulge is covered by an intact muscle layer and may be invisible on exam. This makes clinical diagnosis challenging.
- Incarceration risk: Up to 20% (often contains omentum); repair is recommended even when asymptomatic
- Diagnosis: Dynamic ultrasound or CT of abdomen/pelvis
- Demographics: Typically ages 40–70
6.2 Obturator Hernia
- Site: Through the obturator canal (contains obturator nerve, artery, vein); exits medial to the femoral vein into the medial upper thigh
- Epidemiology: < 1% of all hernias; predominantly affects elderly, thin females due to their triangular pelvis and atrophy of preperitoneal fat
- Risk factors: COPD, constipation, ascites (raised IAP)
- Pathognomonic sign: Howship–Romberg sign — pain in the anteromedial thigh, relieved by hip flexion (compression of the obturator nerve)
- Presentation: Bowel obstruction in up to 50%; can mimic femoral or inguinal hernia
- Strangulation morbidity: As high as 14% due to delayed diagnosis
- Diagnosis: CT scan preferred; ultrasound limited by the bony pelvis
6.3 Lumbar Hernia
- Site: Posterior abdominal wall, between the 12th rib and iliac crest, through one of two triangles:
- Superior lumbar (Grynfeltt's triangle): between the 12th rib and iliocostalis
- Inferior lumbar (Petit's triangle): between the iliac crest, latissimus dorsi, and external oblique
- Most cases are acquired (post-surgical, trauma, infection); primary spontaneous lumbar hernias are rare
- Diagnosis: CT of the abdomen/pelvis
6.4 Sciatic Hernia
- Site: Through the greater sciatic foramen; three subtypes based on their relationship to the piriformis muscle:
- Suprapiriformis (above piriformis)
- Infrapiriformis (below piriformis)
- Spinotuberous (in front of the sacrotuberous ligament)
- Extremely rare: Only ~99 patients in case reports from 1900–2008
- Presentation: Slowly enlarging gluteal mass, sciatic neuralgia, or acute bowel obstruction
- Repair: Minimally invasive (transabdominal) preferred; protect the obturator nerve/vessels and sciatic nerve; mesh sutured to Cooper's ligament
6.5 Perineal Hernia
- Site: Through the pelvic floor musculature; three types:
- Anterior perineal — in front of the deep transverse perineal muscle
- Posterior perineal — behind the deep transverse perineal
- Ischiorectal (ischioanal) — through the levator ani into the ischioanal fossa
- Often occurs after abdominoperineal resection or pelvic exenteration
6.6 Interparietal (Interstitial) Hernia
- Herniation between the layers of the abdominal wall (not through all layers)
- Most are incisional; Spigelian hernia is the classic primary interparietal hernia
- Frequently causes intestinal obstruction; CT essential
- Two forms relevant after complex ventral repairs: posterior rectus sheath herniation (after Rives–Stoppa), and semilunar line herniation (after transversus abdominis release)
6.7 Hernia Through the Foramen of Winslow (Epiploic Foramen)
- An internal hernia with abdominal viscera passing posterior to the porta hepatis into the lesser sac
- Usually diagnosed at laparotomy for bowel obstruction
Summary Table: Rare Hernias
| Hernia | Location | Key Distinguishing Feature |
|---|---|---|
| Spigelian | Semilunar line, at/below arcuate line | Interparietal; high incarceration risk; external oblique intact |
| Obturator | Obturator canal | Howship–Romberg sign; elderly thin women; bowel obstruction |
| Lumbar | Grynfeltt's or Petit's triangle (posterior wall) | Usually acquired/post-traumatic |
| Sciatic | Greater sciatic foramen | Gluteal mass ± sciatica; extremely rare |
| Perineal | Pelvic floor | Often post-pelvic surgery |
| Interparietal | Between abdominal wall layers | May present as obstruction without obvious external mass |
Sources: Mulholland & Greenfield's Surgery, 7e · Sabiston Textbook of Surgery · Tintinalli's Emergency Medicine · Yamada's Textbook of Gastroenterology, 7e · Roberts & Hedges' Clinical Procedures in Emergency Medicine · THIEME Atlas of Anatomy: General Anatomy and Musculoskeletal System
how to diagnose and treat
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I have comprehensive material. Here is the complete structured answer:
Hernia: Diagnosis and Treatment
PART I — DIAGNOSIS
1. History
A thorough history should document:
- Symptoms: Presence, onset, and nature of a groin/abdominal bulge; pain (especially with exertion, coughing, Valsalva); nausea, vomiting, or signs of bowel obstruction
- Eliciting factors: Heavy lifting, chronic cough, constipation, straining to urinate
- Prior repairs: Operative details, type of mesh, dates, infections — operative reports are invaluable for planning
- Risk factors: Smoking, COPD, obesity, collagen disorders, pregnancy, prior abdominal surgery
2. Physical Examination
The physical exam is the cornerstone of diagnosis and should be done standing and supine.
General maneuvers:
- Inspect for visible bulge or asymmetry with the patient standing and performing Valsalva
- Palpate the area at rest and during coughing/straining
- For males: invaginate the scrotal skin and pass a finger into the external inguinal ring — ask the patient to cough
- Impulse at the fingertip → indirect hernia
- Impulse at the dorsum/pulp → direct hernia
- Apply pressure over the mid-inguinal point (midway between ASIS and pubic tubercle): controlling an indirect hernia with this maneuver does not work for a direct hernia
Key distinctions at the groin:
| Feature | Indirect Inguinal | Direct Inguinal | Femoral |
|---|---|---|---|
| Position relative to inferior epigastric vessels | Lateral | Medial | Below inguinal ligament |
| Enters scrotum | Often | Rarely | Never |
| Controlled by pressure over internal ring | Yes | No | No |
| Risk of incarceration | Moderate | Low | Very high (up to 45%) |
Note: The accuracy of clinical differentiation between direct and indirect is only slightly better than chance; anatomical confirmation at surgery is definitive.
Red flag signs of strangulation (requiring emergency operation):
- Tender, warm, erythematous or discolored skin overlying the sac
- Fever, leukocytosis, hemodynamic instability
- Symptoms of bowel obstruction
3. Imaging
Imaging is not needed for obvious hernias. It is indicated when:
- Diagnosis is uncertain (occult hernia, obese patient)
- Differentiating recurrence from other causes of groin pain
- Preoperative planning for complex/recurrent hernias
| Modality | Sensitivity / Specificity | Role |
|---|---|---|
| Ultrasound (US) | Sens 86%, Spec 77% | First-line for occult/groin hernia; dynamic assessment with Valsalva; no radiation; operator-dependent |
| CT scan | Sens 80%, Spec 65% | Best for complex, atypical, or intraabdominal hernias (obturator, sciatic, lumbar); excludes other diagnoses |
| MRI | Sens 95%, Spec 96% | Most sensitive for occult hernias; useful when US inconclusive; identifies neuromas, mesh complications; expensive |
MRI demonstrates the highest sensitivity, specificity, and negative predictive value for occult hernias compared with US and CT, and has increased sensitivity for neuromas or issues with implanted mesh. — Current Surgical Therapy, 14e
4. Differential Diagnosis of Groin/Abdominal Swelling
- Lymphadenopathy
- Lipoma of the cord / femoral pseudohernia (prominent fat pad)
- Hydrocele (transilluminates; examining hand gets above it)
- Varicocele ("bag of worms"; does not transilluminate)
- Saphena varix (below inguinal ligament; obliterated by compression over femoral hiatus)
- Femoral artery aneurysm (pulsatile, expansile; bruit)
- Psoas abscess, hematoma, ascites
PART II — TREATMENT
Decision Framework
Hernia Confirmed
│
├── Strangulated? ──YES──► Emergency surgery (no taxis)
│
├── Incarcerated (no strangulation)? ──► Attempt TAXIS; then repair
│
├── Femoral / Symptomatic inguinal ──► Elective repair (early — femoral has
│ 22–45% strangulation risk at 2 years)
│
└── Asymptomatic / minimally symptomatic inguinal ──► Watchful waiting acceptable
A. Non-Operative Management
Watchful waiting is an appropriate strategy for asymptomatic or minimally symptomatic inguinal hernias in males. Prospective studies and meta-analyses show no difference in outcomes, quality of life, or cost-effectiveness compared to elective repair. However, 72% of initially asymptomatic patients develop symptoms and need surgery within 7.5 years.
Trusses confine the hernia and relieve symptoms in up to 65% of patients but do not prevent complications and may increase incarceration risk.
Femoral hernias should not be managed with watchful waiting — emergency operation carries a sevenfold increase in all-cause mortality over elective surgery (Swedish Hernia Registry, n = 107,838). — Schwartz's Principles of Surgery
B. Manual Reduction (Taxis)
Indication: Incarcerated hernia without signs of strangulation.
Technique:
- Administer analgesics and light sedation
- Place patient in Trendelenburg position (aids reduction by gravity)
- Elongate the hernia sac with both hands
- Apply gentle circumferential countertraction in a stepwise fashion to ease contents back into the abdomen
Taxis is contraindicated when strangulation is suspected — reducing gangrenous bowel into the abdomen causes intraabdominal catastrophe.
C. Surgical Repair — Principles
The universal principles regardless of hernia type:
- Reduce hernia contents
- Reapproximate the fascial defect
- Reinforce with mesh using wide overlap (≥3–5 cm) while preserving adjacent neurovascular structures
D. Inguinal Hernia Repair
Open Approaches
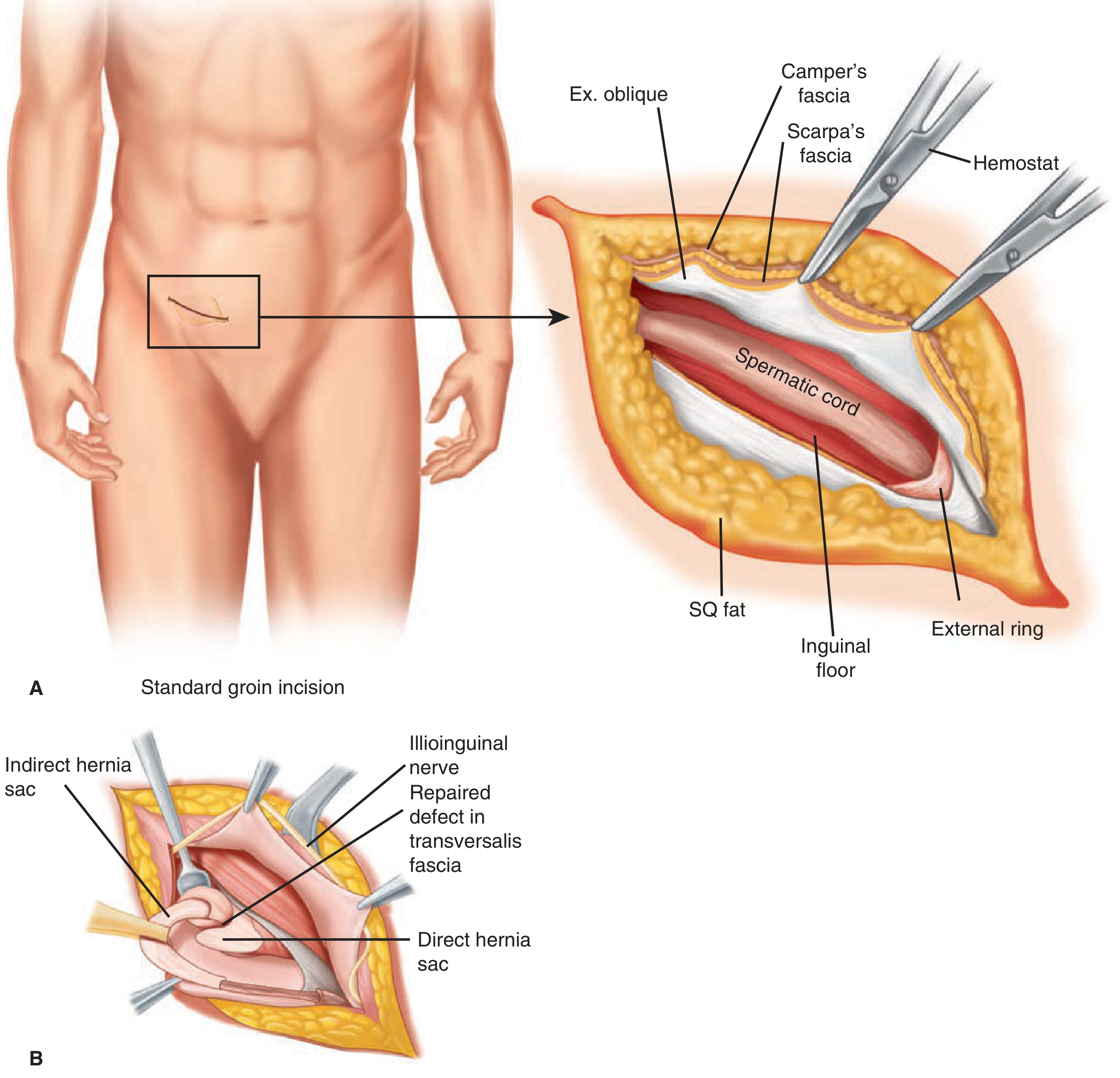
1. Tension-Free Mesh Repair (Lichtenstein — most common)
- Oblique/horizontal groin incision; Scarpa's fascia divided; external oblique aponeurosis opened
- Spermatic cord isolated; hernia sac identified and reduced
- A flat polypropylene mesh is sutured over the inguinal floor, covering the myopectineal orifice with wide overlap
- Standard of care for primary inguinal hernia repair in most centers
2. Tissue Repairs (reserved for infected fields, no mesh)
- Bassini: Approximation of the transversalis fascia, transversus abdominis, and internal oblique to the inguinal ligament
- Shouldice: Multi-layer running suture repair of the posterior inguinal wall; lowest recurrence among pure tissue repairs (~1%)
- Higher recurrence than mesh repairs; now used mainly when mesh is contraindicated
3. Open Preperitoneal Repairs (Stoppa, Kugel, Rives)
- Large mesh placed in the preperitoneal space via open approach; covers the entire myopectineal orifice
- Useful for bilateral, complex, or recurrent hernias
Laparoscopic/Minimally Invasive Approaches
| Technique | Description | Advantages | Notes |
|---|---|---|---|
| TAPP (Transabdominal Preperitoneal) | Laparoscopic; peritoneal cavity entered; preperitoneal space developed; large mesh placed | Excellent visualization; useful for bilateral hernias | Risk of intraperitoneal injuries |
| TEP (Totally Extraperitoneal) | Preperitoneal space entered without entering peritoneal cavity; balloon dissection | Avoids peritoneal entry; fewer adhesion complications | Steeper learning curve; CO₂ leak if peritoneum violated |
| IPOM (Intraperitoneal Onlay Mesh) | Mesh placed directly intraperitoneally over defect | Useful when preperitoneal scarring precludes TEP/TAPP | Mesh migration risk; nerve injury risk with tacking |
| Robot-assisted (rTAPP) | Endowrist dexterity improves intracorporeal suturing | Shorter learning curve than laparoscopic; better for complex/bilateral | Longer operative time, higher cost |
Laparoscopic vs. Open: RCTs and meta-analyses show laparoscopic repair has less initial pain, faster return to activity, lower wound infection and hematoma rates, and less chronic pain/numbness. Disadvantages: longer operative time, general anesthesia required, higher cost, risk of major vascular/bowel injury.
E. Femoral Hernia Repair
- High priority for repair due to high strangulation risk
- Approaches: anterior (via inguinal canal), low (directly below inguinal ligament), preperitoneal (best exposure for strangulated/recurrent cases)
- Mesh plugs or flat mesh placed in the femoral canal or over the myopectineal orifice
F. Ventral / Incisional Hernia Repair
Open Repair
- Primary suture repair: Only for small defects (<2 cm); high recurrence rate
- Mesh sublay (Rives-Stoppa): Mesh placed in the retromuscular (retrorectus) space posterior to the posterior rectus sheath — the current gold standard for open incisional hernia repair; wide mesh overlap in extraperitoneal plane
- Component separation (anterior CS): Release of the external oblique aponeurosis lateral to the linea semilunaris, allowing medial advancement of myofascial flaps to close large midline defects; used for complex, large, or recurrent hernias
- Transversus Abdominis Release (TAR / posterior CS): Division of the transversus abdominis muscle to access the retromuscular space; allows massive mesh overlap; particularly suited to recurrence after anterior CS
Laparoscopic Ventral Hernia Repair (LVHR)
- Greatest value: reduced wound complications due to small access incisions; applies "sublay" mesh technique without large open dissection
- Advantages: decreased blood loss, lower wound infection, shorter hospital stay
- Indications: high wound complication risk, small-to-moderate defects, multiple "swiss cheese" defects
- Contraindications: intolerance of pneumoperitoneum/GA, open wounds, extensive adhesions, large defects >10 cm
- Current trend: close the fascial defect during laparoscopic repair (not just "bridge" it) to prevent eventration/pseudorecurrence
G. Mesh Selection
| Type | Material | Use |
|---|---|---|
| Synthetic (polypropylene, polyester) | Permanent; promotes tissue ingrowth | Standard for most repairs |
| Lightweight mesh | Reduced fiber density; greater elasticity | Preferred — lower chronic pain (RR 0.61), equivalent recurrence |
| Biologic mesh | Derived from human/animal tissue | Reserved for contaminated fields or high infection risk; higher recurrence |
| Composite / barrier-coated | Synthetic + absorbable anti-adhesion layer | Intraperitoneal placement; prevents visceral adhesions |
Mesh should not be used in grossly infected fields unless biologic mesh is chosen. In resource-limited settings, sterilized polypropylene mosquito nets have demonstrated similar short-term complication and recurrence rates to commercial meshes.
H. Emergency Repair (Strangulated Hernia)
Pre-operative management:
- IV fluid resuscitation
- Nasogastric decompression
- IV prophylactic antibiotics
- Urgent theatre booking
Intraoperative:
- Reduce hernia contents and assess bowel viability
- Viable bowel → left in situ
- Non-viable bowel → resection + anastomosis or stoma
- In the context of contamination (necrotic bowel/spillage): avoid permanent synthetic mesh; use tissue repair or biologic mesh; two-stage approach may be necessary
I. Postoperative Complications to Anticipate
| Complication | Notes |
|---|---|
| Seroma | Most common; usually self-limiting; more common after laparoscopic repair |
| Wound infection / mesh infection | More common with heavyweight mesh; may require mesh removal |
| Chronic pain | Up to 10–12% after inguinal repair; related to nerve injury (ilioinguinal, iliohypogastric, genitofemoral); lightweight mesh and careful nerve identification reduce risk |
| Recurrence | Open non-mesh: 10–15%; open Lichtenstein: <2%; laparoscopic: 1–5%; incisional hernia: 20–50% without mesh, <10% with proper mesh sublay |
| Vascular injury | Rare; most serious laparoscopic complication; distal aorta, iliac vessels at risk |
| Testicular ischemia / atrophy | Injury to testicular blood supply during extensive sac dissection |
Sources: Schwartz's Principles of Surgery, 11e · Mulholland & Greenfield's Surgery, 7e · Sabiston Textbook of Surgery · Current Surgical Therapy, 14e · Tintinalli's Emergency Medicine · Yamada's Textbook of Gastroenterology, 7e
causes
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
I now have all the material needed. Here is the comprehensive answer on causes:
Causes of Hernia
Hernia formation is multifactorial — it requires the combination of a structural weakness or defect in the containing wall and a force driving contents through that defect. Current evidence points to both environmental and hereditary influences.
I. Fundamental Mechanism
Two conditions must coexist:
| Condition | Examples |
|---|---|
| Weakness / defect in the wall | Congenital gap (patent processus vaginalis), aging, prior surgery, collagen disorder |
| Force pushing contents through | Raised intraabdominal pressure from coughing, straining, lifting, obesity, ascites |
"Especially where the connective tissue is weakened, as occurs in elderly persons, it occasionally fails to resist intra-abdominal pressure and becomes a site of hernia. Triggering events include lifting heavy objects or even coughing." — THIEME Atlas of Anatomy: General Anatomy and Musculoskeletal System
II. Congenital Causes
1. Patent Processus Vaginalis (PPV) — most important congenital cause
During normal fetal development, the testes descend from the intra-abdominal space into the scrotum in the 3rd trimester, guided by the gubernaculum through an evagination of peritoneum called the processus vaginalis. Normally, the processus vaginalis closes between 36–40 weeks' gestation, eliminating the peritoneal opening at the internal inguinal ring.
Failure of closure = patent processus vaginalis → indirect inguinal hernia or hydrocele
- In preterm infants, the processus is almost always patent → very high incidence of indirect inguinal hernia (up to 30% of premature neonates)
- In full-term infants, ~5% have an inguinal hernia
- In children and young adults, most hernias are indirect inguinal hernias of congenital origin
- The overall risk of developing a symptomatic hernia in the presence of a known PPV during childhood is relatively low — many PPVs close spontaneously
In females: The processus vaginalis accompanies the round ligament through the canal; failure to close creates the canal of Nuck → predisposes to indirect inguinal hernia in women.
2. Other Congenital Defects
- Umbilical hernia in infants — failure of the umbilical ring to close after birth; most close spontaneously by age 4–5
- Congenital diaphragmatic hernia (Bochdalek, Morgagni) — failure of diaphragm development/closure
- Omphalocele / gastroschisis — failure of normal abdominal wall formation in embryonic development
- Naturally weak anatomical points in the abdominal wall where muscle is absent and only connective tissue spans the gap (inguinal canal, femoral canal, umbilical ring, obturator foramen) — these are pre-formed sites of vulnerability
III. Acquired Causes
A. Increased Intraabdominal Pressure (IAP)
Any chronic or repetitive force that pushes against the abdominal wall can drive herniation through an existing weak point:
| Cause | Mechanism |
|---|---|
| Chronic cough / COPD | Repeated Valsalva; COPD significantly increases risk of direct inguinal hernia specifically due to repeated pressure spikes |
| Constipation / straining at stool | Prolonged elevated IAP |
| Prostatism / bladder outlet obstruction | Straining to urinate |
| Obesity | Chronically elevated baseline IAP (paradoxically, obesity may make inguinal hernias harder to detect; obese men have ~50% the risk of lean men — possibly a detection bias) |
| Ascites | Fluid pressure directly distends the abdominal wall |
| Pregnancy | Hormonal laxity + mechanical pressure; also weakens abdominal wall |
| Heavy lifting / physical exertion | Acute spikes in IAP |
| Peritoneal dialysis | Continuous fluid infusion into peritoneal cavity → elevated IAP |
| Low birthweight (<1500 g) | Prematurity = high rate of PPV |
B. Connective Tissue / Collagen Disorders
This is the biochemical core of acquired hernia formation:
- Microscopic examination of skin from inguinal hernia patients shows significantly decreased ratios of type I : type III collagen
- Type I collagen = major structural tensile-strength collagen
- Type III collagen = weaker, more distensible — does not contribute to tensile strength as significantly
- Disaggregated collagen tracts with decreased fiber density are found in hernia tissue
- Matrix metalloproteinase (MMP) dysregulation: elevated concentrations of extracellular matrix elements and altered MMP activity impair structural integrity of fascial tissues
- This explains why hernias can occur even without obvious mechanical triggers
Connective tissue disorders associated with hernia formation:
| Disorder | Notes |
|---|---|
| Ehlers-Danlos syndrome | Defective collagen cross-linking; very high hernia incidence |
| Marfan syndrome | Fibrillin-1 defect; associated with inguinal and hiatal hernia |
| Osteogenesis imperfecta | Type I collagen mutation |
| Cutis laxa (congenital elastolysis) | Elastin defect |
| α₁-Antitrypsin deficiency | Protease-antiprotease imbalance damages fascial matrix |
| Hurler-Hunter syndrome | Mucopolysaccharide storage disorder |
| Polycystic kidney disease | Often associated with inguinal hernia |
| Androgen insensitivity syndrome | Associated with inguinal hernia (undescended testis) |
| Marfan, Williams, Alport, Kawasaki, Menkes' syndrome | Various connective tissue defects |
A positive family history confers an eightfold lifetime incidence of inguinal hernia. — Schwartz's Principles of Surgery
C. Cigarette Smoking
- Tobacco smoke inhibits α₁-antitrypsin, increases systemic protease activity, and impairs collagen synthesis and cross-linking
- Associated with both inguinal hernia formation and poor wound healing → higher incisional hernia rates
D. Age and Loss of Tissue Elasticity
- Advancing age causes progressive loss of tissue elasticity and collagen quality
- Muscle atrophy and thinning of fascial layers
- Direct inguinal hernias are overwhelmingly acquired and increase markedly with age
- Obturator hernias preferentially affect elderly, thin women (loss of preperitoneal fat protecting the obturator canal)
E. Sex
- Male sex is the dominant risk factor for inguinal hernia (male : female ratio = 7.5–10 : 1)
- Men have a 25–27% lifetime risk; women 3–5%
- The inguinal canal in males is larger and has the spermatic cord passing through it — inherent weakness
- Female sex is a risk factor for femoral hernia (though inguinal hernia is still more common even in women)
F. Prior Surgery (Incisional Hernia)
Incisional hernias occur in up to 20% of patients after abdominal surgery. Causes are multifactorial:
| Factor | Mechanism |
|---|---|
| Wound infection | Bacterial collagenases degrade sutured fascia before healing; most potent single risk factor |
| Obesity | Poor fascial blood supply, increased tension, poor healing |
| Malnutrition / hypoalbuminaemia | Impaired collagen synthesis |
| Diabetes mellitus | Impaired wound healing, microvascular disease |
| Immunosuppression / corticosteroids | Suppress collagen synthesis and inflammatory healing response |
| Chemotherapy / radiotherapy | Impairs tissue healing |
| Technical factors | Excessive tension on closure, use of absorbable suture for fascial closure, small bites, missed fascial layers |
| Midline incision | More prone to hernia than transverse or off-midline incisions (EHS recommends off-midline where possible) |
| Emergency surgery | Associated with higher contamination and wound complications |
G. Trauma
- Blunt or penetrating abdominal injury can create fascial defects → traumatic hernia
- Also includes sports hernias (athletic pubalgia) — disruption of the posterior inguinal wall from repetitive strain without a true peritoneal sac
H. Neurological / Muscular Disease
- Conditions causing denervation or paresis of the abdominal wall musculature (e.g., post-polio, spinal cord injury) leave the abdominal wall unsupported → hernia at weak anatomical points
IV. Cause Summary by Hernia Type
| Hernia Type | Primary Cause(s) |
|---|---|
| Indirect inguinal | Patent processus vaginalis (congenital); also acquired with IAP + collagen defects |
| Direct inguinal | Acquired; weakness of the posterior inguinal wall (transversalis fascia); age, COPD, smoking, collagen deficiency |
| Femoral | Acquired; widening of the femoral ring; female sex, age, thin body habitus, pregnancy |
| Umbilical (infant) | Congenital failure of umbilical ring closure |
| Umbilical (adult) | Acquired; raised IAP (obesity, ascites, pregnancy, CAPD) against a naturally weak ring |
| Incisional | Prior surgery; wound infection, obesity, poor technique, diabetes, steroids |
| Epigastric | Acquired; small defects in the linea alba through which preperitoneal fat protrudes |
| Spigelian | Acquired; weakness at the semilunar line at/below arcuate line; prior incisions |
| Obturator | Acquired; loss of preperitoneal fat in obturator canal; elderly thin women; raised IAP |
| Hiatal | Acquired; weakening of the phrenoesophageal ligament; obesity, age, raised IAP |
| Congenital diaphragmatic | Congenital failure of diaphragm formation (pleuroperitoneal fold) |
| Lumbar | Acquired; post-surgical (flank/kidney incision), trauma, infection, retroperitoneal inflammation |
Sources: Schwartz's Principles of Surgery, 11e · Mulholland & Greenfield's Surgery, 7e · Roberts & Hedges' Clinical Procedures in Emergency Medicine · THIEME Atlas of Anatomy: General Anatomy and Musculoskeletal System · Yamada's Textbook of Gastroenterology, 7e
This is a shared conversation. Sign in to Orris to start your own chat.