Panophthalmitis
Reading File
Finding Sources
Searching PubMed
panophthalmitis management treatment
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Here is a detailed account of panophthalmitis based on authoritative textbook sources:
Panophthalmitis
Definition
Panophthalmitis is inflammation of the entire globe - involving the retina, choroid, and sclera - that extends beyond the confines of the eye into the orbit. This distinguishes it from endophthalmitis, which is limited to the interior of the eye (vitreous humor and adjacent structures). When the infection breaches the sclera and involves periorbital tissues, the diagnosis becomes panophthalmitis.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 1216
Pathology
The gross pathological appearance is dramatic: suppurative inflammation distorts the entire architecture of the eye. The image below (Fig. 29.16, Robbins) shows an enucleated globe following a foreign body injury - the entire intraocular architecture is destroyed by suppurative inflammation:
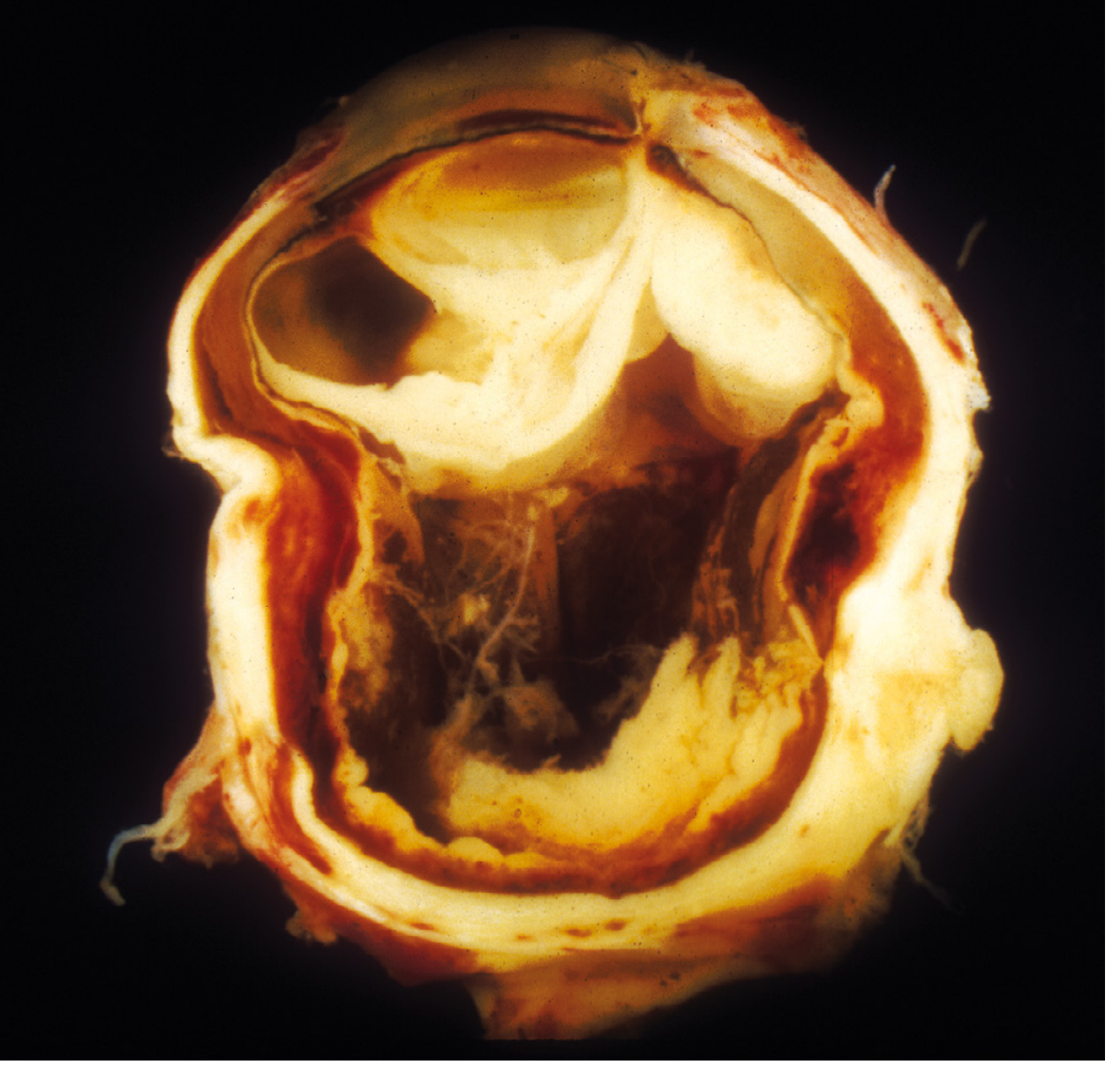
Fig. 29.16 - Exogenous panophthalmitis. The eye was removed after a foreign body injury. Suppurative inflammation of the entire orbit has distorted the architecture of the eye. (Robbins Pathology)
The retina is particularly vulnerable - only a few hours of suppurative inflammation in the vitreous cavity can cause irreversible retinal injury. In panophthalmitis, this process has spread through all coats of the globe.
Classification / Etiology
Panophthalmitis arises from the same routes as endophthalmitis:
| Type | Source |
|---|---|
| Exogenous | Foreign body injury, penetrating trauma, post-surgical wound infection |
| Endogenous | Hematogenous spread from systemic sepsis (bacteremia, fungemia) |
| Extension | Direct spread from adjacent orbital or periorbital structures (ethmoiditis, dacryocystitis, dacryoadenitis, orbital cellulitis) |
Causative Organisms
Bacterial (most common):
- Bacillus cereus (especially in i.v. drug users - extremely virulent)
- Streptococcus species
- Staphylococcus aureus
- Klebsiella (particularly in East Asia)
- Neisseria meningitidis
- H. influenzae
- Anaerobes (Bacteroides, Fusobacterium - in orbital extension from sinus/dental sources)
Fungal:
- Candida species (immunocompromised, i.v. drug users, indwelling catheters)
- Aspergillus species
Clinical Features
Symptoms
- Severe pain, marked reduction in vision
- Presentation in context of systemic illness (sepsis, i.v. drug use, recent surgery, immunocompromise)
Signs
Critical:
- Chorioretinitis
- Vitreous cells and debris
- Anterior chamber cell, flare, and hypopyon
- Absent red reflex
Other (indicating progression toward / established panophthalmitis):
- Iris microabscesses
- Retinal inflammatory infiltrates; flame-shaped hemorrhages with or without white centers
- Retinal / subretinal / choroidal abscesses
- Corneal edema
- Eyelid edema and chemosis
- Conjunctival injection
- Proptosis and restricted ocular motility - hallmarks of orbital involvement that define panophthalmitis
The condition may be bilateral in cases of hematogenous spread.
- Wills Eye Manual, §12.16
Workup
- History - duration, systemic illness, indwelling catheter, i.v. drug use, immunosuppression, recent medical procedures
- Complete ocular exam including dilated fundus evaluation
- B-scan ultrasound if fundus view is obscured - assesses for vitritis and abscesses
- Complete medical workup with an infectious disease specialist
- Chest X-ray and cultures of blood, urine, all indwelling catheters and i.v. lines; Gram stain of any discharge
- Transesophageal/transthoracic echocardiogram to rule out endocarditis
- Lumbar puncture if meningitis or CNS involvement is suspected
- Orbital imaging (CT/MRI) if orbital cellulitis or abscess is suspected
Treatment
Management must be coordinated with internal medicine/infectious disease.
1. Hospitalization
Mandatory - this is an ocular emergency.
2. Systemic Antibiotics (IV)
- Broad-spectrum IV antibiotics started after cultures obtained
- Dosed at meningitis/severe infection levels (for CNS/vitreous penetration)
- Tailored to suspected source (GI, GU, cardiac) and culture sensitivity
- IV drug users: aminoglycoside + clindamycin (to cover Bacillus cereus)
- IV antibiotics maintained for at least 2 weeks
3. Intravitreal Antibiotics
Considered when vitreous involvement is significant or worsening:
- Vancomycin 1 mg/0.1 mL (gram-positive cover)
- Ceftazidime 2.25 mg/0.1 mL (gram-negative cover)
- Clindamycin 1 mg/0.1 mL or amikacin 0.4 mg/0.1 mL for anaerobic/Bacillus cover
- Caution: intravitreal aminoglycosides (including amikacin) can cause macular infarction
4. Topical Therapy
- Cycloplegic (e.g., atropine 1% b.i.d.-t.i.d.) for pain and to prevent synechiae
- Topical steroid (e.g., prednisolone acetate 1% q1-6h) for anterior segment inflammation
5. Periocular Antibiotics
Subconjunctival or sub-Tenon injections may be used as adjuncts.
6. Pars Plana Vitrectomy (PPV)
Considered if severe or non-responsive to initial therapy. Benefits:
- Reduces infective and inflammatory load
- Provides material for diagnostic culture and pathology
- Intravitreal antibiotics can be given concurrently
7. Surgical - Evisceration / Enucleation
In panophthalmitis with complete destruction of the globe and no useful vision, evisceration (removal of intraocular contents) or enucleation (removal of entire globe) may be necessary, especially to prevent:
- Intracranial extension (meningitis, cavernous sinus thrombosis)
- Sympathetic ophthalmia in the fellow eye (a consideration in penetrating trauma cases)
Complications
- Blindness (nearly inevitable in established panophthalmitis)
- Orbital cellulitis / abscess
- Cavernous sinus thrombosis
- Meningitis (direct intracranial extension)
- Septicemia / septic shock
- Loss of the globe (requiring enucleation)
Prognosis
Visual prognosis is extremely poor - most eyes with panophthalmitis suffer permanent blindness. The goal of treatment shifts from vision preservation to control of systemic infection and prevention of life-threatening complications.
Sources:
- Robbins, Cotran & Kumar Pathologic Basis of Disease (p. 1216) - definition and pathology
- Wills Eye Manual, §12.16 (Endogenous Bacterial Endophthalmitis) - clinical features, workup, and treatment
- Tintinalli's Emergency Medicine - orbital cellulitis complications including panophthalmitis
This is a shared conversation. Sign in to Orris to start your own chat.