Chopart injuries etiology causes mechanism of injury associated injury signs and symptoms investigation and treatment explain in detail with appropriate illustrative diagrams and images
Reading File
Finding Sources
Finding Sources
Searching the Web
Chopart joint injury mechanism treatment anatomy radiology 2024
Searching PubMed
Chopart joint injury treatment outcome
Reading File
Reading File
Reading File
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC10774188
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Reading Web Page
https://surgeryreference.aofoundation.org/orthopedic-trauma/…
Loading Image
Loading Image
I now have comprehensive data from multiple authoritative sources. Let me compile the full, detailed answer.
Chopart Joint Injuries - Comprehensive Overview
1. Anatomy and Named Structure
The Chopart joint (also called the transverse tarsal joint or midtarsal joint) is named after French surgeon François Chopart (1743-1795), who described a transmetatarsal amputation through this articulation. It forms the functional boundary between the hindfoot and midfoot.
Constituent Joints
The Chopart joint complex consists of two anatomically and functionally linked joints that act in synchrony:
| Joint | Articulation | Function |
|---|---|---|
| Talonavicular joint (TNJ) | Head of talus - navicular | Part of the coxa pedis; enables pronation/supination of the tarsus |
| Calcaneocuboid joint (CCJ) | Anterior calcaneus - cuboid | ~25° of rotation for hindfoot eversion/inversion |
Together they allow the forefoot to remain flat on the ground while the hindfoot inverts or everts, and they lock during push-off in the gait cycle, stabilizing the midfoot.
Key Ligamentous Supports
| Ligament | Location | Significance |
|---|---|---|
| Bifurcate ligament | Anterior process calcaneus → navicular and cuboid (Y-shape) | Most commonly injured; avulsion fractures of anterior calcaneal process |
| Dorsal talonavicular ligament | Dorsal talus → navicular | Torn in dorsal distraction injuries |
| Dorsal calcaneocuboid ligament | Calcaneus → cuboid dorsally | Torn in inversion injuries |
| Spring ligament (plantar calcaneonavicular) | Sustentaculum tali → navicular | Supports talar head; injury in medial distraction |
| Long plantar ligament | Calcaneus → cuboid/metatarsal bases | Secondary stabilizer of lateral column |
| Short plantar ligament (plantar calcaneocuboid) | Calcaneus → cuboid | Direct support of CCJ |
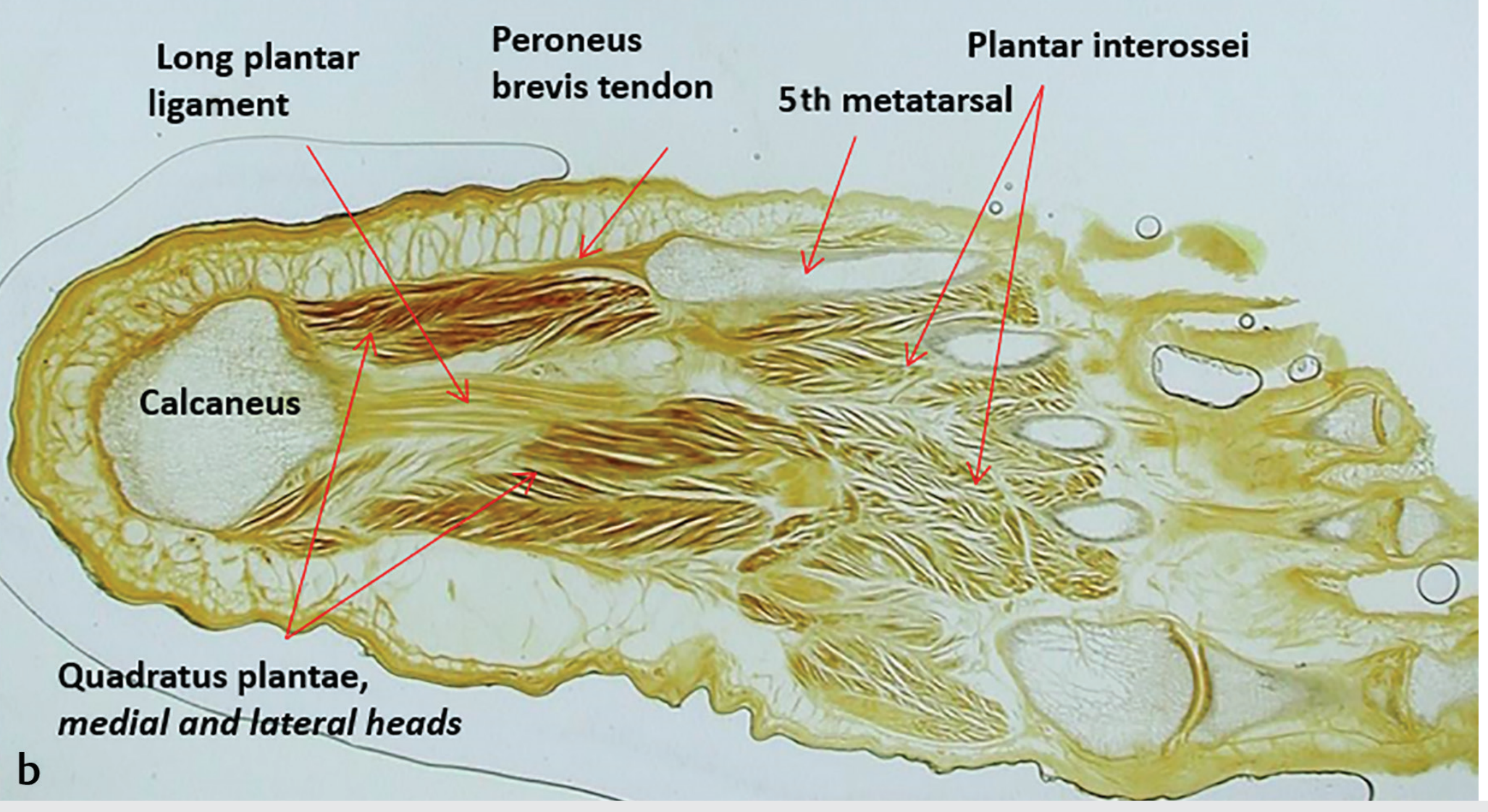
Fig. 22.87 - Inferior view of foot dissection showing the long plantar ligament (arrows). Ca = calcaneus. (Imaging Anatomy Text and Atlas, Vol. 3)
2. Epidemiology and Etiology
Chopart joint injuries are uncommon but frequently missed. Key statistics:
- Midfoot fractures occur at an estimated 3.6/100,000/year (Court-Brown et al.)
- Chopart injuries occur 4x less frequently than Lisfranc injuries
- In a review of 155 midfoot fractures/dislocations, pure Chopart fracture-dislocations accounted for 16%, Chopart-Lisfranc combined for 16.8%
- Misdiagnosis rate is 20-41% - symptoms are frequently attributed to ankle sprain
- The incidence has risen with motor vehicle airbag use (patients who previously would not have survived now sustain severe blunt foot trauma)
Causes / Etiological Factors
- Falls (stairs, height) - most common low-energy cause
- Sports injuries - particularly football, equestrian, skiing
- Motor vehicle accidents (MVA) - high-energy; associated with severe fracture-dislocations
- Pedestrian vs. vehicle accidents - high energy
- Axial loading injuries (e.g., fall from height, landing on plantar-flexed foot)
- Twisting injuries with or without inversion/eversion component
3. Mechanism of Injury
The mechanism determines which structures are injured and in which pattern. Two key classification systems describe this:
Main and Jowett Classification (1975)
Based on direction and magnitude of force:
| Type | Mechanism | Structures Injured |
|---|---|---|
| Medial stress | Adduction/inversion force | Lateral ligaments stretched; medial compression fractures of talar head/navicular |
| Longitudinal stress | Axial compressive force through foot | Comminuted fractures of navicular/cuboid |
| Lateral stress | Abduction/eversion force | Medial ligament disruption; lateral compression fractures |
| Plantar stress | Plantar flexion force | Dorsal capsule/ligament disruption |
| Crush | Direct trauma | Multiple fractures; soft tissue injury |
Inversion Injuries (Most Common ~75%)
The most frequent mechanism involves forced inversion, often with simultaneous plantar flexion. This creates:
- Lateral distraction - avulsion of bifurcate ligament, dorsal calcaneocuboid ligament, extensor digitorum brevis origin; may produce anterior calcaneal process fracture
- Medial compression - impaction of talar head and navicular body
- When accompanied by plantar flexion: distraction propagates dorsally through the talonavicular joint → dorsal talonavicular ligament tear or dorsal navicular avulsion
Eversion/Abduction Injuries (Less Common)
- "Nutcracker" mechanism at the calcaneocuboid joint
- Compressive impaction on lateral side → comminuted anterior calcaneus and posterolateral cuboid fractures (often depressed)
- Medial distraction → navicular tuberosity avulsion (tibialis posterior traction), spring ligament injury
High-Energy Injuries
- MVA / crush: Complete fracture-dislocation of both TNJ and CCJ (complete Chopart dislocation)
- Swivel dislocations: Medial or lateral deforming forces causing TNJ and/or CCJ dislocation while the calcaneus rotates around the talus
4. Classification of Chopart Injuries
Chopart injuries span a spectrum from subtle sprains to complete fracture-dislocations:
Spectrum of Injury
GRADE 1 - Sprain/Ligament injury (no dislocation)
GRADE 2 - Ligament injury WITH dislocation (pure dislocation)
GRADE 3 - Fracture WITHOUT dislocation
GRADE 4 - Fracture WITH dislocation (fracture-dislocation)
By Direction (Clinical Classification)
| Category | Description |
|---|---|
| Pure dislocation | Navicular and/or cuboid dislocation without fracture |
| Fracture-dislocation | Dislocation + fracture of talus, navicular, calcaneus, or cuboid |
| Complete Chopart dislocation | Simultaneous TNJ + CCJ dislocation |
| Swivel dislocation | Calcaneus rotates around talus; partial dislocation |
| Nutcracker fracture | Cuboid compression fracture from lateral column impaction |
5. Associated Injuries
Given the high-energy mechanisms involved, Chopart injuries are rarely isolated:
Local Associated Injuries
- Lisfranc joint injuries (most common co-injury; combined Chopart-Lisfranc has worst prognosis)
- Navicular fractures (body, tuberosity, stress fractures)
- Cuboid fractures (avulsion or nutcracker compression type)
- Anterior calcaneal process fractures (bifurcate ligament avulsion)
- Talar head fractures (impaction from navicular in medial stress)
- Cuneiform fractures (rare in isolation)
- Subtalar joint injuries (in high-energy mechanisms)
- Compartment syndrome of the foot (must be ruled out in all significant injuries)
Systemic/Regional Associated Injuries (High-Energy)
- Calcaneal fractures
- Tibial/fibular fractures (pilon fracture)
- Knee injuries (dashboard mechanism)
- Pelvic fractures
- Neurovascular injury (peroneal nerve, dorsalis pedis artery)
- Open wounds and soft tissue degloving
6. Signs and Symptoms
Chopart injuries are notoriously under-diagnosed because they mimic ankle sprains.
History
- Mechanism: twisting of foot, fall, MVA
- Inability or difficulty weight-bearing
- Onset of midfoot/dorsal foot pain
Clinical Examination
| Sign/Symptom | Description |
|---|---|
| Pain | Over the midfoot, dorsal aspect at the level of the Chopart joint |
| Swelling | Dorsal midfoot swelling (may be delayed) |
| Tenderness | Point tenderness over the talonavicular joint medially and calcaneocuboid joint laterally |
| Inability to weight-bear | Common in moderate-severe injuries |
| Plantar ecchymosis sign (PES) | Bruising on the sole of the foot - originally described for Lisfranc but applicable here; high specificity for midfoot injury |
| Deformity | Obvious in displaced fracture-dislocations; may be subtle in sprain |
| Abnormal ROM | Pain on passive inversion/eversion, dorsiflexion/plantarflexion |
| Ankle appearance | Ankle may appear normal, leading to misdiagnosis as ankle sprain |
Red Flags Requiring Urgent Assessment
- Tense compartments (pain out of proportion, pain with passive stretch of toes)
- Neurovascular compromise (pallor, absent pulses, paraesthesia)
- Open fracture
7. Investigations
Plain Radiography (First-Line)
Three standard views of the foot (not the ankle):
- Dorsoplantar (AP) view
- Lateral view
- Oblique view
Radiographs are often normal or show only subtle findings - the diagnosis is frequently missed.
Key radiographic signs:
- Loss of parallelism at the talonavicular or calcaneocuboid joint
- Fleck avulsion fractures at ligament attachment sites
- Anterior calcaneal process fracture
- Navicular tuberosity avulsion
- Cuboid compression/avulsion
- Joint space widening

Fig. 93.67 - Cuboid fracture invisible on plain X-ray (A, B), revealed on CT scan (C, D), after ORIF with screw fixation (E, F). (Campbell's Operative Orthopaedics 15th Ed, 2026)
Computed Tomography (CT) - Gold Standard for Bony Injury
Indications:
- Any clinically suspected Chopart injury even with normal X-rays
- All confirmed injuries for surgical planning
- Assessment of comminution, articular involvement, and column length
CT findings:
- Subtle articular fractures invisible on plain X-ray
- Degree of comminution and displacement
- Associated injuries to adjacent bones
- 3D reconstruction for surgical planning
MRI - Gold Standard for Ligamentous Injury
Indications:
- Suspected purely ligamentous injury (normal CT)
- Assessment of spring ligament, bifurcate ligament, plantar fascia
- Chronic instability evaluation
- Differentiating sprain from occult fracture
MRI patterns (Radsource classification):
- Lateral distraction / medial compression (inversion)
- Dorsal distraction (plantar flexion + inversion)
- Medial distraction / lateral compression (eversion/"nutcracker")
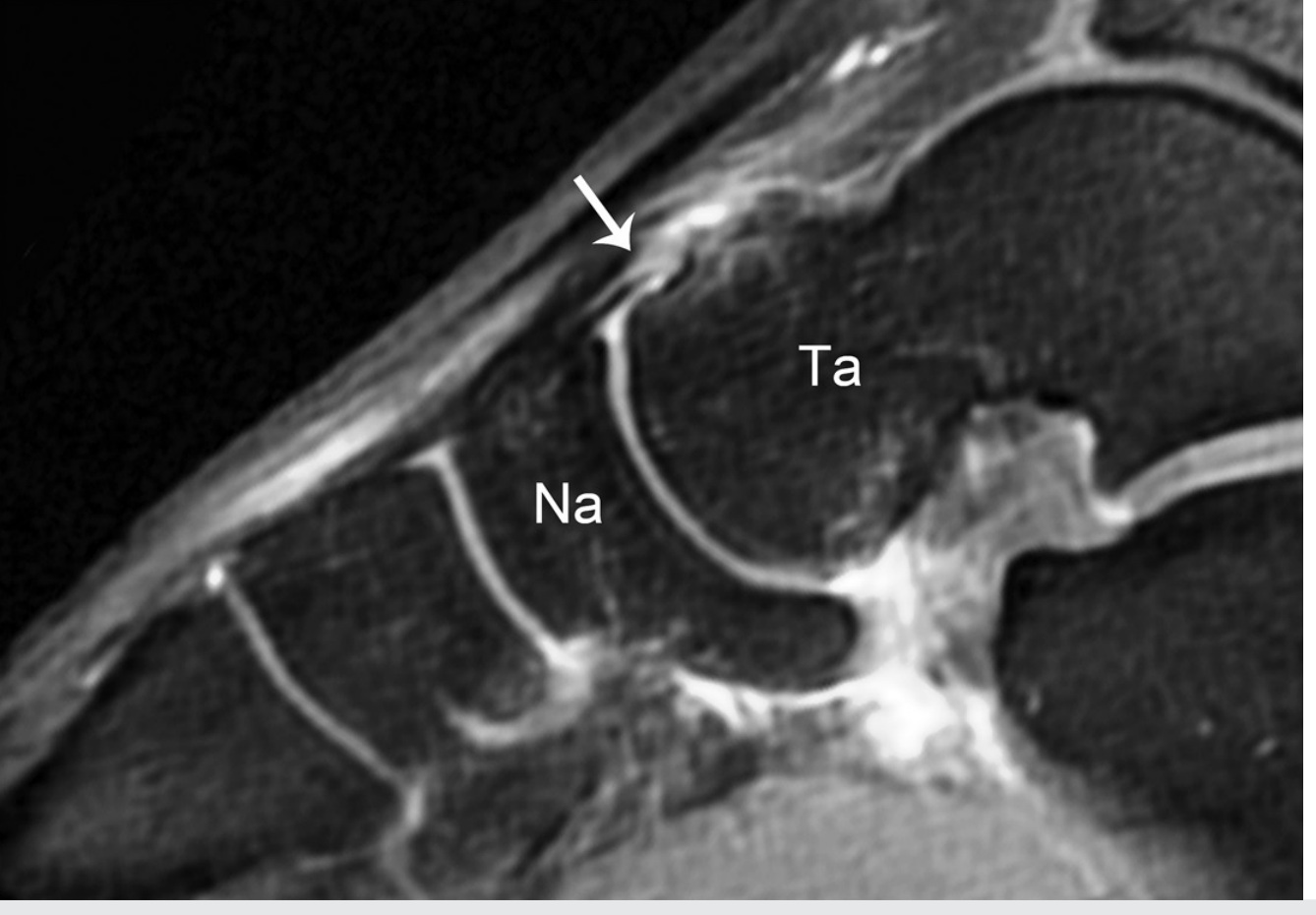
Fig. 22.88 - Sagittal MRI showing tear of the dorsal talonavicular ligament (arrow). Na = navicular, Ta = talus. (Imaging Anatomy Text and Atlas, Vol. 3)
Bone Scan / SPECT
- Useful for detecting occult fractures (navicular stress fractures)
- Less commonly used with widespread CT/MRI availability
8. Treatment
General Principles
The goals of treatment are:
- Anatomic reduction of the Chopart joint
- Restoration and maintenance of column length (medial and lateral)
- Stable fixation until healing
- Prevention of post-traumatic arthritis and flatfoot deformity
Early operative intervention with anatomic alignment gives the best outcomes. The lowest-scoring results occur in patients with combined Chopart + Lisfranc fracture-dislocations.
Non-Operative Treatment
Indications:
- Isolated ligamentous sprain (Grade 1-2) without instability or dislocation
- Nondisplaced avulsion fractures
- Nondisplaced navicular/cuboid fractures
Protocol:
- RICE (rest, ice, compression, elevation) initially
- Non-weight-bearing in a below-knee (BK) cast for 6-8 weeks
- Controlled motion walking boot or aircast splint
- Progressive weight-bearing with soft brace for 6 further weeks
- Outpatient orthopedic follow-up within 48 hours for non-operative injuries
Note: More aggressive immobilization (6-8 weeks SLC rather than walking boot) is recommended compared to ankle sprains, as Chopart sprains can lead to significant chronic instability.
Operative Treatment
Indications:
- Displaced fractures
- Any dislocation (pure or fracture-dislocation)
- Instability after reduction
- Failed closed reduction
- Open fractures
Step 1: Closed Reduction (Attempt First)
Under general or regional anesthesia:
- Apply manual traction in the axial vector
- Reverse the mechanism of injury (e.g., eversion for an inversion dislocation)
- Assess under fluoroscopy
If closed reduction fails → open reduction required (due to bone interposition, soft tissue interposition, or both)
Step 2: Patient Positioning
- Supine, knee flexed 90°
- Tourniquet applied to thigh
Step 3: Surgical Approaches
Medial approach: Dorsomedial incision - for talonavicular joint, navicular, talar head
Lateral (anterolateral) approach: Anterolateral incision - for calcaneocuboid joint, cuboid, anterior calcaneus
For complete Chopart dislocations: Combination of both approaches (described as a combination of the subtalar dislocation approach with anterolateral + dorsomedial incisions)
Step 4: Fracture Fixation
| Injury Type | Fixation Method |
|---|---|
| Simple navicular fracture | Lag screw fixation |
| Multifragmentary navicular | ORIF with plate, or fusion (naviculocuneiform), or bridging |
| Unreconstructable talonavicular joint | Bridging (NOT fusion - preserve hindfoot circumduction) |
| Cuboid avulsion | Lag screw |
| Cuboid "nutcracker" fracture | Plate fixation; external fixation to restore lateral column length first |
| Anterior calcaneal process | Lag screw or K-wire |
Critical principle: Loss of lateral column length leads to flatfoot deformity and peritalar subluxation. External fixation or distraction may be required before definitive fixation.
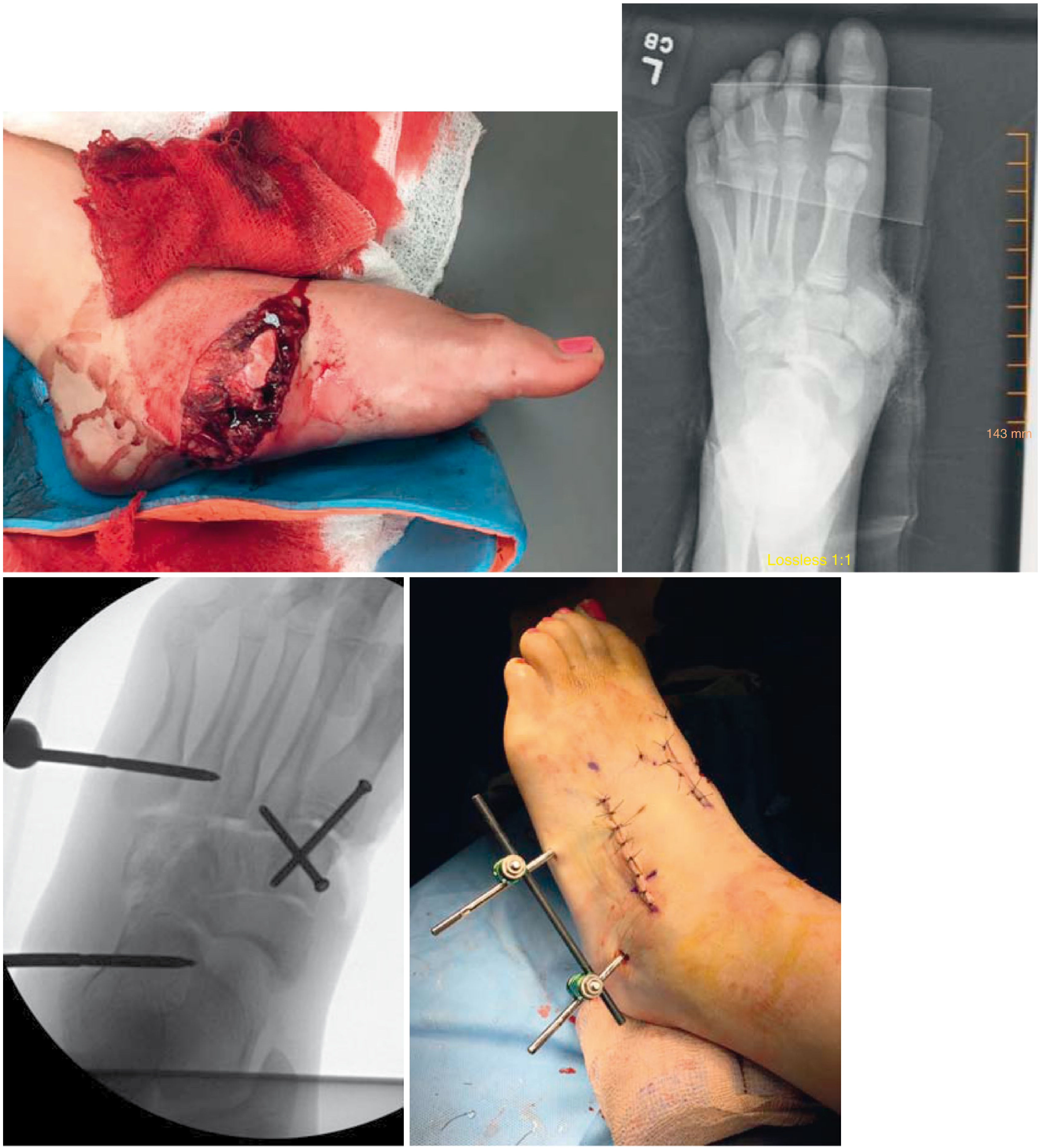
Fig. 93.68 - Open cuboid fracture (top left), AP radiograph (top right), intraoperative fluoroscopy showing crossed K-wire fixation (bottom left), and post-operative external fixation appearance (bottom right). (Campbell's Operative Orthopaedics 15th Ed, 2026)
Step 5: Stabilization of Residual Instability
After bony fixation, any residual ligamentous instability of the Chopart joint is treated with temporary transfixion K-wires:
- Minimum 2 x 1.8 mm K-wires per unstable column
- Wires placed perpendicular to the joint surface
| Column | K-wire trajectory |
|---|---|
| Medial (talonavicular) | Retrograde through navicular into talar head |
| Lateral (calcaneocuboid) | Retrograde through cuboid into calcaneus |
Aftercare Protocol
| Phase | Duration | Management |
|---|---|---|
| Immediate post-op | 0-2 weeks | Non-adherent dressing, below-knee padded cast, strict non-weight-bearing; wound check at 2 weeks |
| Immobilization phase | 6-12 weeks | Continue non-weight-bearing until healing evident; K-wire removal at 6-12 weeks; bridging device minimum 12 weeks |
| Mobilization phase | Post K-wire removal | Progressive weight-bearing; soft brace |
| Rehabilitation | From ~12 weeks | Formal physiotherapy begins; daily toe movement throughout |
| Long-term | Ongoing | Arch support orthoses; monitoring for post-traumatic arthritis |
Gastrocnemius release may be required for postoperative equinus contracture, more common in mid- and hind-foot injuries.
9. Complications
| Complication | Details |
|---|---|
| Post-traumatic arthritis | Most common long-term complication; painful joint arthritis especially at TNJ |
| Missed injury | 20-41% misdiagnosis rate; diagnosed late as ankle sprain |
| Compartment syndrome | Must be ruled out urgently; may require fasciotomy |
| Chronic instability | Especially from purely ligamentous injuries inadequately immobilized |
| Flatfoot deformity | From loss of lateral column length or talonavicular joint disruption |
| Non-union / malunion | Particularly navicular, cuboid |
| Avascular necrosis | Rare; talar head/navicular with vascular compromise |
| Wound complications / infection | Especially with open injuries or extensive ORIF |
| Long-term disability | Most patients cannot return to pre-injury activity levels at 2 years |
| Combined Chopart-Lisfranc injury | Worst functional prognosis of all midfoot injuries |
10. Prognosis
- Purely ligamentous sprains treated conservatively: generally good if properly immobilized
- Displaced fracture-dislocations: most patients cannot return to pre-injury activity level by 2 years (Campbell's, 2026)
- Early anatomical reduction and operative fixation gives significantly better AOFAS and VAS scores than late or inadequate treatment
- Combined Chopart + Lisfranc injuries have the lowest functional scores
- A 2026 study (van Meelen et al., PMID 41578167) specifically examined outcomes of combined navicular + talar head fractures - a particularly morbid injury pattern
Summary Diagram
CHOPART INJURY ALGORITHM
Suspected Chopart Injury
(midfoot pain, swelling, mechanism)
↓
3-view foot X-ray (not ankle)
↓
┌──────┴──────┐
Normal Abnormal
↓ ↓
CT + MRI CT scan
↓ ↓
Confirmed injury Classify severity
↓
┌──────────────────────────────────┐
│ NON-DISPLACED / SPRAIN ONLY │
│ Non-weight-bearing cast 6-8wk │
│ Progressive WB with brace │
└──────────────────────────────────┘
↓
┌──────────────────────────────────┐
│ DISPLACED / DISLOCATION │
│ 1. Closed reduction attempt │
│ 2. If failed → Open reduction │
│ 3. ORIF (lag screws / plates) │
│ 4. K-wire stabilization │
│ 5. NWB 6-12 weeks │
│ 6. K-wire removal + rehab │
└──────────────────────────────────┘
Sources:
- Campbell's Operative Orthopaedics, 15th Ed (2026) - Midfoot Fractures and Dislocations, pp. 5199-5201
- Rosen's Emergency Medicine, 9th Ed - Midtarsal Joint Injuries, p. 751
- Imaging Anatomy Text and Atlas, Vol. 3 - Transverse Tarsal Joint, p. 855
- AO Surgery Reference - Treatment of Chopart Injuries (surgeryreference.aofoundation.org)
- Metcalfe TSN et al. "Chopart dislocations: a review of diagnosis, treatment and outcomes." Arch Orthop Trauma Surg 2024 Jan [PMID: 37715068]
- Rammelt S, Missbach T. "Chopart joint injuries: assessment, treatment, and 10-year results." J Orthop Trauma 2023;37:e14
- Abs B et al. "The missed chapter on midfoot: Chopart injuries." Radiol Med 129:1840-1848 (2024)
- van Meelen TS et al. "Functional Outcome of Chopart Injuries Involving Combined Fractures of the Navicular and Talar Head." Foot Ankle Spec 2026 [PMID: 41578167]
This is a shared conversation. Sign in to Orris to start your own chat.