Breast tumor
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Loading Image
I have comprehensive content for a complete classification answer. Here is the full, structured response:
Classification & Types of Breast Tumors
Breast tumors are broadly divided into epithelial tumors (the majority) and stromal/mesenchymal tumors. Carcinomas are further classified by two overlapping systems: morphological/histological type and molecular/biomarker type.
I. Carcinoma (Epithelial Malignancies)
A. In Situ Carcinoma (Non-Invasive)
These are confined within the ductal-lobular system with the basement membrane intact.
| Type | Key Features |
|---|---|
| Ductal Carcinoma In Situ (DCIS) | Most common in situ lesion; precursor to invasive ductal carcinoma; detected on mammography as microcalcifications; when untreated, ~30-50% progress to invasive carcinoma in the same breast |
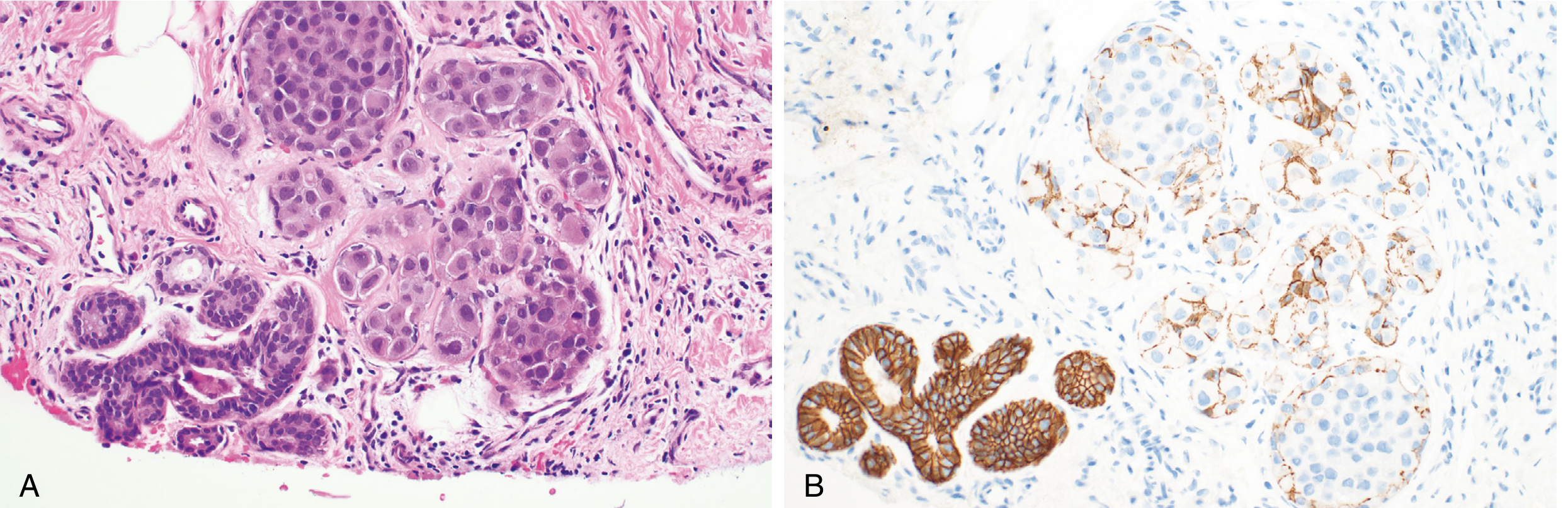
| Lobular Carcinoma In Situ (LCIS) | Marker of increased risk rather than a direct precursor; when invasive cancer later develops, ~2/3 arise in the same breast, ~1/3 in the contralateral breast; cells are small, rounded, and dyscohesive (E-cadherin negative) |
B. Invasive (Infiltrating) Carcinoma
1. No Special Type (NST) - "Invasive Ductal Carcinoma"
- Most common, ~75% of all invasive carcinomas
- Heterogeneous group; does not fit criteria for any special subtype
- Presents as a hard, irregular mass with desmoplastic stroma; grating sound on sectioning
- Graded by Nottingham Histologic Score (tubule formation + nuclear pleomorphism + mitotic rate):
- Grade 1 (well differentiated): tubular/cribriform pattern, small uniform nuclei, low mitotic rate
- Grade 2 (moderately differentiated): mixed solid/glandular growth, moderate pleomorphism
- Grade 3 (poorly differentiated): ragged nests/sheets, marked pleomorphism, high mitotic rate, necrosis
- "Medullary pattern" = high-grade NST with prominent tumor-infiltrating lymphocytes (TILs); previously considered a separate entity
2. Special Histologic Subtypes
Predominantly ER-positive / Luminal subtype:
| Subtype | Morphology | Notes |
|---|---|---|
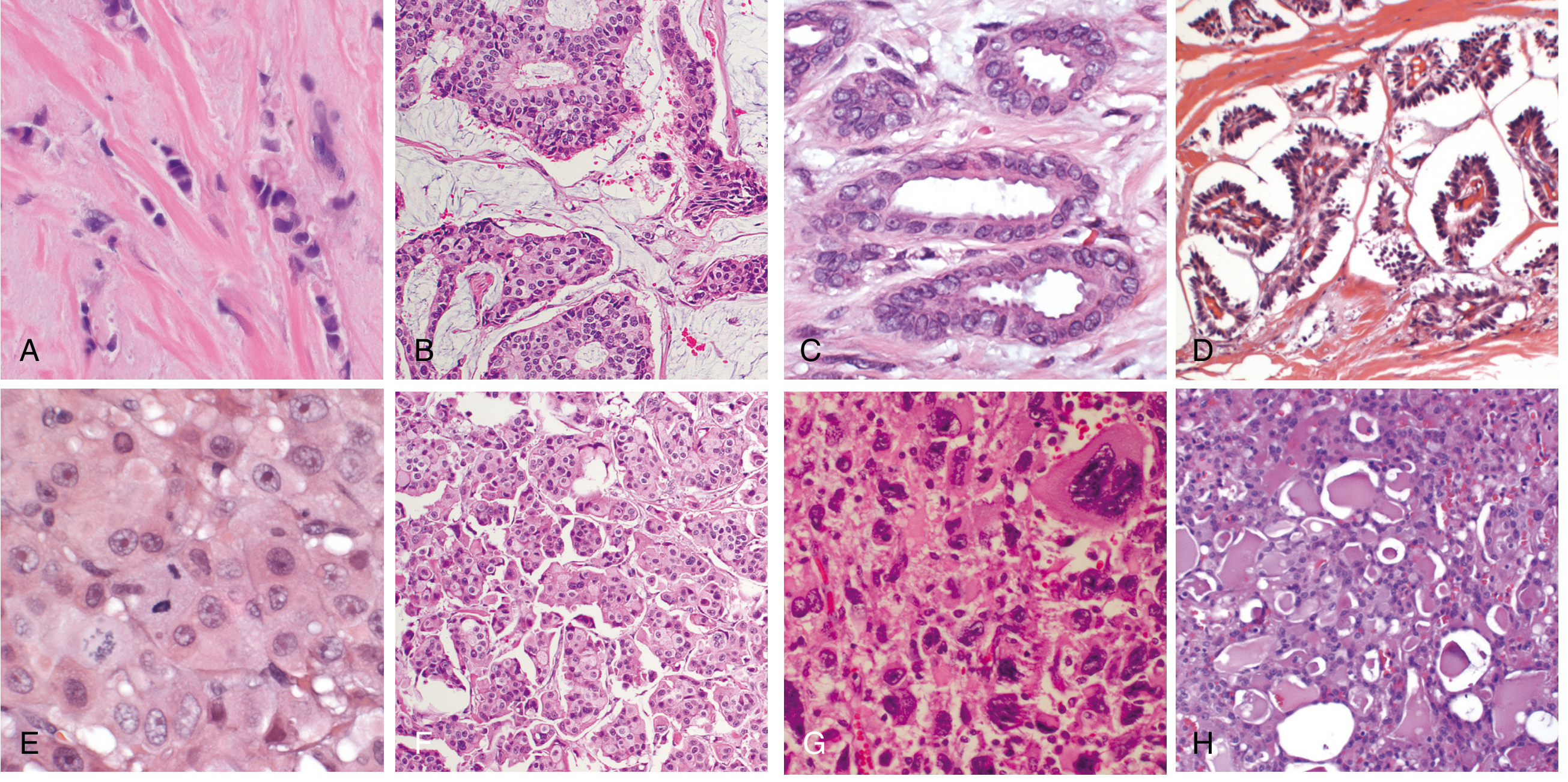
| Invasive Lobular Carcinoma | Dyscohesive single-file "Indian file" cords; signet ring cells with intracytoplasmic mucin; minimal desmoplasia | Most common special subtype; insidious spread, hard to detect on imaging; E-cadherin loss |
| Mucinous (Colloid) Carcinoma | Clusters of cells floating in large lakes of extracellular mucin; well-circumscribed | Soft, gelatinous gross appearance; better prognosis |
| Tubular Carcinoma | Exclusively well-formed tubules; may mimic benign sclerosing lesion | Excellent prognosis |
| Cribriform Carcinoma | Invasive nests with cribriform (sieve-like) morphology | Favorable prognosis |
| Papillary Carcinoma | True papillary fronds lined by tumor cells | Often intracystic; generally good prognosis |
Predominantly HER2-positive:
| Subtype | Morphology |
|---|---|
| Apocrine Carcinoma | Cells resemble apocrine sweat gland cells; enlarged round nuclei, prominent nucleoli, abundant eosinophilic granular cytoplasm |
| Invasive Micropapillary Carcinoma | Hollow "balls" of cells floating in intercellular fluid; mimics papillae but lacks fibrovascular cores; associated with lymphovascular invasion |
Predominantly Triple-Negative (TNBC):
| Subtype | Notes |
|---|---|
| Metaplastic Carcinoma | Squamous or mesenchymal (spindle, chondroid, osseous) differentiation; myoepithelial-like gene expression; poor prognosis overall |
| Salivary Gland-Like Carcinomas | Adenoid cystic, mucoepidermoid, secretory carcinoma; histologically identical to salivary gland counterparts; relatively favorable prognosis despite TNBC status |
Clinical Presentation Subtype:
- Inflammatory Breast Carcinoma - not a histologic subtype; caused by extensive dermal lymphovascular plugging by carcinoma cells; presents with erythema, skin thickening, and "peau d'orange" (skin dimpling due to tethering by Cooper's ligaments); no discrete palpable mass; usually high-grade; commonly mistaken for infection
II. Molecular (Biomarker-Based) Classification
This is the most clinically relevant classification for treatment decisions:
| Molecular Group | Receptor Status | Intrinsic Subtypes | Key Features |
|---|---|---|---|
| Luminal A | ER+/PR+, HER2-, low Ki-67 | Luminal A | Best prognosis; low proliferation; respond well to endocrine therapy |
| Luminal B | ER+/PR±, HER2-, high Ki-67 OR HER2+ | Luminal B | Higher proliferation than A; less favorable prognosis |
| HER2-enriched | ER-, PR-, HER2+ | HER2 | HER2 gene amplification; responds to HER2-targeted therapy (trastuzumab) |
| Triple Negative (TNBC) | ER-, PR-, HER2- | Basal-like | Often BRCA1-mutated; high grade; poor prognosis; no targeted therapy historically |
| Normal-like | ER+, HER2- | Normal-like | Gene profile resembles normal breast; intermediate prognosis |
| Claudin-low | Often TNBC | Claudin-low | Low expression of cell-cell junction proteins; stem-cell-like features |
The three major clinical groups used in practice are:
- Luminal (ER-positive/HER2-negative) - most common; treated with endocrine therapy
- HER2 - overexpression usually due to gene amplification; treated with HER2 inhibitors
- TNBC - no targeted therapy; chemotherapy backbone; DNA repair defects common (BRCA1/TP53)
III. Stromal / Non-Epithelial Tumors
These arise from the two types of breast stroma:
From Intralobular Stroma (breast-specific "biphasic" tumors - contain both stromal and epithelial components):
| Tumor | Notes |
|---|---|
| Fibroadenoma | Most common benign breast tumor overall; driven by MED12 mutations (same gene mutated in uterine leiomyomas); responds to estrogen; common in women aged 20-35 |
| Phyllodes Tumor | Closely related to fibroadenoma; stromal overgrowth with leaf-like projections; ranges from benign to borderline to malignant; malignant phyllodes can metastasize hematogenously |
From Interlobular Stroma:
- Same mesenchymal tumors as in other tissues: lipoma, angiosarcoma (especially post-radiation), myofibroblastoma
IV. Summary Diagram
BREAST TUMORS
├── EPITHELIAL (Carcinoma) ─ ~95% of malignant breast tumors
│ ├── In Situ
│ │ ├── DCIS (ductal) → precursor to invasive
│ │ └── LCIS (lobular) → risk marker + precursor
│ └── Invasive
│ ├── No Special Type (NST) ~75% ← most common
│ └── Special Types
│ ├── Lobular (most common special type)
│ ├── Mucinous / Tubular / Cribriform / Papillary (luminal, good prognosis)
│ ├── Apocrine / Micropapillary (HER2-enriched)
│ ├── Metaplastic / Salivary gland-like (TNBC)
│ └── Inflammatory (clinical subtype, not histologic)
│
└── STROMAL / MESENCHYMAL
├── Intralobular: Fibroadenoma, Phyllodes tumor
└── Interlobular: Lipoma, Angiosarcoma, Myofibroblastoma
Key points to remember:
- Lifetime risk in US women: ~1 in 8 (by age 90)
- ~12% of breast cancers involve germline mutations; BRCA1/BRCA2 account for half of hereditary cases
- High-risk genes: BRCA1, BRCA2, PALB2, TP53
- NST (no special type) = ~75% of invasive carcinomas; invasive lobular = most common "special" subtype
- Prognosis depends on biologic type (molecular group), grade, and anatomic stage (AJCC 8th edition combines molecular + anatomic stage into "prognostic stage")
Sources: Robbins & Cotran Pathologic Basis of Disease (9780443264528); Robbins & Kumar Basic Pathology (9780323790185)
This is a shared conversation. Sign in to Orris to start your own chat.