Tell me about pyogenic liver abscess. Yep.
Reading File
Finding Sources
Finding Sources
Searching PubMed
"pyogenic liver abscess"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive textbook content and imaging. Here is a thorough, well-organized answer:
Pyogenic Liver Abscess (PLA)
Definition and Epidemiology
A pyogenic liver abscess is a collection of pus and inflammatory tissue within the hepatic parenchyma caused by bacterial infection. It is the most common type of visceral abscess. Incidence varies significantly by geography - in Taiwan, where PLA is endemic, rates rose from 10.8 to 15.5 cases per 100,000 person-years between 2000-2011, while in Europe and Canada the rate is 1.1-3.7 cases per 100,000. A Minnesota study documented a rise from 2.1 to 3.6 per 100,000 over 35 years. Men and individuals over 65 are disproportionately affected. Morbidity is substantial and mortality ranges from 6% to 10%.
- Fischer's Mastery of Surgery, 8th ed.
- Maingot's Abdominal Operations
Routes of Infection / Pathogenesis
PLA develops through several pathways:
| Route | Mechanism | Examples |
|---|---|---|
| Biliary (most common today) | Direct spread from infected bile ducts | Cholangitis, choledocholithiasis, malignant/benign strictures, instrumentation |
| Portal (pylephlebitis) | Suppurative portal vein thrombophlebitis | Appendicitis, diverticulitis, colorectal malignancy, IBD |
| Hematogenous | Arterial seeding | Endocarditis, severe sepsis, dental/periodontal disease |
| Direct extension | Spread from adjacent structures | Cholecystitis, perinephric abscess |
| Traumatic/Iatrogenic | Necrotic tissue superinfection | Post-TACE, post-ablation, liver surgery, foreign body ingestion (fish/chicken bones) |
| Cryptogenic | No identifiable source | ~35-40% of cases |
Historically, pylephlebitis from untreated appendicitis was the leading cause. Today, biliary disease and instrumentation dominate. PPI use increases risk by reducing gastric acidity and allowing pathogen survival.
- Fischer's Mastery of Surgery; Yamada's Textbook of Gastroenterology, 7th ed.; Sleisenger & Fordtran's GI and Liver Disease
Risk Factors
- Diabetes mellitus
- Malnutrition, immunosuppression
- Prior hepatobiliary/pancreatic disease
- Liver transplant
- Cirrhosis
- History of biliary-intestinal anastomosis or sphincterotomy
- Regular PPI use
- IBD, colorectal malignancy
- Oral flora / periodontal disease (especially in alcoholics - cryptogenic cases)
One population-based study noted a fourfold higher risk of GI malignancy in patients presenting with PLA - screening for occult malignancy is warranted.
Microbiology
Most PLA are polymicrobial. Key organisms:
- E. coli and Klebsiella pneumoniae - most frequently isolated
- Klebsiella pneumoniae (hypervirulent/mucoid) - a distinct syndrome, predominantly in Asia (accounts for ~80% of cases in Taiwan), community-acquired, associated with diabetes, and carries a high risk of metastatic complications (endophthalmitis, meningitis, necrotizing fasciitis)
- Streptococcus milleri group (S. anginosus, S. constellatus, S. intermedius) - normal GI flora, important cause
- Bacteroides fragilis, Fusobacterium necrophorum - most common anaerobes
- Staphylococci - post-trauma/instrumentation or hematogenous; prompt evaluation for infective endocarditis
- Proteus, Pseudomonas spp.
- Rare: Yersinia, Pasteurella, Haemophilus, Listeria, Actinomyces, Clostridium
Anaerobic organisms are likely underrepresented in culture due to suboptimal isolation methods.
- Sleisenger & Fordtran's; Fischer's Mastery of Surgery
Clinical Features
The classic pre-antibiotic triad was spiking fever + RUQ pain + shock. Today, the presentation is typically more indolent, especially in older adults:
- Fever (most consistent finding; can be low-grade)
- Right upper quadrant or epigastric pain - may be pleuritic; may radiate to the right shoulder if the diaphragm is irritated
- Malaise, anorexia, weight loss, nausea
- Symptoms may be present 1 month or more before diagnosis
- Jaundice - uncommon; if present, suggests biliary obstruction
- Normochromic normocytic anemia, weight loss on exam
- Multiple abscesses (often biliary source) tend to present more acutely with sepsis/shock; solitary abscesses are more indolent
Without treatment, mortality approaches 100%. Rupture into the peritoneum is a surgical emergency.
Imaging
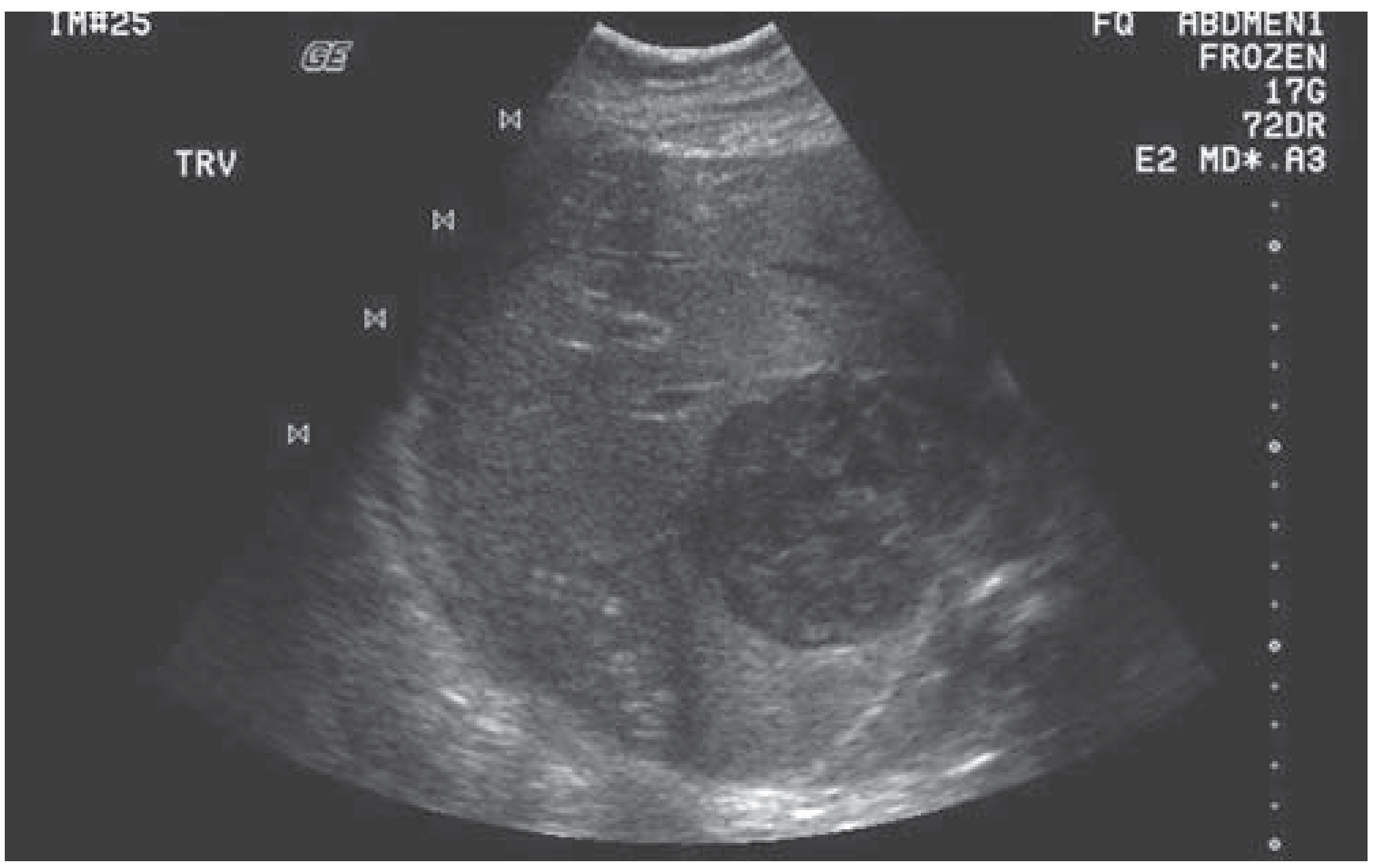
Ultrasound (US)
First-line, widely accessible. Appearance varies with stage:
- Early: mixed hypo/hyperechoic solid-appearing lesion
- Later: complex cystic mass with anechoic spaces and irregular wall, internal septations
- Gas-forming organisms: "dirty shadowing"
- No intracavitary Doppler flow (flow in periphery/septations only)
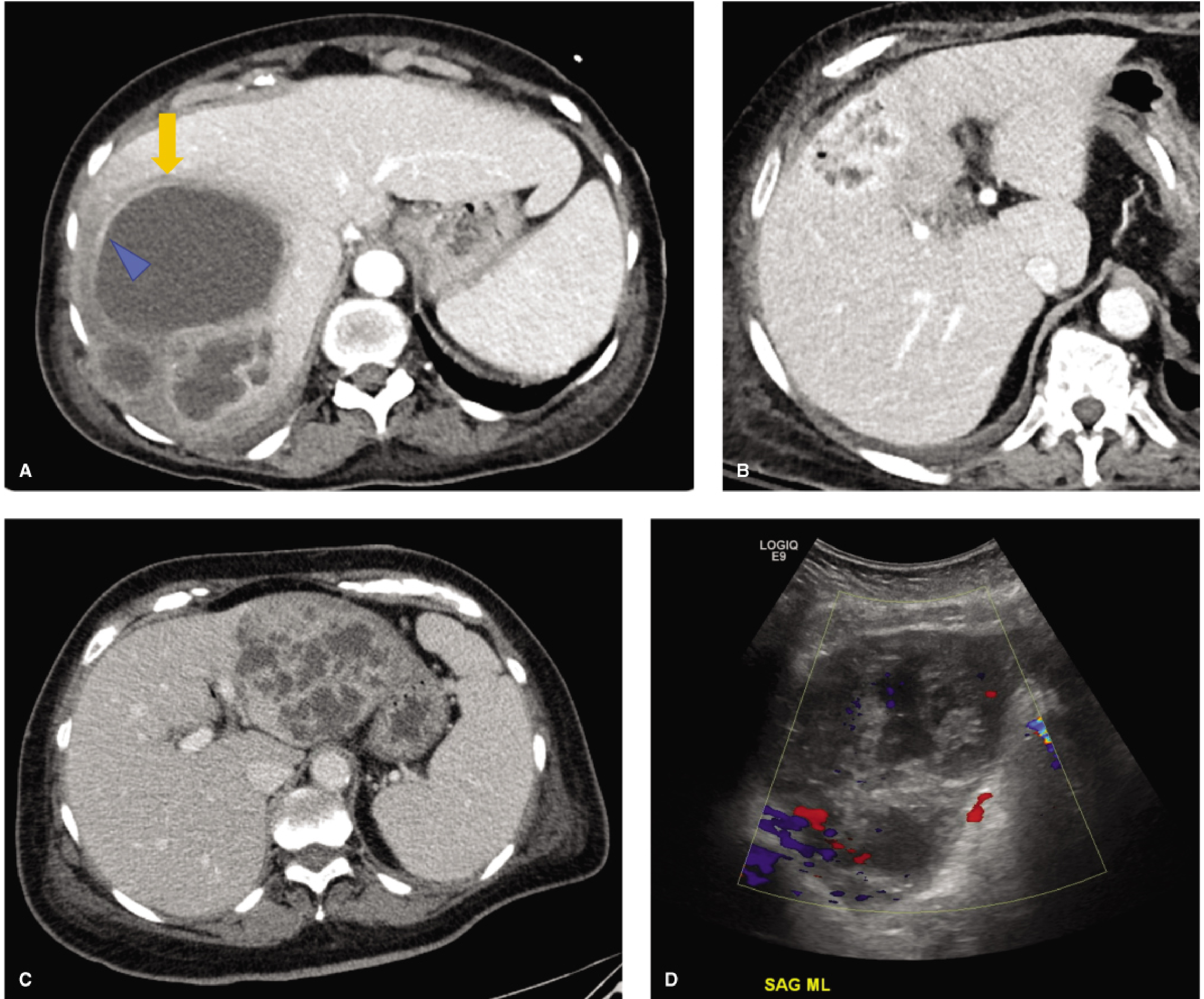
CT (contrast-enhanced)
Most useful for characterization and planning:
- Hypoattenuating mass with enhancing rim (most common appearance)
- "Double target sign" - central hypoattenuating pus cavity + enhancing inner rim + outer hypoattenuating rim of parenchymal edema
- "Cluster sign" - multiple small rim-enhancing lesions beginning to coalesce
- "Turquoise sign" - arborizing septa in K. pneumoniae abscess
- Gas within the abscess = gas-forming organism
MRI
- T1: hypointense center
- T2: hyperintense with perilesional edema
- DWI: restricted diffusion (bright DWI, dark ADC) - helpful to distinguish abscess from necrotic tumor
- Superior soft tissue contrast, but not always needed if US/CT is diagnostic
Laboratory Findings
- Elevated alkaline phosphatase (common, often disproportionate)
- Elevated bilirubin, transaminases
- Leukocytosis
- Blood cultures positive in ~50% (up to 95% in K. pneumoniae PLA)
- Anemia
- Hypoalbuminemia in severe/chronic cases
Treatment
Treatment involves three pillars: antibiotics + drainage + source control.
1. Antibiotics
- Draw blood cultures and aspirate abscess before starting antibiotics when possible
- Start broad-spectrum IV antibiotics empirically, covering gram-negatives, gram-positives, and anaerobes
- Classic regimens: aminoglycoside + clindamycin + ampicillin or vancomycin; fluoroquinolones can replace aminoglycosides; metronidazole can replace clindamycin
- Single-agent options: piperacillin-tazobactam, imipenem-cilastatin, or ticarcillin-clavulanate
- Note: K. pneumoniae is intrinsically resistant to ampicillin; first-generation cephalosporins lack adequate anaerobic coverage
- Duration: traditionally 4-6 weeks, though many studies support success with 2 weeks of IV therapy followed by oral step-down based on clinical/culture response
- Empiric anaerobic coverage should always be included in older patients and those with malignancy
2. Percutaneous Drainage
Now the first-line invasive intervention for most PLA:
- Performed under US or CT guidance
- Either needle aspiration (single/repeat) or catheter drainage
- Catheter placement preferred for large, complex, or multiloculated abscesses
- Success rates are high; the method replaced open surgery as standard of care since the 1980s
Contraindications / relative indications to avoid percutaneous drainage:
- Coagulopathy
- Multiple small abscesses (microabscesses)
- Intervening vascular structures (e.g., portal vessels blocking safe access)
- Ascites
- Need for transpleural drainage
- Abscesses requiring surgical source control
3. Surgical Drainage
Reserved for:
- Failure of percutaneous drainage/antibiotics
- Need to treat the underlying intra-abdominal source surgically
- Multiple macroscopic abscesses not amenable to percutaneous approach
- Patient on steroids
- Concomitant ascites
Historically done extraperitoneally via 12th-rib resection; now transperitoneal approach allows simultaneous source control, full liver assessment, and biliary exploration.
- Maingot's Abdominal Operations; Fischer's Mastery of Surgery
Complications
Up to 40% of patients develop complications:
- Sepsis - most common
- Pleural effusion / empyema
- Rupture into peritoneum (peritonitis, high mortality)
- Subphrenic abscess (controlled leak)
- Hemobilia
- Portal vein or hepatic vein thrombosis - can cause portal hypertension or Budd-Chiari syndrome
- Bacteremia with metastatic seeding
K. pneumoniae-specific complications:
-
Bacteremia in ~95% of cases
-
Endophthalmitis (6-61%) - can occur after drainage; often results in permanent visual loss
-
Meningitis, brain abscess, CNS complications
-
Necrotizing fasciitis
-
Septic pulmonary emboli
-
DIC, acute renal failure
-
Maingot's Abdominal Operations; Yamada's Gastroenterology
Prognosis / Poor Prognostic Factors
Historical mortality ranged from 11% to 88%; with modern management it is 6-10% overall, and 6-17% for K. pneumoniae PLA. Poor outcomes are associated with:
| Clinical | Laboratory |
|---|---|
| Age >70 years | WBC >20,000/mm³ |
| Diabetes mellitus | Increasing bilirubin |
| Associated malignancy | Increasing SGOT/AST |
| Biliary etiology | Albumin <2 g/dL |
| Multiple abscesses | |
| Septicemia | |
| Polymicrobial bacteremia | |
| Significant complication |
For K. pneumoniae PLA, abscess >5 cm, intrahepatic gas, APACHE III >40, delayed drainage, and thrombocytopenia are additional poor prognosticators. The main concern with K. pneumoniae PLA today is not mortality per se, but catastrophic disability from irreversible ocular and neurological complications - the K1 genotype is particularly virulent.
Key Distinctions from Amebic Abscess
| Feature | Pyogenic | Amebic |
|---|---|---|
| Cause | Mixed bacteria | Entamoeba histolytica |
| Typical patient | Elderly, comorbidities | Traveler from endemic area (Mexico, S. Asia, Africa); male predominance |
| Microbiology | Polymicrobial | Single organism |
| Serology | Not helpful | Diagnostic (IFA/ELISA) |
| Number | Often multiple | Usually solitary (right lobe) |
| Contents | Pus | "Anchovy paste" fluid |
| Treatment | Abx + drainage | Metronidazole; drainage less often needed |
Sources: Fischer's Mastery of Surgery 8th ed.; Yamada's Textbook of Gastroenterology 7th ed.; Sleisenger & Fordtran's GI and Liver Disease; Maingot's Abdominal Operations; Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.