Ankle surgical anatomy with pictures
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
I now have all the core anatomical text and images. Let me compile the comprehensive answer.
Ankle Surgical Anatomy
Sources: Rockwood and Green's Fractures in Adults, 10th ed. (2025) | Rheumatology, 2-Volume Set (2022, Elsevier)
1. Bony Anatomy - The Mortise
The ankle is a three-bone hinge (mortise) joint formed by:
- Tibial plafond - the ceiling of the mortise
- Medial malleolus - shorter and more anterior; the axis of the joint is in 15 degrees of external rotation relative to the knee
- Posterior malleolus - a dorsal projection of the tibia that enlarges the articular surface
- Lateral malleolus (distal fibula) - articulates with the lateral facet of the talus; carries approximately 1/6 of the axial load
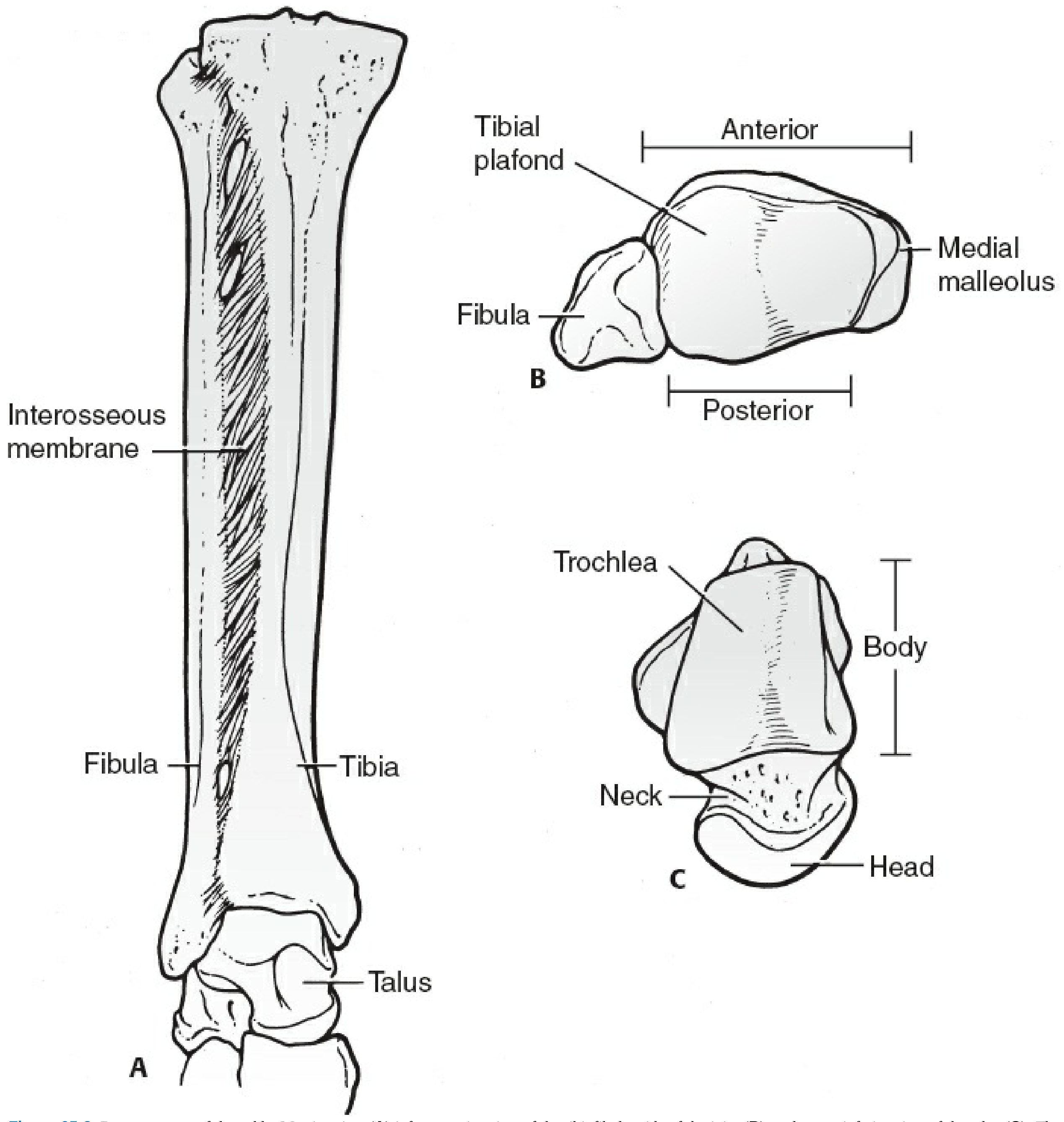
The talus is geometrically complex - it describes a frustum (truncated cone) lying transversely in the mortise, wider anteriorly than posteriorly. 70% of its surface is articular cartilage. It has no direct muscular attachments and a tenuous retrograde vascular supply. In dorsiflexion (close-packed position) the wider anterior talus locks into the mortise; in plantarflexion the narrower posterior portion allows physiologic external rotation and inversion, making this the position of instability.
A landmark biomechanical study (Ramsey & Hamilton) showed that just 1 mm of lateral talar displacement reduces the tibiotalar contact area by 42% - the basis for the principle of anatomical reduction.
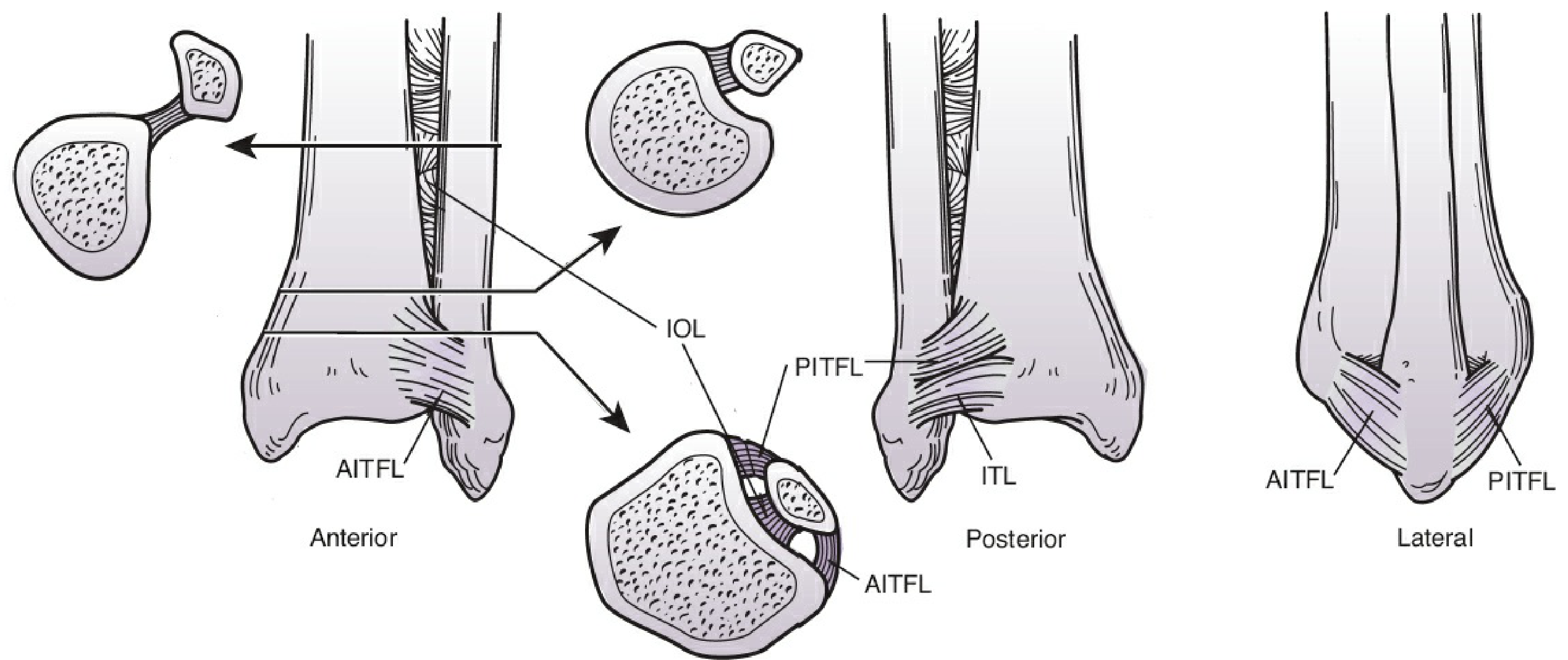
2. The Syndesmosis
The tibiofibular syndesmosis is where the fibula sits in the incisura fibularis on the lateral tibia, stabilized by four structures:
| Ligament | Origin | Insertion | Notes |
|---|---|---|---|
| AITFL (anteroinferior tibiofibular ligament) | Tubercle of Chaput (anterolateral tibia) | Tubercle of Wagstaffe (fibula) | Can avulse bony tubercles |
| PITFL (posteroinferior tibiofibular ligament) | Volkmann tubercle (posterior malleolus) | Posterior fibula | Extremely strong; trimalleolar fragments often remain attached to fibula via this |
| IOL (interosseous ligament) | Continuous with interosseous membrane | - | Provides the bulk of syndesmotic strength |
| ITL (inferior transverse ligament) | Deep component of PITFL | - | - |
Surgical pearl: Reduction of the distal fibula usually reduces the posterior malleolus (via the PITFL attachment), and stabilizing the posterior malleolus often restores mortise stability.
3. Ligamentous Anatomy
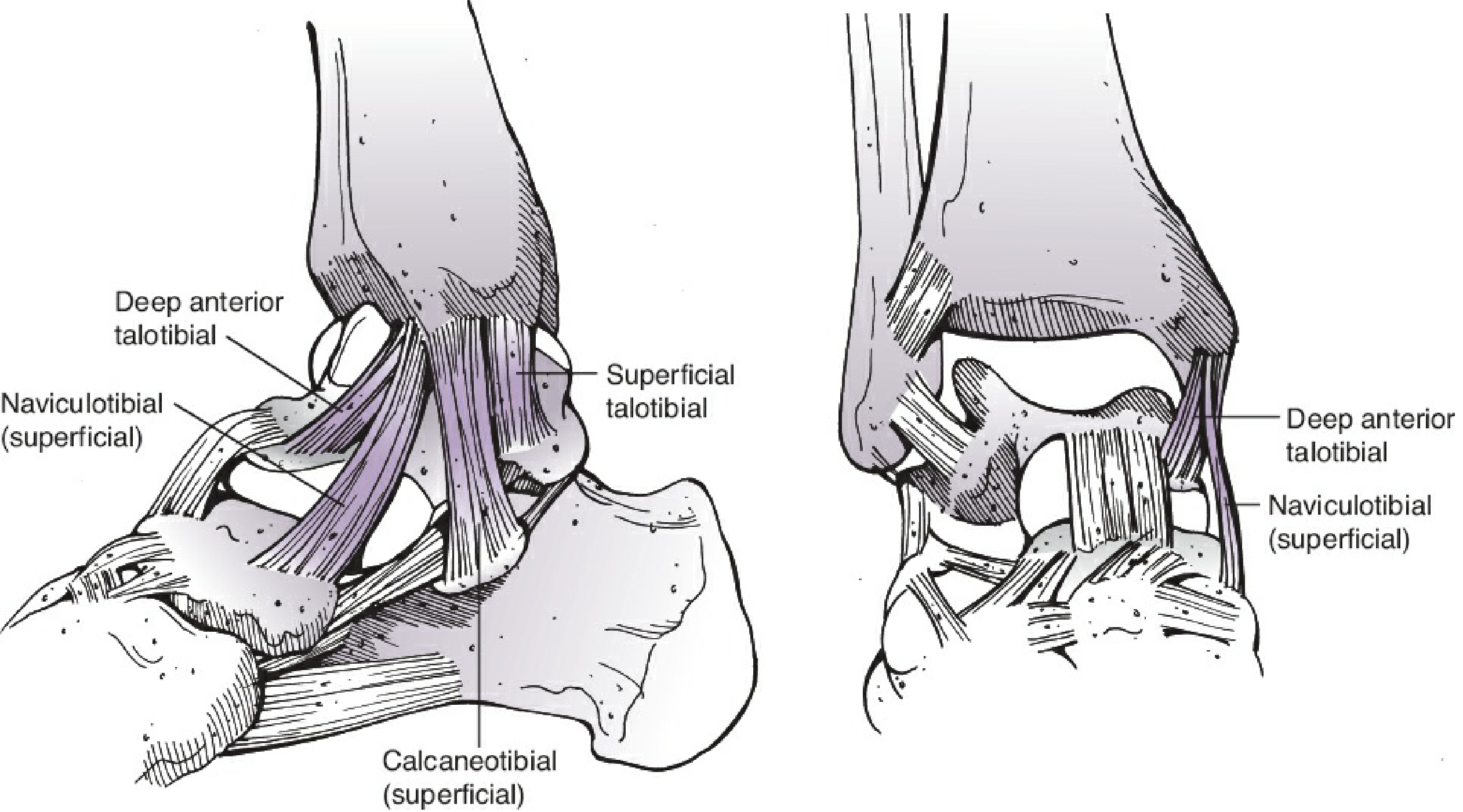
Medial - Deltoid Ligament
The deltoid (medial collateral) ligament has two layers:
- Superficial deltoid - arises from the anterior colliculus of the medial malleolus; fans out to insert into the talus, navicular, and sustentaculum of the calcaneus; continuous with the tendon sheaths of tibialis posterior and FHL
- Deep deltoid - intra-articular; runs from the posterior colliculus and intercollicular groove to the dome of the talus; this is the key restraint against lateral talar displacement and rotation
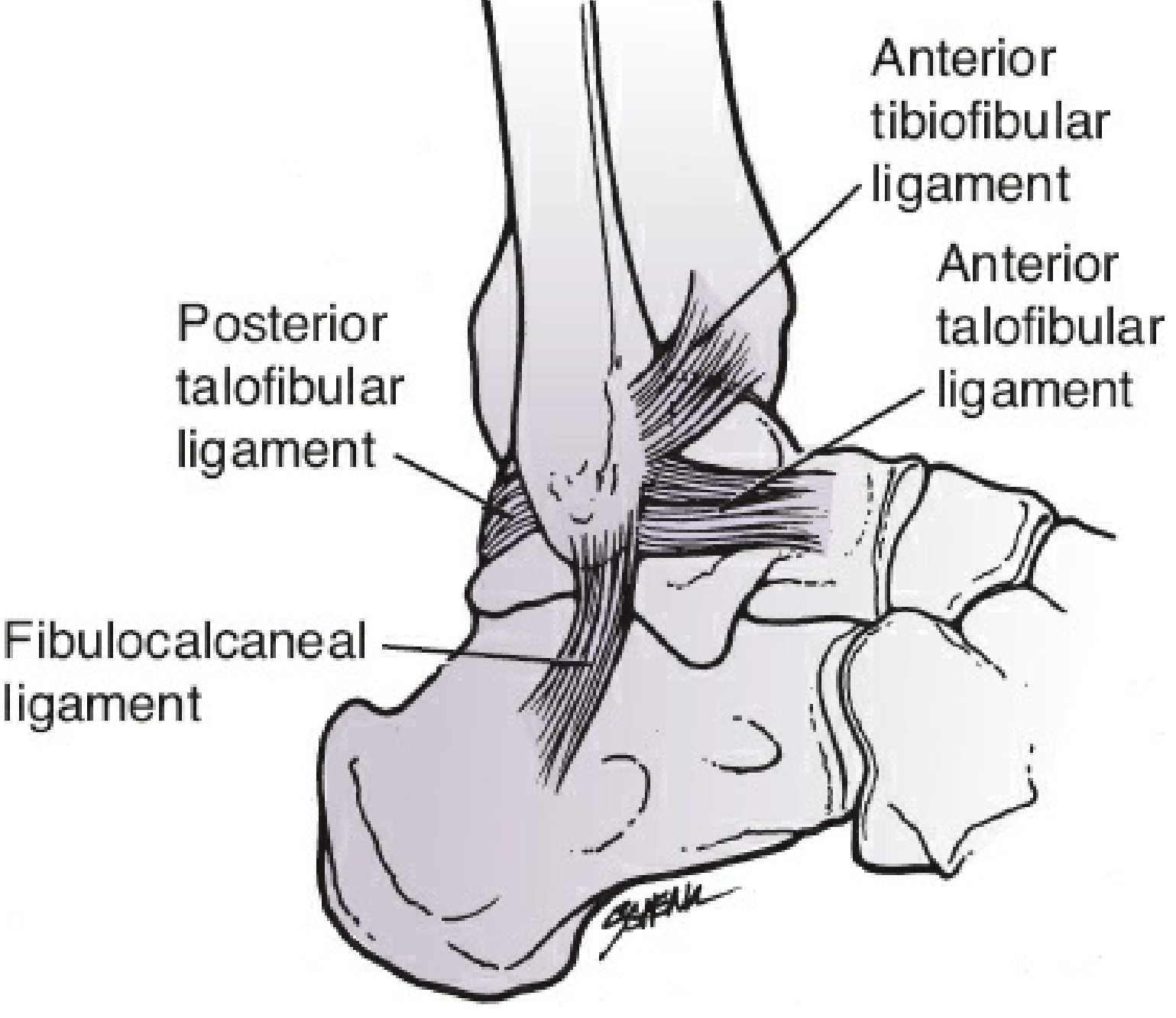
Lateral - Collateral Complex
Three ligaments form the lateral complex:
| Ligament | Course | Clinical significance |
|---|---|---|
| ATFL (anterior talofibular) | From fibular tip anteriorly to lateral talar body | Weakest; most commonly injured in inversion sprains |
| FCL / CFL (fibulocalcaneal) | Vertically downward from fibular tip to lateral calcaneus | Injured in more severe sprains |
| PTFL (posterior talofibular) | Horizontally backward from fibular tip | Strongest; rarely injured in isolation |
Key stability rule: Two of the three stabilizing complexes (medial, lateral, syndesmosis) must be intact for the ankle to remain stable.
4. Soft Tissue Compartments - Tendons, Nerves & Vessels
Tendons cross the ankle in three surgical compartments. The classic mnemonic for the posteromedial structures is "Tom, Dick And Very Nervous Harry" (Tibialis posterior, flexor Digitorum longus, posterior tibial Artery, tibial Nerve, flexor Hallucis longus).
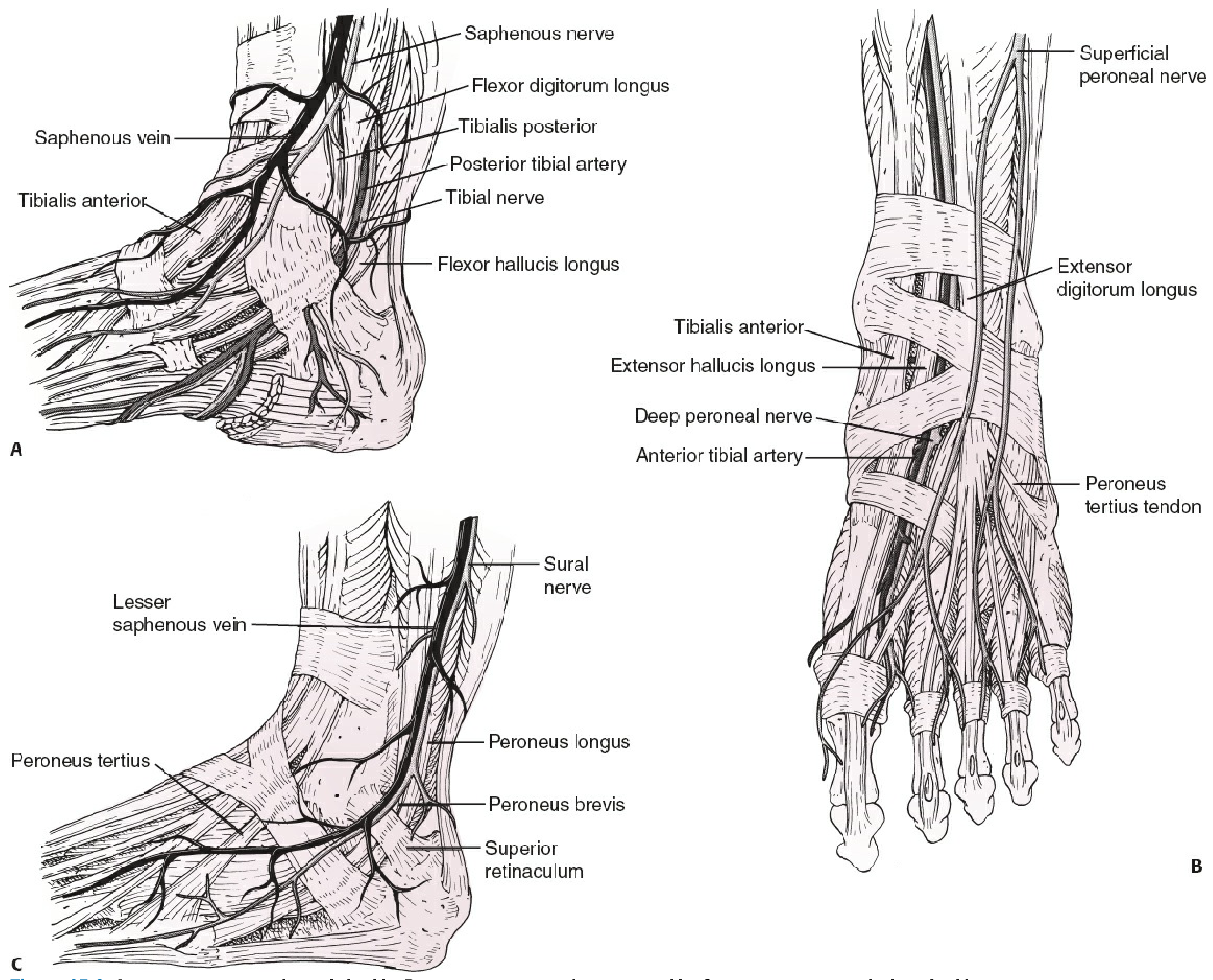
Anterior Compartment (under extensor retinacula)
From medial to lateral, from most medial to lateral:
- Tibialis anterior
- Extensor hallucis longus (EHL)
- Deep peroneal nerve + dorsalis pedis artery (anterior tibial artery)
- Extensor digitorum longus (EDL)
- Peroneus tertius
The safe anterior surgical plane lies between tibialis anterior and EHL. The deep peroneal nerve and dorsalis pedis artery lie just lateral to EHL - retract EHL medially to protect them.
Posteromedial Compartment (under lacinate ligament = tarsal tunnel)
From anterior to posterior (Tom, Dick ANd Very Nervous Harry):
- Tibialis posterior
- Flexor Digitorum longus
- Posterior tibial Artery (with venae comitantes)
- Tibial Nerve
- Flexor Hallucis longus (FHL)
FHL can be identified at this level by the muscle fibers that insert into it distally. This is an important landmark for posterior approaches.
Posterolateral Compartment (under peroneal retinaculum)
- Peroneus brevis (more anterior, directly behind fibula)
- Peroneus longus (posterior to brevis)
- Sural nerve and lesser saphenous vein - lie approximately two-thirds of the way between the distal fibula and the Achilles tendon
5. Surgical Approaches
Medial Approach
- Interval: Between dorsiflexors (deep peroneal nerve) and invertors/plantarflexors (posterior tibial nerve) - a true internervous plane
- Incision: Straight longitudinal over the malleolus, or curvilinear anteriorly for plafond access
- At risk: Great saphenous vein and saphenous nerve, which pass just anterior to the medial malleolus
Posteromedial Approach
- Incision: Longitudinal, halfway between medial malleolus and Achilles tendon
- Deep plane: Between FHL (retracted medially) and peroneal tendons laterally
- Retracting FHL medially exposes the back of the ankle joint while protecting the posterior tibial neurovascular bundle
Lateral Approach
- Incision: Directly over the subcutaneous border of the fibula
- At risk: Superficial peroneal nerve - emerges through deep fascia in the distal 1/3 of the leg; a substantial branch lies within 5 mm of the fibula in 50% of cases at 10 cm above the malleolar tip, and in 20% of cases at 5 cm above the tip - blunt dissection is mandatory
- For posterior plating, the incision shifts to the posterior border of the fibula; the safe interval is between peroneal tendons (anteriorly) and FHL (posteriorly), providing access to both the posterior fibula and the posterior malleolus through the same window
Posterolateral Approach
- Exploits the same deep plane as the posteromedial approach (between FHL and peroneal tendons)
- Sural nerve is at risk subcutaneously
- Useful for accessing the posterior malleolus when the fracture plane results in a posterolateral fragment
6. Neurovascular Summary
| Structure | Location | Surgical Risk |
|---|---|---|
| Deep peroneal nerve + dorsalis pedis a. | Anterior, between EHL and EDL | Anterior approach |
| Superficial peroneal nerve | Subcutaneous in distal 1/3 of leg, variable | Lateral approach |
| Sural nerve | ~2/3 between fibula and Achilles | Posterolateral approach |
| Posterior tibial nerve + artery | Posteromedial, within tarsal tunnel | Posteromedial approach |
| Saphenous nerve + vein | Just anterior to medial malleolus | Medial approach |
Rockwood and Green's Fractures in Adults, 10th ed. (2025), pp. 3287-3291 | Rheumatology, 2-Volume Set (2022), p. 84
This is a shared conversation. Sign in to Orris to start your own chat.