6.Evaluation and Management of Peripheral Nerve Injuries and Disorders : History, Observation, Palpation, Motor & Sensory examination, Reflex testing, differential Diagnosis, Balance & Coordination examination, Gait analysis, Functional analysis, List of Problems & Complications, short & Long Term goals, Management of systemic complications, Management of Mechanical Complications, Use of various Neuro physiological approaches& Modalities in Hereditary motor sensory neuropathy, Guillain-Barre syndrome, Brachial plexus palsy, Thoracic outlet syndrome, Lumbosacral plexus lesions, Phrenic & intercostals nerve lesions, Median nerve palsy, Ulnar nerve palsy, Radial nerve palsy, Musculocutaneous nerve palsy, Anterior & Posterior interosseous nerve palsy, Axillary nerve palsy, Long thoracic nerve palsy, Supra scapular nerve palsy, sciatic nerve palsy, Tibial nerve palsy, Common peroneal nerve palsy, Femoral nerve palsy, Obturator nerve palsy, and Pudental nerve palsy. [10 hours]
peripheral nerve injury physiotherapy rehabilitation neurophysiological approaches modalities 2024
Evaluation and Management of Peripheral Nerve Injuries and Disorders
PART I: EVALUATION FRAMEWORK
1. History Taking
- Onset (sudden vs. gradual), duration, and progression
- Distribution of weakness, numbness, tingling, or pain
- Character of sensory symptoms: burning, shooting, electric, pins-and-needles
- Trauma: traction, compression, laceration, fracture (nerve adjacent to bone)
- Systemic disease: diabetes, hypothyroidism, renal failure, vasculitis, HIV
- Toxic exposure: alcohol, heavy metals (lead, arsenic, mercury), chemotherapy drugs (vincristine, paclitaxel, cisplatin)
- Hereditary: family history of foot deformity, gait problems, or similar symptoms
- Iatrogenic: post-surgical, injection injuries, prolonged tourniquet use
- Recent infections (preceding GBS by 1-4 weeks): Campylobacter, CMV, EBV, Zika
- Impact on ADLs: fine motor tasks, dressing, grip, walking, bladder/bowel
- Occupation and hand dominance
- Medications (some are neurotoxic: isoniazid, metronidazole)
- Nutritional status (B1, B6, B12 deficiencies)
- Rapidly progressive weakness (GBS)
- Bilateral involvement
- Respiratory compromise (phrenic nerve, GBS)
- Bladder/bowel dysfunction (lumbosacral plexus, pudendal nerve)
2. Observation
| Finding | Implication |
|---|---|
| Wrist drop | Radial nerve palsy |
| Claw hand (ring/little fingers) | Ulnar nerve palsy |
| Ape/simian hand | Combined median + ulnar |
| Foot drop (steppage gait) | Common peroneal nerve palsy |
| Winging of scapula | Long thoracic nerve palsy (serratus anterior) |
| Shoulder asymmetry/atrophy | Suprascapular or axillary nerve palsy |
| Thenar wasting | Median nerve (carpal tunnel or high lesion) |
| Hypothenar wasting | Ulnar nerve palsy |
| Pes cavus + hammer toes | Hereditary motor sensory neuropathy (CMT) |
| Fasciculations | Denervation / lower motor neuron disease |
| Pressure ulcers / burns | Sensory loss (insensate skin) |
| Asymmetric chest expansion | Phrenic nerve palsy |
| Posture: shoulder depression | Brachial plexus traction injury |
- Dry, shiny, hairless skin = autonomic/sensory involvement
- Sudomotor testing (sweat pattern) over the territory of suspected nerve
- Joint deformities from chronic denervation
3. Palpation
- Nerve palpation: Examine accessible nerves (ulnar at medial epicondyle, common peroneal at fibular head, radial at spiral groove) for swelling, nodularity (neuroma), tenderness, or thickening (as in CMT - "onion bulb" formation may make nerve palpably enlarged)
- Tinel's sign: Tapping over a nerve at the compression/injury site produces tingling/electrical sensation distally - indicates regenerating axons or entrapment
- Phalen's test: Wrist flexion 60 seconds reproduces carpal tunnel symptoms (median nerve)
- Adson's test, Wright's test, Roos test: Thoracic outlet syndrome provocative tests
- Muscle bulk/tenderness: Palpate target muscles for wasting, fibrosis, or tenderness
- Spine palpation: Paraspinal tenderness, trigger points, referred pain patterns
4. Motor Examination
| Grade | Description |
|---|---|
| 0 | No contraction |
| 1 | Flicker / trace contraction |
| 2 | Movement with gravity eliminated |
| 3 | Movement against gravity |
| 4 | Movement against resistance (sub-normal) |
| 5 | Normal strength |
| Nerve | Key Muscles Tested | Action Tested |
|---|---|---|
| Radial | ECRL, ECU, EDC, EPL | Wrist extension, finger extension, thumb extension |
| Median (low) | APB, FPB, opponens | Thumb abduction, opposition |
| Median (high) | FDP index/middle, FPL, pronator | Wrist flexion, FDP, pronation |
| Ulnar (low) | Interossei, ADM, FDM | Finger abduction/adduction |
| Ulnar (high) | FCU, FDP ring/little | Wrist ulnar deviation, ring/little DIP flexion |
| Axillary | Deltoid | Shoulder abduction 15-90° |
| Musculocutaneous | Biceps, brachialis | Elbow flexion, forearm supination |
| Long thoracic | Serratus anterior | Scapular protraction (wall push-up test) |
| Suprascapular | Supraspinatus, infraspinatus | Shoulder abduction (initiation), external rotation |
| Femoral | Quadriceps | Knee extension |
| Obturator | Hip adductors | Hip adduction |
| Common peroneal | Tibialis anterior, EHL, peronei | Dorsiflexion, eversion |
| Tibial | Gastrocnemius, soleus, toe flexors | Plantarflexion, toe flexion |
| Sciatic | All below knee + hamstrings | Knee flexion, all ankle/foot |
- Pinch strength (dynamometer) - median/ulnar
- Grip strength - median/ulnar
- Kapandji index - thumb opposition
- Key grip test - ulnar intrinsics
5. Sensory Examination
| Modality | Fiber Type | Tool |
|---|---|---|
| Light touch | A-beta | Cotton wool |
| Vibration | A-beta | 128 Hz tuning fork |
| Proprioception | A-beta | Passive joint movement |
| Pin-prick / pain | A-delta | Neurotip / pin |
| Temperature | C fibers | Hot/cold tubes |
- Absent / Diminished / Normal / Hypersensitive / Allodynia (pain from light touch)
- Two-point discrimination (static and moving) - normal fingertip: 2-4 mm static, 2-3 mm moving
- Semmes-Weinstein monofilaments: quantify pressure threshold; 4.17 = normal; 6.65 = deep pressure only; loss of protective sensation at >4.31
- Vibration threshold with biothesiometer
- Stocking-glove pattern = length-dependent polyneuropathy (diabetes, CMT, GBS)
- Dermatomal pattern = nerve root/radiculopathy
- Single nerve territory = mononeuropathy/entrapment
- Multiple mononeuropathies = mononeuritis multiplex (vasculitis, leprosy, diabetes)
6. Reflex Testing
| Reflex | Nerve Root | Test |
|---|---|---|
| Biceps | C5-C6 (musculocutaneous) | Tendon at antecubital fossa |
| Brachioradialis | C6 | Brachioradialis tendon |
| Triceps | C7 (radial) | Triceps tendon |
| Knee (patellar) | L2-L4 (femoral) | Patellar tendon |
| Ankle (Achilles) | S1-S2 (tibial) | Achilles tendon |
- GBS: global areflexia (early, even before weakness)
- CMT: absent Achilles reflexes early, later generalized areflexia
- Femoral nerve palsy: absent knee jerk
- Tibial/sciatic: absent ankle jerk
- Median/ulnar: absent finger jerks (rarely tested, but useful in high lesions)
- Bulbocavernosus reflex: S3-S4, pudendal nerve - critical for pudendal/lumbosacral assessment
- Anal wink reflex: S4-S5 - tests perianal sensation + sphincter motor arc
- Cremasteric reflex: L1-L2, genitofemoral nerve
7. Differential Diagnosis
| Diagnosis | Key Distinguishing Features |
|---|---|
| UMN lesion (stroke, MS, myelopathy) | Hyperreflexia, spasticity, positive Babinski, no significant atrophy early |
| Radiculopathy | Dermatomal sensory loss, positive SLR/ULTT, neck/back pain, imaging evidence |
| Plexopathy | Multiple nerve territories, may follow radiation/cancer/trauma |
| Myopathy | Proximal weakness, preserved sensation/reflexes, elevated CK |
| NMJ disorder (MG, LEMS) | Fatigability, preserved sensation and reflexes, decremental/incremental EMG |
| Motor neuron disease (ALS) | Mixed UMN + LMN signs, no sensory loss, fasciculations |
| CRPS | Allodynia, autonomic changes, vasomotor instability, disproportionate pain |
| Functional/psychogenic | Inconsistency on exam, "give-way" weakness, Hoover sign positive |
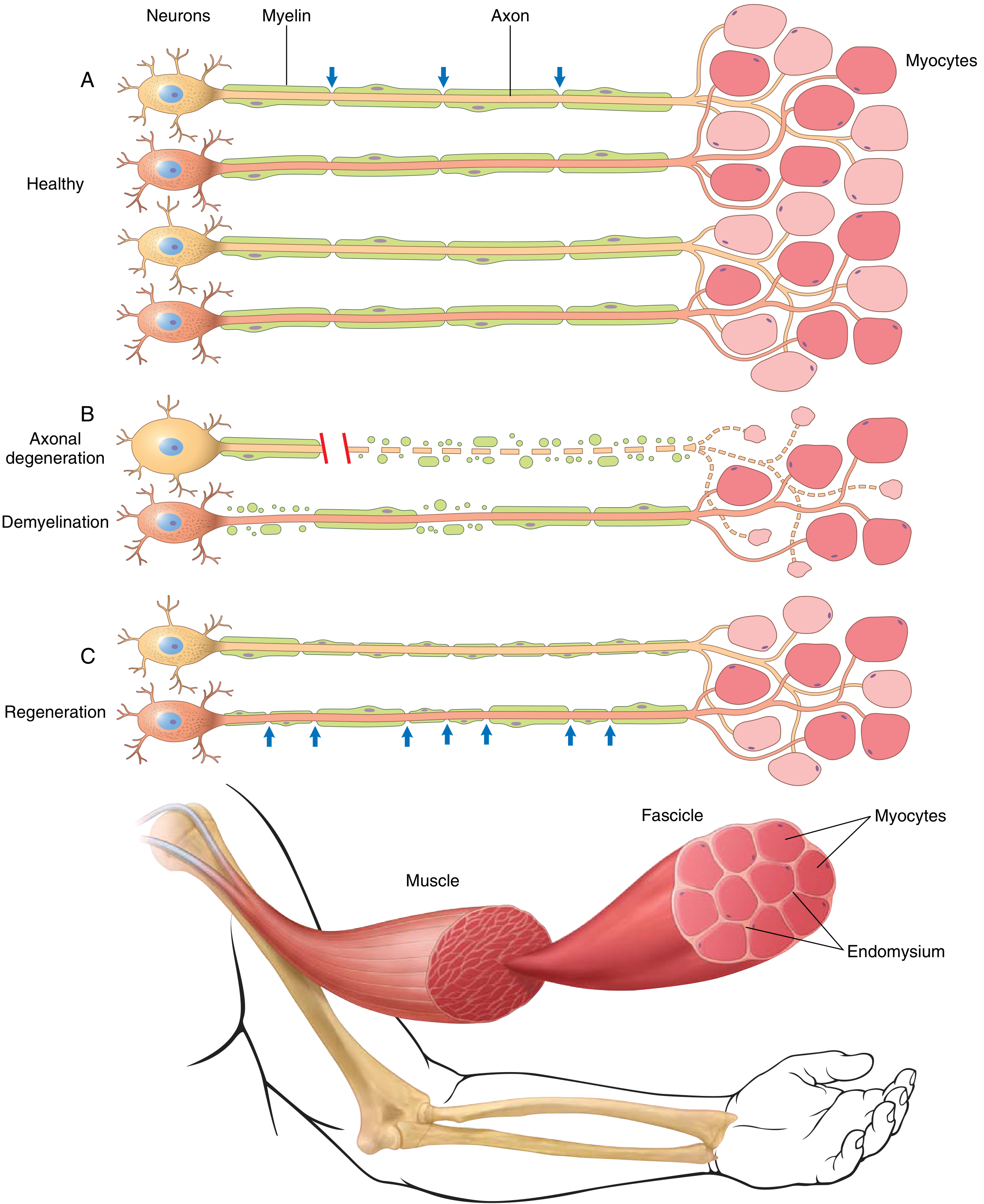
- Nerve Conduction Study (NCS): Demyelinating = slowed velocity, prolonged latency, conduction block; Axonal = reduced amplitude, preserved velocity
- EMG: Denervation signs (fibrillations, PSWs), reinnervation (polyphasic MUAPs) indicate axonal loss
- Somatosensory Evoked Potentials (SSEP): assess central vs. peripheral, useful in plexus injuries
- F-waves and H-reflexes: assess proximal nerve conduction (roots, plexus)
8. Balance and Coordination Examination
- Romberg test: Eyes open vs. closed - positive if loss of balance worsens with eyes closed (proprioceptive/sensory deficit)
- Tandem walking (heel-to-toe): Assesses coordination; impaired in sensory neuropathy
- Single-leg stance: Timed; affected side reveals deficits
- Fukuda stepping test: Assesses vestibular vs. proprioceptive balance
- Berg Balance Scale (BBS): 14-item; relevant in GBS recovery, sciatic/tibial nerve palsy
- Balance Master / force platform: measures center of pressure displacement
- Dynamic Posturography: differentiates vestibular vs. proprioceptive vs. visual balance contributions
- Finger-nose-finger test: intact in peripheral neuropathy (cerebellar lesions positive)
- Heel-shin test: affected in sensory neuropathy (proprioceptive ataxia)
- Diadochokinesis: generally intact in peripheral nerve lesions
9. Gait Analysis
| Nerve Affected | Characteristic Gait Pattern |
|---|---|
| Common peroneal | Foot drop - steppage gait (excessive hip/knee flexion to clear foot); equinovarus posture |
| Tibial | Inability to push off; calcaneal gait; impaired stance phase |
| Sciatic | Combined foot drop + weak knee flexion; Trendelenburg if hip also affected |
| Femoral | Knee buckling in stance; compensates by trunk lean or hand on thigh |
| Obturator | Abductor lurch; scissor gait if bilateral |
| Long thoracic | Scapular winging; altered upper limb swing |
| GBS (recovery) | Wide-based, ataxic gait; steppage pattern |
| CMT | High-stepping gait; pes cavus; stocking distribution sensory loss |
- Observational Gait Analysis (OGA): video recording, 2D
- 3D Motion capture (Vicon, OptiTrack): quantitative kinematics
- Wearable accelerometers: community ambulators
- Timed 10-Meter Walk Test (10MWT), 6-Minute Walk Test (6MWT): functional measures
- Dynamic EMG: identifies timing/pattern of muscle activation during gait
10. Functional Analysis
- Upper limb: pinch, grip, writing, dressing, feeding, tool use
- Lower limb: stairs, uneven terrain, community ambulation
- Respiratory: tidal volume, vital capacity (phrenic/intercostal lesions)
- Sphincter function: bladder/bowel control (pudendal, lumbosacral plexus)
- DASH/QuickDASH: Disabilities of Arm, Shoulder, and Hand
- Michigan Hand Questionnaire (MHQ): Hand-specific functional outcomes
- Functional Independence Measure (FIM): Global ADL assessment
- Barthel Index: ADL independence
- GBS Disability Scale: GBS-specific functional grading
- Foot and Ankle Disability Index (FADI): Lower limb neuropathy
- Motricity Index: Quantifies motor recovery post-nerve injury
11. Problems and Complications
- Muscle weakness/paralysis
- Muscle wasting/atrophy (denervation)
- Contractures from muscle imbalance
- Joint instability (paralytic subluxation - e.g., shoulder in axillary palsy)
- Sensory loss (loss of protective sensation)
- Neuropathic pain (burning, dysesthesia, allodynia, hyperalgesia)
- Trophic ulcers from insensate skin
- Loss of fine motor skills, grip, pinch
- Impaired gait and mobility
- Falls risk (proprioceptive loss + weakness)
- Impaired ADLs
- Respiratory failure (GBS, phrenic nerve palsy, intercostal nerve lesions)
- Autonomic dysfunction (GBS): arrhythmia, BP instability, ileus, bladder dysfunction
- Deep vein thrombosis (DVT) in immobile patients
- Pressure sores / decubitus ulcers
- Psychological: depression, anxiety, adjustment disorder
- Contractures (wrist flexion in radial nerve palsy, equinus in common peroneal palsy)
- Joint malalignment (shoulder subluxation, foot deformity)
- Tendon shortening / adhesions
- Edema of denervated limb
- Skin breakdown
12. Goal Setting
- Prevent deformity and contracture with splinting/orthotics
- Prevent pressure ulcers with sensory precautions
- Reduce pain and edema
- Maintain ROM of affected joints
- Protect regenerating nerve (activity modification)
- Respiratory: maintain airway/ventilation (GBS)
- Patient education: skin care, positioning, activity precautions
- Maximize motor and sensory recovery
- Re-educate recovered muscles for functional use
- Achieve independent ADLs
- Return to occupation/sport
- Optimize compensatory strategies where recovery is incomplete
- Vocational rehabilitation and community reintegration
- Provide definitive orthosis/adaptive equipment if permanent deficit
PART II: MANAGEMENT
13. Management of Systemic Complications
- Serial bedside spirometry (FVC, FEV1) - especially GBS, phrenic nerve palsy
- Intubate if FVC <20 mL/kg or rapidly declining (GBS)
- Incentive spirometry, IPPB, and manual chest physiotherapy
- Glossopharyngeal breathing for high-level respiratory compromise
- BiPAP/NIV support in subacute phase; diaphragmatic re-training in recovery
- Cardiac monitoring for arrhythmias
- Cautious positioning for orthostatic hypotension (head-up tilt protocol)
- Bowel program for neurogenic bowel (timing, dietary fiber, laxatives)
- Bladder management: intermittent catheterization for neurogenic bladder
- Thermoregulation support (impaired sweating in autonomic neuropathy)
- Pneumatic compression devices
- LMWH (pharmacological prophylaxis per physician)
- Active + passive limb exercises; early mobilization
- Thiamine (B1), B6, B12 supplementation in deficiency neuropathies
- Protein optimization for axon regeneration
- Neuropathic pain: gabapentin, pregabalin (first-line); duloxetine, amitriptyline
- TENS for pain modulation
- Desensitization program for allodynia/hyperalgesia
14. Management of Mechanical Complications
- Radial nerve palsy: Wrist cock-up splint (dynamic or static) - maintains functional position, prevents contracture
- Median nerve palsy (low): Opponens splint - maintains thumb opposition
- Ulnar nerve palsy: Anti-claw splint (lumbrical bar) - blocks MCP hyperextension in ring/little fingers
- Common peroneal palsy: AFO (ankle-foot orthosis) - prevents foot drop, enables heel-strike gait
- Brachial plexus / axillary palsy: Shoulder sling or humeral cuff - prevents inferior subluxation
- Sciatic nerve palsy: Combined AFO + knee orthosis as needed
- Daily passive ROM exercises through full range
- Prolonged stretch with serial casting or dynamic splints
- Heat before stretching (ultrasound, warm wax bath)
- Splinting at end-range position during rest
- Elevation of denervated limb
- Retrograde massage
- Compression bandaging/gloves
- Contrast baths (cautious in insensate limbs)
- Regular visual inspection of insensate areas
- Protective footwear/padding
- Pressure offloading for trophic ulcers
- Moist wound healing principles
- Begin active-assisted exercise when MMT grade 2 appears
- Progress to active and resisted exercise with grading
- Functional task-specific training
- Biofeedback-assisted muscle reeducation
15. Neurophysiological Approaches and Modalities
- Neuromuscular Electrical Stimulation (NMES/FES): Delays denervation atrophy; stimulates reinnervated muscle once NMJ re-established
- Transcutaneous Electrical Nerve Stimulation (TENS): Pain relief via gate control (conventional/high frequency) or endorphin release (low-frequency acupuncture-type)
- Percutaneous Electrical Neural Stimulation: Brief intraoperative or perioperative electrical stimulation enhances axon regeneration (current evidence: 20 Hz, 1 hour of continuous intraoperative stimulation shown to accelerate reinnervation)
- Interferential Therapy (IFT): Deep penetrating current; pain relief and circulation
- Pulsed therapeutic ultrasound: promotes Schwann cell proliferation, upregulates NGF, reduces inflammation at injury site
- Parameters: 0.5-1 MHz (deep nerve), 0.3-0.5 W/cm², pulsed mode (1:4), 5-10 min
- Evidence supports acceleration of peripheral nerve regeneration in animal and early human studies
- Wavelengths 600-1000 nm activate mitochondrial cytochrome c oxidase
- Promotes axon sprouting, reduces oxidative stress, improves Schwann cell function
- Application over nerve trunk and target muscle; doses 1-4 J/cm²
- Growing evidence in carpal tunnel syndrome (median nerve), facial nerve palsy
- Pulsed electromagnetic fields (PEMF): enhance nerve regeneration in animal models
- Clinically used for neuropathic pain management
- rTMS of motor cortex: cortical reorganization following peripheral nerve injury; applied in complex regional pain syndrome
- Irradiation principle: strong patterns from intact muscles elicit overflow into weak denervated muscles
- Techniques: Hold-Relax, Contract-Relax, Rhythmic Stabilization
- Diagonal patterns (D1/D2 flexion-extension) facilitate nerve-territory muscles
- Useful when reinnervation begins (MMT 1-2); progresses with recovery
- Facilitation techniques: brushing, icing, tapping over muscle belly - facilitate alpha motor neuron via cutaneous afferents
- Inhibition: maintained pressure, slow stroking, prolonged icing - reduce hypertonicity in antagonists
- Application in re-education of reinnervated muscles
- Early phase (when protective sensation returns): Graded desensitization using textures from least to most stimulating (cotton, towel, Velcro, rice)
- Late phase (when moving touch/localization return): Object recognition training, texture discrimination, two-point discrimination training
- Mirror therapy: used in chronic peripheral nerve pain / CRPS type II
- Constraint-induced movement therapy (CIMT): adapted for hand nerve injuries
- Warm water reduces muscle spasm and pain; buoyancy enables active exercise with gravity elimination
- Particularly useful in GBS rehabilitation, bilateral lower limb peripheral neuropathy
- Turbine (whirlpool) for wound healing and sensory stimulation
- EMG biofeedback: real-time muscle activity display - trains patient to activate reinnervated muscles
- Threshold-based training: patient tries to exceed minimal contraction threshold
- Effective when clinical EMG shows nascent motor unit potentials (MUPs)
PART III: SPECIFIC CONDITIONS
16. Hereditary Motor Sensory Neuropathy (HMSN / Charcot-Marie-Tooth Disease)
- Most common inherited neuropathy; prevalence ~1 in 2,500
- Mutations in >80 genes affecting Schwann cell membrane proteins (PMP22, MPZ, Cx32), axonal cytoskeleton (NEFL), and mitochondrial proteins (MFN2)
- CMT1 (HMSN-I): demyelinating type - markedly reduced NCV (<38 m/s ulnar); onion bulb formation on nerve biopsy; most commonly CMT1A (PMP22 duplication)
- CMT2 (HMSN-II): axonal type - near-normal NCV, reduced amplitudes; axonal loss on biopsy
- CMTX: X-linked; intermediate conduction velocities (35-45 m/s)
- Dejerine-Sottas Disease (formerly CMT3): severe early-onset demyelinating; NCV <10 m/s
- Onset: adolescence to young adulthood (CMT1), later in CMT2
- Peroneal muscular atrophy: foot/leg wasting; "inverted champagne bottle" or "stork leg" appearance
- Pes cavus + hammer toes + high arched feet (long-standing denervation-reinnervation)
- Distal > proximal weakness (foot drop, steppage gait)
- Stocking-glove sensory loss; proprioception often reduced
- Achilles reflexes: absent early; generalized areflexia later
- Palpably enlarged peripheral nerves (demyelinating forms)
- Scoliosis in severe cases
- Ankle-foot orthoses (AFOs): prevent foot drop, improve gait efficiency
- Strengthening: ankle dorsiflexors, invertors; resistance exercises for remaining function
- Stretching: Achilles tendon lengthening (equinus contracture prevention)
- Balance training: proprioceptive retraining on foam/wobble board
- Aquatic therapy: enables exercise with buoyancy support
- Footwear modification + orthotics: metatarsal pads, cushioned soles
- Energy conservation strategies (progressive fatigue is common)
- Vocational adaptation
17. Guillain-Barré Syndrome (GBS)
- Acute immune-mediated polyneuropathy; incidence 1-2 per 100,000/year
- Molecular mimicry: preceding infection (Campylobacter jejuni, CMV, EBV, Zika) triggers autoantibodies against peripheral nerve gangliosides
- Subtypes:
- AIDP (Acute Inflammatory Demyelinating Polyneuropathy): most common in Europe/North America
- AMAN (Acute Motor Axonal Neuropathy): motor axon attack; common in Asia
- AMSAN: motor + sensory axonal; severe, poor recovery
- Miller-Fisher Syndrome (MFS): ophthalmoplegia + ataxia + areflexia; anti-GQ1b antibody
- Required: progressive weakness of both legs and arms + areflexia/hyporeflexia
- Supportive: progression over days to 4 weeks, relative symmetry, mild sensory signs, bifacial palsies, autonomic dysfunction, absent fever at onset
- Lab: elevated CSF protein with <10 cells/µL (albuminocytological dissociation); NCS shows slowing/conduction block (AIDP) or amplitude reduction (axonal)
- Acute phase (peak dysfunction): days to 4 weeks
- Plateau phase
- Recovery phase: weeks to months; 80% recover functional ambulation; mortality 1-5%
- IVIG: 2 g/kg over 5 days - equivalent to plasmapheresis
- Plasmapheresis (PE): 5 exchanges over 2 weeks - indicated in non-ambulatory GBS
- Do NOT use corticosteroids (no benefit, may worsen outcome)
- Mechanical ventilation if FVC <20 mL/kg or rapidly declining (10-30% require ICU)
- Passive ROM to prevent contractures (hip/knee/ankle)
- Positioning: anti-contracture, pressure relief every 2 hours
- Respiratory physiotherapy: IPPB, suctioning, manual hyperinflation in ventilated patients
- Venous compression devices (DVT prophylaxis)
- Splinting: AFO for foot drop, wrist splints as needed
- Progressive active-assisted to active to resisted exercises as reinnervation proceeds
- PNF techniques: irradiation from strong proximal muscles to recovering distal ones
- Hydrotherapy: early ambulation and exercise with buoyancy
- Balance and gait re-education: parallel bars → walking frame → cane → independent
- Fatigue management: energy conservation; graduated return to activity
- Berg Balance Scale and 6MWT to track progress
- Respiratory rehabilitation: diaphragmatic breathing, incentive spirometry post-extubation
- Psychological support: anxiety/depression common in prolonged GBS recovery
18. Brachial Plexus Palsy
- Roots: C5-T1; Trunks (upper C5-C6, middle C7, lower C8-T1); Divisions; Cords (lateral, posterior, medial); Terminal branches
- Upper plexus (Erb-Duchenne palsy): C5-C6 lesion; "waiter's tip" posture - shoulder adducted/internally rotated, elbow extended, forearm pronated; deltoid, biceps, brachialis, supraspinatus, infraspinatus affected
- Lower plexus (Klumpke's palsy): C8-T1; intrinsic hand muscles + finger flexors; claw hand; Horner's syndrome (stellate ganglion involvement: ptosis, miosis, anhidrosis)
- Total plexus: C5-T1 - flail anesthetic limb
- Preganglionic vs. Postganglionic: Preganglionic (avulsion) - Tinel's negative, NCS: preserved SNAP with absent CMAP, normal EMG in paraspinals; rhomboids/serratus affected. Postganglionic - Tinel's positive, SNAP absent.
- Shoulder sling/arm support: prevent subluxation and stretch
- Passive ROM: prevent capsular contracture (especially shoulder external rotation + abduction)
- Splinting: wrist/hand splints for hand function
- PNF patterns: D2 flexion pattern engages C5-C6 muscles (upper plexus)
- FES: NMES to deltoid, biceps in upper plexus injury
- Sensory re-education for returning sensation
- Mirror therapy / mental imagery: enhances cortical reorganization
- Post-surgical rehabilitation: nerve grafts, tendon transfers, free muscle transfers
19. Thoracic Outlet Syndrome (TOS)
- Neurogenic TOS (95%): Lower trunk/medial cord (C8-T1) most commonly; ulnar distribution symptoms; wasting of intrinsic hand muscles (true neurogenic TOS - rare)
- Venous TOS: Effort thrombosis (Paget-Schroetter); upper limb swelling, cyanosis
- Arterial TOS: Rarest; cervical rib present; embolic complications
- Roos test (EAST): arm elevation + open/close hand 3 min - reproduces symptoms
- Adson's test: radial pulse obliteration with head turned to ipsilateral side + deep breath (low sensitivity)
- Wright's test: radial pulse obliteration with shoulder hyperabducted at 180°
- Halstead maneuver: clavicular traction with neck laterally flexed to opposite side
- Posture correction: forward head posture + depressed shoulder posture correction
- Scalene and pectoralis minor stretching
- Strengthening: lower trapezius, serratus anterior, deep cervical flexors
- Rib 1 mobilization (manipulation)
- Neural mobilization (median + ulnar nerve sliding techniques)
- Ergonomic advice: workstation, lifting technique
- Breathing pattern retraining (diaphragmatic breathing to reduce scalene overactivity)
20. Lumbosacral Plexus Lesions
- Femoral nerve territory: quadriceps weakness, diminished knee jerk, anterior thigh/medial leg sensory loss
- Obturator nerve territory: hip adductor weakness
- Iliohypogastric/Ilioinguinal: groin/inguinal sensory disturbance
- Sciatic territory: hamstrings, all muscles below knee
- Superior/Inferior gluteal: hip abductors, extensors
- Pudendal: perineal, bladder, bowel, sexual dysfunction
- Identify and address cause; manage neuropathic pain
- Lower limb strengthening: quadriceps, hip stabilizers
- AFO for foot drop component
- Pelvic floor physiotherapy (if pudendal/S3-S4 involvement)
- Gait retraining
- Hydrotherapy for early mobility
21. Phrenic and Intercostal Nerve Lesions
- Unilateral injury: elevated hemidiaphragm; paradoxical movement on CXR fluoroscopy; dyspnea on exertion + lying flat
- Bilateral injury: severe respiratory compromise requiring ventilatory support
- Causes: cardiac surgery (topical cooling), trauma, malignancy (Pancoast), cervical spine surgery, birth trauma
- Management: Respiratory physiotherapy: accessory muscle training (scalenes, intercostals, SCM); glossopharyngeal breathing; diaphragm pacing (electrical) for bilateral phrenic injury; non-invasive ventilation (BiPAP)
- Causes: rib fractures, thoracotomy (post-thoracotomy pain syndrome), herpes zoster (post-herpetic neuralgia), thoracic surgery
- Signs: band-like intercostal neuralgia; chest wall hypoesthesia; paradoxical breathing if multiple levels
- Management: TENS over affected dermatomal strip; intercostal nerve block (lidocaine); breathing exercises; postural correction; gabapentin/pregabalin for post-herpetic neuralgia
22. Median Nerve Palsy
- Pronator teres, FCR, FDS affected
- FDP to index + middle, FPL (FPL test: Okay sign loss; index FDP loss)
- All thenar muscles + lateral 2 lumbricals
- "Orator's hand" or "hand of benediction" on attempted fist - index/middle remain extended
- Thenar wasting (APB, opponens, FPB)
- Loss of thumb palmar abduction and opposition
- Sensory: lateral 3.5 digits (palmar surface), index/middle fingertip = most sensitive indicator
- Ape hand deformity: thumb adducted in plane of palm
- Phalen's test (wrist flexion 60 sec), Tinel's at carpal tunnel, Durkan compression test
- Night splint in neutral wrist position (CTS)
- Neural gliding exercises (median nerve slider/tensioner)
- Thenar muscle strengthening on reinnervation
- Opponens splint: maintains functional pinch position
- Sensory re-education
- Ergonomic modification for occupational CTS
- LLLT over carpal tunnel: evidence supports reduction of CTS symptoms
23. Ulnar Nerve Palsy
- FCU + FDP ring/little affected
- All intrinsics (interossei, hypothenar, medial 2 lumbricals) affected
- Sensation: little finger, medial ring finger (both dorsal + palmar), medial palm, medial dorsum of hand
- All intrinsics except FCU + FDP
- Sensation: palmar ulnar zone only
- "Claw hand" deformity: ring + little fingers in MCP hyperextension + IP flexion (more severe at wrist - "ulnar paradox": high lesions less clawed because FDP also weak)
- Froment's sign: FPL compensates for adductor pollicis weakness when gripping paper
- Jeanne's sign: MCP hyperextension of thumb with paper grip
- Wartenberg's sign: little finger abducted (EDM unopposed)
- Card test: cannot hold card between fingers (weak interossei)
- Anti-claw splint (lumbrical bar): block MCP hyperextension of ring/little
- Elbow padding (cubital tunnel): protect nerve at elbow
- Nerve gliding exercises: ulnar nerve
- Intrinsic strengthening on reinnervation
- Froment's sign reduces as adductor pollicis recovers
- Sensory re-education
24. Radial Nerve Palsy
- Triceps weak + absent triceps reflex
- Brachioradialis weak
- Wrist drop + finger extension loss
- Sensory: posterior arm, lateral dorsal forearm, dorsal lateral 3.5 digits
- Triceps relatively spared (its branches arise proximal to spiral groove)
- Wrist drop (ECRL/ECU), finger drop (EDC, EIP)
- Sensory: dorsal lateral forearm (LABC) + dorsal lateral hand (superficial radial)
- No sensory loss (purely motor)
- No wrist drop (ECRL intact)
- Finger/thumb extension loss (EDC, EIP, EPL)
- Wrist deviates radially on extension (ECU weak, ECRL intact)
- Inability to extend wrist + fingers = high/spiral groove
- Finger drop without wrist drop = PIN syndrome
- Weakness reproduces with resisted supination (radial tunnel entrapment)
- Wrist cock-up splint (dynamic extension splint preferred): restores functional grasp
- Prevent web space contracture: thumb web splint
- Electrical stimulation to maintain muscle bulk
- Re-education exercises when reinnervation occurs
- Radial nerve gliding/mobilization
- Heat/ultrasound over spiral groove (for entrapment/edema)
25. Musculocutaneous Nerve Palsy
- Elbow flexion weakness (especially in supination)
- Supination weakness (biceps is the main supinator)
- Sensory loss: lateral forearm
- Biceps reflex absent
- Elbow flexion orthosis if severely weak: gravity-assisted spring-loaded orthosis
- Strengthening brachioradialis (radial nerve, C6) as functional elbow flexor substitute
- PNF: D2 flexion pattern (involves elbow flexion)
- Sensory re-education over lateral forearm
26. Anterior Interosseous Nerve (AIN) Palsy
- No sensory loss (purely motor)
- Loss of IP flexion of thumb (FPL) and DIP flexion of index/middle (FDP)
- Pinch deformity: Patient cannot make OK sign - both thumb IP and index DIP extend instead of flex (square pinch pattern)
- Weakness of forearm pronation (pronator quadratus)
- Most recover spontaneously within 6-12 months (neuralgic amyotrophy)
- Rest, avoid forceful pronation
- Tenodesis splint to assist pinch
- Monitor with serial EMG for reinnervation
27. Posterior Interosseous Nerve (PIN) Palsy
28. Axillary Nerve Palsy
- Shoulder abduction weakness (deltoid): loss of 15-90° arc primarily
- External rotation weakness (teres minor - mild)
- Sensory loss: "regimental badge" area = lateral deltoid patch
- Shoulder girdle flatness/dimpling from deltoid atrophy
- Risk of inferior subluxation of glenohumeral joint
- Sling for shoulder support: humeral cuff sling (not collar and cuff - inferior subluxation risk)
- Passive ROM: full shoulder range, especially external rotation/abduction
- NMES to deltoid: maintains muscle bulk during denervation
- Progressive shoulder strengthening: start with shoulder shrugs (trapezius), scapular stabilizers, then deltoid retraining
- Functional shoulder exercises in pool (buoyancy assists)
- Proprioceptive training to restore shoulder stability
29. Long Thoracic Nerve Palsy
- Medial winging of scapula: medial border + inferior angle lift away from thorax
- Winging worsens with forward flexion against wall (push-up position)
- Shoulder abduction limited above 90° (serratus needed for upward rotation beyond 90°)
- Shoulder pain from altered scapulohumeral rhythm
- Scapular brace/orthosis: holds scapula against thorax
- Strengthening serratus anterior on reinnervation: "serratus punches," wall push-ups progressing to floor push-ups
- Compensatory training: lower trapezius strengthening
- Postural correction: avoid protracted shoulders
- Most cases: spontaneous recovery in 6-24 months; prognosis generally good
30. Suprascapular Nerve Palsy
- Supraspinatus + infraspinatus atrophy (visible above and below spine of scapula)
- Isolated infraspinatus wasting if compression at spinoglenoid notch (overhead athletes)
- External rotation weakness (infraspinatus)
- Shoulder abduction initiation weakness (supraspinatus)
- Shoulder/lateral neck pain
- Identify and treat cause (ganglion cyst: aspiration or surgery)
- Shoulder external rotation strengthening with theraband
- Rotator cuff rehabilitation protocol
- Scapular stabilization
- Overhead activity modification
31. Sciatic Nerve Palsy
- Combined common peroneal + tibial territory weakness
- Hamstrings may be weak (knee flexion)
- Foot drop + plantarflexion weakness (complete high lesion)
- Sensory: entire foot + lower leg (except medial strip = saphenous/femoral)
- Absent ankle jerk
- Note: Peroneal division of sciatic is more vulnerable (less intraneural connective tissue)
- AFO: foot drop
- Stretching: Achilles tendon, hip flexors
- Strengthening: hip extensors (gluteus maximus), hamstrings, all calf + foot muscles on recovery
- Gait re-education
- Sensory re-education for foot (high ulceration risk)
- Pain management: gabapentin/pregabalin for sciatic neuropathic pain
32. Tibial Nerve Palsy
- Plantarflexion + toe flexion weakness
- Calcaneal gait (heels strikes, unable to push off)
- Foot/toe flexor intrinsic wasting (intrinsic minus foot)
- Claw toes
- Sensory: sole of foot + heel (plantar surface); great toe tip
- Tarsal tunnel: burning + tingling in sole/plantar aspect; Tinel's at medial malleolus
- Tarsal tunnel syndrome: night splint in neutral, orthotics to reduce pronation, corticosteroid injection, neural mobilization
- Calcaneal gait: AFO with heel cushioning; shoe modification
- Strengthening: tibialis posterior, toe flexors on reinnervation
- Trophic foot care: plantar insensate skin is high ulceration risk
33. Common Peroneal Nerve Palsy
- Foot drop: Weak dorsiflexion (TAS = tib anterior sign - unable to walk on heels)
- Eversion weakness: Weak peronei
- Equinovarus deformity: Inversion (tibialis posterior unopposed) + plantarflexion
- Steppage gait
- Sensory: dorsum of foot, first web space (deep peroneal), lateral leg/dorsal foot (superficial peroneal)
- Ankle jerk preserved (tibial nerve intact)
- AFO (drop-foot splint): dorsiflexion assist, prevents equinus contracture
- Daily passive dorsiflexion + eversion stretching
- Strengthening tibialis anterior, EHL, peronei on reinnervation
- Gait re-education with AFO
- FES to tibialis anterior (peroneal nerve stimulator): real-time dorsiflexion assist during walking
- Padding over fibular head to prevent recurrence
- Neural mobilization: common peroneal nerve at fibular head
34. Femoral Nerve Palsy
- Quadriceps weakness: knee buckles on weight-bearing; patient compensates with trunk lean forward or hyperextends knee passively
- Absent knee jerk
- Sensory: anterior thigh + medial leg + medial foot (saphenous)
- Hip flexion relatively preserved if injury distal to inguinal ligament (psoas intact)
- Knee immobilizer or KAFO (knee-ankle-foot orthosis): prevents knee buckling in gait
- Quadriceps strengthening: isometric, then isotonic, then functional (SLR, step-ups)
- EMG biofeedback for quadriceps recruitment
- Gait re-education: compensatory strategies initially
- Address cause (anticoagulant review, abscess drainage)
35. Obturator Nerve Palsy
- Hip adductor weakness: impaired hip adduction and internal rotation
- Scissor gait tendency
- Sensory: medial thigh (variable)
- Trendelenburg pattern absent (gluteus medius intact)
- Hip adductor strengthening on reinnervation
- Gait training: prevent excessive lateral sway
- Stretching hip abductors (antagonists may tighten)
- Address precipitating cause
36. Pudendal Nerve Palsy
- Perineal numbness + paresthesias
- Erectile dysfunction / reduced clitoral sensation
- Urinary incontinence (urethral sphincter weakness) or retention
- Fecal incontinence (external anal sphincter)
- Absent bulbocavernosus reflex
- Absent anal wink reflex
- Pelvic floor physiotherapy: biofeedback-assisted sphincter re-education
- Bladder training program: scheduled voiding, pelvic floor exercises
- Interferential therapy to perineum: pain relief + neuromuscular stimulation
- Positions: avoid prolonged sitting (pressure off pudendal canal)
- Specialist cycling saddle modification
- Pudendal nerve block (diagnostic + therapeutic)
- SNS (Sacral Nerve Stimulation) for refractory cases
PART IV: QUICK REFERENCE SUMMARY TABLE
| Condition | Deformity | Motor Loss | Sensory Loss | Key Test | Splint |
|---|---|---|---|---|---|
| Radial nerve (spiral groove) | Wrist drop | Wrist + finger extension | Dorsal forearm + hand | Inability to extend wrist | Wrist cock-up |
| Median nerve (low - CTS) | Ape hand | Thumb abduction/opposition | Lateral 3.5 digits palm | Phalen's, Tinel's, Durkan | Wrist neutral night splint |
| Ulnar nerve (low) | Claw hand (ring/little) | Intrinsics, hypothenar | Medial 1.5 digits | Froment, card test | Anti-claw lumbrical bar |
| Axillary nerve | Deltoid atrophy | Shoulder abduction | Lateral deltoid patch | Deltoid MMT | Arm sling |
| Long thoracic | Medial scapular winging | Serratus anterior | Nil | Wall push-up | Scapular brace |
| Musculocutaneous | - | Elbow flexion/supination | Lateral forearm | Biceps reflex absent | Elbow flexion assist |
| Common peroneal | Foot drop/equinovarus | Dorsiflexion, eversion | Dorsum of foot | Walk on heels (TAS) | AFO |
| Tibial | Calcaneal gait | Plantarflexion, toe flexion | Plantar foot | Tinel's at medial malleolus | AFO (heel cushion) |
| Femoral | Knee buckling | Quadriceps | Anterior thigh, medial leg | Knee jerk absent | KAFO |
| Sciatic | Foot drop + plantarflexion | Hamstrings + all below knee | Entire foot (except medial) | - | AFO ± knee support |
KEY REFERENCES
- Patterns of peripheral nerve injury, axonal vs. demyelinating neuropathy: Robbins & Kumar Basic Pathology, 10e
- Hereditary Motor Sensory Neuropathy (CMT): Bradley and Daroff's Neurology in Clinical Practice
- Guillain-Barré Syndrome - diagnostic criteria and subtypes: Bradley and Daroff's Neurology in Clinical Practice
- Physical therapy modalities for peripheral nerve injury (ultrasound, LLLT, ES): Frontiers in Neurology, 2025 review
- Thoracic outlet syndrome anatomy and management: Sabiston Textbook of Surgery, 21e
Mnd
motor neuron disease ALS types pathophysiology clinical features management 2024 guidelines
motor neuron disease physiotherapy management respiratory riluzole tofersen 2024
Motor Neuron Disease (MND) - Full Study Notes
1. OVERVIEW AND DEFINITION
- Charcot disease (first described by Jean-Martin Charcot, 1869)
- Lou Gehrig's disease (USA - after the baseball player diagnosed in 1939)
2. EPIDEMIOLOGY
| Parameter | Data |
|---|---|
| Incidence | ~2 per 100,000/year |
| Prevalence | 5-8 per 100,000 |
| Mean age of onset | 55-60 years |
| Sex ratio | Male:Female = 1.2-1.6:1 (slight female predominance in bulbar onset) |
| Familial vs. sporadic | ~90% sporadic (SALS); 5-10% familial (FALS) |
| Median survival | 3 years from symptom onset (range: 2-5 years; some 10+ years) |
| Mortality | Invariably fatal; respiratory failure is the usual cause |
3. TYPES / CLINICAL VARIANTS
3.1 Classic ALS (Most Common - 80%)
- Combined UMN + LMN degeneration
- Affects all four limbs and bulbar musculature
- Spinal onset (75%): asymmetric distal limb weakness; foot drop or hand wasting
- Bulbar onset (25%): dysarthria, dysphagia, dysphonia first
3.2 Progressive Bulbar Palsy (PBP)
- LMN predominant involving cranial motor nuclei (IX, X, XII)
- Flaccid dysarthria, dysphagia, tongue wasting + fasciculations
- Pseudobulbar palsy component (UMN) superimposed: emotional lability, brisk jaw jerk, spastic dysarthria
- Worst prognosis of all MND variants; rapid respiratory compromise
3.3 Primary Lateral Sclerosis (PLS)
- Pure UMN degeneration only
- Progressive spastic paraparesis / tetraparesis
- Hyperreflexia, spasticity, Babinski sign; NO wasting or fasciculations
- Most benign variant: slower progression, longer survival (10+ years)
- Diagnosis of exclusion; 10-15% eventually develop LMN signs and reclassify as ALS
3.4 Progressive Muscular Atrophy (PMA)
- Pure LMN degeneration (anterior horn cells)
- Flaccid weakness, wasting, fasciculations; areflexia
- NO UMN signs; resembles SMA in adults
- Intermediate prognosis; most eventually develop UMN signs
- Must exclude Kennedy disease, multifocal motor neuropathy, SMA
3.5 Flail Arm / Flail Leg Syndrome (Brachial / Crural Amyotrophy)
- Flail arm (Vulpian-Bernhart): bilateral proximal arm weakness + wasting; legs and bulbar spared initially
- More common in men; longer survival than typical ALS
- Flail leg syndrome: bilateral distal leg weakness (foot drop)
3.6 Kennedy Disease (Bulbospinal Muscular Atrophy)
- X-linked; CAG repeat expansion in androgen receptor gene
- Men only; LMN only (no UMN signs)
- Proximal limb weakness, oropharyngeal weakness, gynecomastia, infertility
- Key ALS mimic - distinguished by androgen receptor testing
3.7 Spinal Muscular Atrophy (SMA) - Related LMN Disorders
| Type | Onset | Features | Prognosis |
|---|---|---|---|
| SMA I (Werdnig-Hoffmann) | Preterm - 6 months | Floppy baby, cannot sit | Few survive 1 year |
| SMA II (Dubowitz) | 6-15 months | Cannot stand | Variable; respiratory |
| SMA III (Kugelberg-Welander) | 1 yr - adolescence | Proximal leg weakness | Slowly progressive |
| SMA IV | After 30 years | Proximal + diaphragm | Wheelchair; normal life span |
4. PATHOPHYSIOLOGY
4.1 Genetics
- 90% sporadic - unknown cause; complex interaction of genetic susceptibility + environment
- C9ORF72 hexanucleotide (GGGGCC) repeat expansion: most common genetic cause; accounts for 40-50% of familial ALS and 7-10% of sporadic ALS
- Defective RNA processing: RNA foci sequester RNA-binding proteins; dipeptide repeat proteins are neurotoxic
- SOD1 (Superoxide dismutase 1) mutations on chromosome 21: 20% of familial ALS (2% overall)
- Misfolded SOD1 proteins trigger unfolded protein response + prion-like propagation
- Oxidative stress, excitotoxicity, mitochondrial dysfunction, impaired axonal transport
- TDP-43 (TARDBP gene): RNA-binding protein; abnormal cytoplasmic inclusions are the hallmark of most ALS (both sporadic and familial); also in frontotemporal lobar degeneration (FTLD)
- FUS (FUS/TLS gene): another RNA-binding protein; associated with juvenile ALS
- Other genes: ALSIN, senataxin, angiogenin, VAPB, dynactin, TBK1, ataxin-2 intermediate repeats
4.2 Pathogenic Mechanisms
- Excitotoxicity: excess glutamate → Ca²⁺ influx → neuronal death (basis for riluzole)
- Oxidative stress: mutant SOD1 → reactive oxygen species
- Protein aggregation: TDP-43, SOD1, FUS inclusions disrupt normal cell function
- Mitochondrial dysfunction: impaired energy supply to high-demand motor neurons
- Neuroinflammation: activated microglia + astrocytes accelerate neuronal injury
- Impaired axonal transport: motor neurons are extremely long; transport defects are catastrophic
4.3 Pathology (Morphology)
- Macroscopic: Atrophy of precentral gyrus (motor cortex); sclerosis and pallor of lateral corticospinal tracts; thinning of ventral (anterior) spinal nerve roots and hypoglossal nerves; visible muscle wasting
- Microscopic: Loss of anterior horn cells (>50% lost by time of death); reactive astrocytic gliosis in spinal cord gray matter; TDP-43 cytoplasmic inclusions; neurogenic atrophy of skeletal muscle (grouped fiber atrophy)
- Spared: Onuf's nucleus (sacral sphincter motor neurons - explains preserved continence); extraocular muscle nuclei; sensory pathways
5. CLINICAL FEATURES
5.1 Motor Features (Combined UMN + LMN)
- Weakness (progressive, often asymmetric initially)
- Muscle wasting / atrophy
- Fasciculations (spontaneous, visible especially in large proximal muscles)
- Hyporeflexia / areflexia (in PMA or late ALS)
- Cramps (often an early symptom)
- Flaccidity
- Hyperreflexia (paradoxically brisk reflexes in wasted limbs - a hallmark of ALS)
- Spasticity
- Babinski sign (extensor plantar response)
- Clonus
- Pseudobulbar affect (involuntary laughing/crying)
- Jaw jerk brisk (pseudobulbar palsy component)
5.2 Regional Onset Pattern
- Distal, asymmetric; typically one limb first
- Upper limb: thenar + intrinsic hand wasting, clumsy hand, dropping objects
- Lower limb: foot drop, stumbling; pyramidal pattern (hip flexion + ankle dorsiflexion most affected early)
- Muscle cramps often precede weakness
- Dysarthria: initially on fatigue; progresses to mixed spastic-flaccid dysarthria (tight, strained + nasal quality)
- Dysphagia: liquids before solids initially
- Sialorrhoea (drooling - from reduced swallowing frequency)
- Weak, wasted, fasciculating tongue
- Brisk jaw jerk; weak facial muscles
- Weight loss, aspiration pneumonia
- Diaphragm weakness: orthopnoea, paradoxical abdominal movement on inspiration
- Nocturnal hypoventilation: interrupted sleep, morning headaches, daytime somnolence, anorexia (CO₂ retention)
- Dyspnea on exertion; reduced FVC
- "Dropped head syndrome": neck extensor weakness - chin-on-chest posture (late)
5.3 Preserved Functions
- Extraocular movements (even in very advanced ALS - allows communication via eye tracking)
- Sphincter control / continence (Onuf's nucleus spared)
- Sensation is generally intact
- Proprioception preserved
5.4 Cognitive/Behavioral Features
- ~5% develop overt frontotemporal dementia (FTD) (ALS-FTD overlap)
- Up to 50% have subtle frontal lobe dysfunction without overt dementia
- C9ORF72 variant especially associated with cognitive/behavioral changes + family history of dementia
6. DIAGNOSIS
6.1 Awaji-Shima Criteria (Revised El Escorial Criteria)
- Evidence of LMN degeneration (clinical, electrophysiologic, or neuropathologic)
- Evidence of UMN degeneration (clinical examination)
- Progressive spread of symptoms/signs within or to other regions
- Absence of other disease processes explaining findings
| Level | Criteria |
|---|---|
| Definite ALS | UMN + LMN signs in bulbar region + ≥2 spinal regions, OR UMN + LMN in 3 spinal regions |
| Probable ALS | UMN + LMN signs in ≥2 regions, with UMN signs rostral to LMN signs |
| Possible ALS | UMN + LMN in 1 region only, OR UMN signs in ≥2 regions, OR LMN signs rostral to UMN signs |
6.2 Investigations
- EMG: Active denervation (fibrillations, positive sharp waves, fasciculation potentials) + chronic reinnervation (large-amplitude, long-duration, polyphasic MUAPs) in ≥2 regions not explained by single nerve/root lesion
- NCS: Normal or near-normal motor conduction velocities + amplitudes in early ALS; distinguishes from demyelinating neuropathies
- No conduction block (rules out multifocal motor neuropathy)
- MRI brain + spine: to exclude structural mimics (cervical myelopathy, brain tumor, syrinx); may show T2 hyperintensity along corticospinal tracts in ALS
- FBC, CRP, ESR, thyroid function, calcium, parathyroid hormone
- Serum protein electrophoresis (paraprotein neuropathy)
- CK (elevated in ALS + SMA from denervation)
- Anti-GM1 antibodies (multifocal motor neuropathy)
- Hexosaminidase A+B (GM2 gangliosidosis mimic)
- Genetic panel (SOD1, C9ORF72, FUS, TDP-43 in familial/atypical cases)
- Forced Vital Capacity (FVC): <50% predicted = indication for NIV
- Sniff Nasal Inspiratory Pressure (SNIP): sensitive for diaphragm weakness
- Peak Cough Flow (PCF): <270 L/min = risk of secretion retention
7. DIFFERENTIAL DIAGNOSIS
| MND Variant | Key Mimics | Distinguishing Features |
|---|---|---|
| PMA (LMN only) | Kennedy disease | AR gene testing; gynecomastia in Kennedy |
| PMA | Multifocal motor neuropathy (MMN) | Anti-GM1 antibodies; conduction block on NCS; responds to IVIG |
| PMA | Spinal muscular atrophy (SMA) | SMN gene deletion/mutation; childhood onset |
| ALS | Cervical myelopathy + radiculopathy | MRI spine; pure sensory signs; no fasciculations at multiple levels |
| ALS | Myasthenia gravis | Fatigability; no fasciculations; normal NCS/EMG; anti-AChR positive |
| PLS (UMN only) | Primary progressive MS | MRI lesions; oligoclonal bands in CSF |
| ALS | Thyrotoxicosis | TFTs; fasciculations + thyroid history |
| Bulbar ALS | Post-polio syndrome | History of polio; no UMN signs; stable/slowly progressive |
8. MANAGEMENT
8.1 Multidisciplinary Team (MDT)
- Neurologist (diagnosis, disease-modifying therapy)
- Physiotherapist (mobility, respiratory, exercise)
- Occupational therapist (ADL aids, environmental adaptation)
- Speech and language therapist (AAC, dysarthria, dysphagia)
- Dietitian (nutritional support, PEG timing)
- Respiratory physician (NIV, cough assist)
- Palliative care team (pain, end-of-life planning)
- Nurse specialist / case coordinator
- Social worker, psychologist
8.2 Disease-Modifying Pharmacotherapy
- Mechanism: sodium channel blocker; reduces excitotoxicity by inhibiting presynaptic glutamate release
- Benefit: prolongs survival by approximately 3 months (modest but the only proven survival benefit in most patients)
- Dose: 50 mg twice daily
- Side effects: nausea, fatigue, elevated liver enzymes (LFTs monitoring needed)
- Mechanism: free radical scavenger / antioxidant
- Approved in Japan (2015), USA (2017), certain other countries
- Benefit: slows functional decline in a subset of early ALS patients (ALSFRS-R)
- Given as IV infusion (original formulation) or oral suspension (newer)
- Specifically for SOD1-ALS
- Reduces SOD1 protein levels; lowers neurofilament biomarkers
- FDA-approved 2023 (accelerated approval); first genotype-specific ALS therapy
- Tyrosine kinase inhibitor; targets neuroinflammation (microglia/mast cells)
- Phase III trial data under regulatory review (as of 2024)
8.3 Symptomatic Management
| Symptom | Management |
|---|---|
| Spasticity | Baclofen (oral), tizanidine, dantrolene; physiotherapy; stretching |
| Cramps | Quinine sulfate (limited evidence); baclofen; magnesium |
| Fasciculations | Reassurance; mexiletine |
| Sialorrhoea | Anticholinergics (amitriptyline, hyoscine patch, glycopyrrolate); botulinum toxin to parotid glands; salivary gland radiotherapy |
| Thick secretions | Mucolytics (N-acetylcysteine, carbocisteine); nebulized saline; cough assist device |
| Pseudobulbar affect | Nuedexta (dextromethorphan + quinidine) - FDA approved; amitriptyline |
| Neuropathic pain | Gabapentin, pregabalin, amitriptyline |
| Anxiety/depression | SSRIs (citalopram, sertraline); counselling |
| Insomnia | Amitriptyline; melatonin; treat nocturnal hypoventilation |
8.4 Nutritional Management
- Malnutrition is an independent poor prognostic factor in ALS
- Dysphagia assessment: videofluoroscopy, fiberoptic endoscopic evaluation of swallowing (FEES)
- High-calorie diet; modified food/liquid textures per SLT
- Percutaneous endoscopic gastrostomy (PEG):
- Indicated when: weight loss >10% body weight, or FVC drops below 50% predicted (increased procedural risk at lower FVC)
- Improves nutrition, quality of life; survival benefit debated
8.5 Respiratory Management
- FVC every 3 months; SNIP, PCF
- Nocturnal oximetry if symptoms of nocturnal hypoventilation
- Indications: FVC <50% or rapidly falling; SNIP <40 cmH₂O; symptomatic nocturnal hypoventilation; orthopnoea
- Extends survival by average 7-12 months in non-bulbar ALS; improves quality of life and sleep
- Initiation at night first; titrate to daytime use as disease progresses
- Benefit reduced in severe bulbar ALS (unable to tolerate mask due to weak perioral muscles)
- Manual assisted cough: physiotherapist applies abdominal thrust during cough effort
- Mechanical insufflation-exsufflation (MI-E / CoughAssist): delivers positive pressure breath then rapid negative pressure - clears secretions effectively
- Target PCF >270 L/min with assistance
- Patient choice only (requires full counselling)
- Extends life indefinitely but with significant burden
- Requires around-the-clock carers; quality of life highly variable
8.6 Communication
- Augmentative and Alternative Communication (AAC):
- Voice amplifiers (early dysarthria)
- Voice banking: record speech for synthesis before it deteriorates
- Text-to-speech apps (e.g., Proloquo2Go, Grid)
- Eye-gaze technology (Tobii): allows communication via eye tracking when all limb function lost (critical in locked-in state)
8.7 Physiotherapy Management in MND
- Serial muscle strength testing (MMT, dynamometry)
- Respiratory function (FVC, PCF, SNIP)
- Gait and mobility assessment
- Berg Balance Scale, Timed Up and Go
- ALSFRS-R (ALS Functional Rating Scale-Revised): tracks function across domains
- Exercise should be moderate intensity - overwork weakness (eccentric damage to denervated muscle) must be avoided
- Resistance exercise: low resistance, high repetition; submaximal; focus on activities of daily living
- Fatigue management: energy conservation, prioritization of activities
- Aerobic exercise: evidence suggests moderate-intensity aerobic exercise (cycling, swimming) may slow decline and is safe
- Stretching and ROM exercises: daily passive/active stretching to prevent contractures
- Spasticity management: positioning, stretching, splinting, hydrotherapy; oral baclofen/tizanidine as adjunct
- Foot drop: AFO (ankle-foot orthosis) - improves safety and gait efficiency
- Cervical collar: for dropped head syndrome (soft collar first; rigid if severe)
- Falls prevention: home hazard assessment, walking aids (rollator frame with seat), wheelchair as needed
- Walking stick → crutch → rollator frame → manual wheelchair → powered wheelchair (when hand function lost)
- Hospital-type bed with pressure-relieving mattress; bed rail; ceiling hoist
- Stair lift / ramp for home access
- Bath/shower aids; commode
- Role: maintain airway clearance, support breathing efficiency, manage secretions
- Breathing exercises: diaphragmatic breathing, inspiratory muscle training (limited evidence; avoid fatigue)
- Glossopharyngeal breathing (GPB): augments ventilation when conventional breathing compromised
- Manual chest physiotherapy / percussion: loosens secretions
- Cough augmentation: manual assisted cough, CoughAssist device
- NIV setup and monitoring: physiotherapist often involved in mask fitting, acclimatization, monitoring
- Positioning: upright seating improves FVC; avoid supine in advanced disease
- Comfort positioning: pressure relief, limb elevation for oedema, pain relief positioning
- Passive movements to maintain comfort and prevent contractures
- Lymphoedema management for dependent limbs
- Breathlessness management: fan directed at face (stimulates trigeminal receptors, reduces dyspnoea sensation); pursed lip breathing
- Opioids (low-dose morphine) for refractory dyspnoea are appropriate and do not hasten death
9. PROGNOSIS
- Older age at onset
- Bulbar onset (shorter survival ~2 years vs. 3-4 years for limb onset)
- Rapid functional decline (slope of ALSFRS-R fall)
- Low FVC at diagnosis
- Low BMI / early weight loss
- C9ORF72 variant (more cognitive involvement)
- Shorter time from onset to diagnosis
- Young onset
- PLS variant (10+ years)
- Flail arm/leg variant (4-5 years)
- Limb onset
10. KEY OUTCOME MEASURES
| Scale | Use |
|---|---|
| ALSFRS-R (ALS Functional Rating Scale-Revised) | 12-item functional scale covering speech, swallowing, handwriting, dressing, turning in bed, walking, climbing stairs, dyspnoea, orthopnoea, respiratory insufficiency; 0-48; tracks decline |
| FVC (% predicted) | Respiratory function; primary survival predictor |
| SNIP (Sniff Nasal Inspiratory Pressure) | Diaphragm strength; <40 cmH₂O = poor prognosis |
| PCF (Peak Cough Flow) | Airway clearance; <270 L/min = risk |
| Norris Scale / Appel ALS Scale | Older functional tools |
| ALS Assessment Questionnaire (ALSAQ-40) | Quality of life |
11. SUMMARY TABLE: MND VARIANTS AT A GLANCE
| Variant | UMN Signs | LMN Signs | Region | Prognosis |
|---|---|---|---|---|
| Classic ALS | Yes | Yes | Spinal ± bulbar | Median 3 years |
| Bulbar-onset ALS | Yes (pseudobulbar) | Yes (flaccid bulbar) | Bulbar first | 2-3 years (worst) |
| PBP | Minimal | Yes | Bulbar only (initially) | Poor |
| PLS | Yes only | No | Spinal | Best (10+ years) |
| PMA | No | Yes only | Spinal | Intermediate |
| Flail arm | UMN later | Yes (arms) | Cervical | Better (>3 years) |
| Flail leg | UMN later | Yes (legs) | Lumbosacral | Better |
KEY REFERENCES
- Pathology, genetics, morphology: Robbins & Kumar Basic Pathology 10e; Goldman-Cecil Medicine 22e
- Clinical classification, subtypes, EMG criteria: Bradley and Daroff's Neurology in Clinical Practice
- Riluzole, edaravone, masitinib treatment: Adams and Victor's Principles of Neurology 12e; Goldman-Cecil Medicine 22e
- Physiotherapy guidelines: Hospice Foundation Ireland MND Physiotherapy Guidelines; NICE NG42
- 2024 EAN ALS Management Guideline: European Academy of Neurology, 2024
Make a presentation on physiotherapy progression through MND stages
mkdir -p /tmp/workspace/mnd-pptx && ls /tmp/workspace/mnd-pptx/
~/mnd-pptx/create_mnd_pptx.py
from pptx import Presentation
from pptx.util import Inches, Pt, Emu
from pptx.dml.color import RGBColor
from pptx.enum.text import PP_ALIGN, MSO_ANCHOR
from pptx.oxml.ns import qn
from lxml import etree
from io import BytesIO
# ── Colour palette ──────────────────────────────────────────────────────────
NAVY = RGBColor(0x0D, 0x2B, 0x55) # dark header bg
TEAL = RGBColor(0x00, 0x7A, 0x8A) # accent / stage bars
GREEN = RGBColor(0x2E, 0x86, 0x48) # Stage 1
AMBER = RGBColor(0xE8, 0x8C, 0x17) # Stage 2
ORANGE = RGBColor(0xD4, 0x4F, 0x1C) # Stage 3
PURPLE = RGBColor(0x6A, 0x35, 0x8A) # Stage 4 / palliative
WHITE = RGBColor(0xFF, 0xFF, 0xFF)
LIGHT_GREY = RGBColor(0xF2, 0xF4, 0xF7)
MID_GREY = RGBColor(0xCC, 0xD0, 0xD8)
DARK_GREY = RGBColor(0x3C, 0x3C, 0x3C)
STAGE_COLORS = [GREEN, AMBER, ORANGE, PURPLE]
prs = Presentation()
prs.slide_width = Inches(13.333)
prs.slide_height = Inches(7.5)
blank = prs.slide_layouts[6]
# ── Helpers ──────────────────────────────────────────────────────────────────
def add_rect(slide, x, y, w, h, fill_rgb, alpha_pct=None):
shape = slide.shapes.add_shape(1, Inches(x), Inches(y), Inches(w), Inches(h))
shape.line.fill.background()
shape.fill.solid()
shape.fill.fore_color.rgb = fill_rgb
return shape
def add_text(slide, text, x, y, w, h,
font_size=16, bold=False, color=DARK_GREY,
align=PP_ALIGN.LEFT, wrap=True, italic=False,
v_anchor=MSO_ANCHOR.TOP):
tb = slide.shapes.add_textbox(Inches(x), Inches(y), Inches(w), Inches(h))
tf = tb.text_frame
tf.word_wrap = wrap
tf.margin_left = Inches(0.05)
tf.margin_right = Inches(0.05)
tf.margin_top = Pt(2)
tf.margin_bottom = Pt(2)
tf.vertical_anchor = v_anchor
p = tf.paragraphs[0]
p.alignment = align
run = p.add_run()
run.text = text
run.font.size = Pt(font_size)
run.font.bold = bold
run.font.italic = italic
run.font.color.rgb = color
run.font.name = "Calibri"
return tb
def add_bullet_box(slide, items, x, y, w, h,
font_size=13, color=DARK_GREY, title=None,
title_color=NAVY, title_size=14, bg=None, pad=0.12):
if bg:
add_rect(slide, x, y, w, h, bg)
tb = slide.shapes.add_textbox(Inches(x + pad), Inches(y + pad),
Inches(w - 2*pad), Inches(h - 2*pad))
tf = tb.text_frame
tf.word_wrap = True
tf.margin_left = Inches(0.05)
tf.margin_right = Inches(0.05)
tf.margin_top = Pt(2)
tf.margin_bottom = Pt(2)
first = True
if title:
p = tf.paragraphs[0] if first else tf.add_paragraph()
first = False
run = p.add_run()
run.text = title
run.font.size = Pt(title_size)
run.font.bold = True
run.font.color.rgb = title_color
run.font.name = "Calibri"
for item in items:
p = tf.add_paragraph() if not first else tf.paragraphs[0]
first = False
p.space_before = Pt(2)
run = p.add_run()
run.text = f"• {item}"
run.font.size = Pt(font_size)
run.font.color.rgb = color
run.font.name = "Calibri"
def header_bar(slide, title, subtitle=None):
"""Dark navy top bar with title."""
add_rect(slide, 0, 0, 13.333, 1.1, NAVY)
add_text(slide, title,
0.3, 0.08, 12.5, 0.65,
font_size=28, bold=True, color=WHITE,
align=PP_ALIGN.LEFT, v_anchor=MSO_ANCHOR.MIDDLE)
if subtitle:
add_text(slide, subtitle,
0.3, 0.72, 12.5, 0.35,
font_size=14, bold=False, color=MID_GREY,
align=PP_ALIGN.LEFT)
# teal accent line below header
add_rect(slide, 0, 1.1, 13.333, 0.06, TEAL)
def stage_label(slide, label, x, y, w, h, color):
add_rect(slide, x, y, w, h, color)
add_text(slide, label, x, y, w, h,
font_size=12, bold=True, color=WHITE,
align=PP_ALIGN.CENTER, v_anchor=MSO_ANCHOR.MIDDLE)
# ═══════════════════════════════════════════════════════════════════════════
# SLIDE 1 – Title Slide
# ═══════════════════════════════════════════════════════════════════════════
slide = prs.slides.add_slide(blank)
# Full background gradient simulation with two rects
add_rect(slide, 0, 0, 13.333, 7.5, NAVY)
add_rect(slide, 0, 4.8, 13.333, 2.7, TEAL)
# Decorative accent
add_rect(slide, 0, 4.6, 13.333, 0.22, RGBColor(0xFF, 0xFF, 0xFF))
# Main title
add_text(slide,
"Physiotherapy Progression\nThrough MND Stages",
1.0, 1.0, 11.0, 3.0,
font_size=40, bold=True, color=WHITE,
align=PP_ALIGN.CENTER, v_anchor=MSO_ANCHOR.MIDDLE)
# Subtitle
add_text(slide,
"Motor Neuron Disease · Stage-by-Stage Rehabilitation Framework",
1.0, 3.8, 11.0, 0.6,
font_size=18, bold=False, color=MID_GREY,
align=PP_ALIGN.CENTER)
# Stage pills at bottom
stage_labels = ["Stage 1\nEarly", "Stage 2\nMiddle", "Stage 3\nLate", "Stage 4\nPalliative"]
for i, (lbl, col) in enumerate(zip(stage_labels, STAGE_COLORS)):
x = 1.0 + i * 2.9
add_rect(slide, x, 5.2, 2.5, 0.9, col)
add_text(slide, lbl, x, 5.2, 2.5, 0.9,
font_size=13, bold=True, color=WHITE,
align=PP_ALIGN.CENTER, v_anchor=MSO_ANCHOR.MIDDLE)
add_text(slide, "Based on NICE NG42 | Irish MND Guidelines | Goldman-Cecil Medicine",
0, 6.9, 13.333, 0.4,
font_size=10, color=RGBColor(0xCC, 0xDD, 0xFF),
align=PP_ALIGN.CENTER)
# ═══════════════════════════════════════════════════════════════════════════
# SLIDE 2 – MND Overview: What is MND?
# ═══════════════════════════════════════════════════════════════════════════
slide = prs.slides.add_slide(blank)
add_rect(slide, 0, 0, 13.333, 7.5, LIGHT_GREY)
header_bar(slide, "What is Motor Neuron Disease (MND)?",
"Understanding the disease before planning rehabilitation")
# Left column: key facts
add_bullet_box(slide,
["Progressive degeneration of UMN (motor cortex) & LMN (brainstem, spinal cord)",
"Incidence ~2/100,000 per year | Prevalence 5–8/100,000",
"Mean age of onset: 55–60 years | Male > Female",
"Median survival: 2–5 years (bulbar onset worst; PLS best)",
"Cause of death: respiratory failure in vast majority"],
x=0.3, y=1.3, w=6.5, h=3.5,
font_size=13, title="Key Facts", title_color=NAVY, bg=WHITE)
# Right column: types
add_bullet_box(slide,
["Classic ALS – mixed UMN + LMN (most common, 80%)",
"Progressive Bulbar Palsy (PBP) – bulbar onset, worst prognosis",
"Primary Lateral Sclerosis (PLS) – UMN only, best prognosis",
"Progressive Muscular Atrophy (PMA) – LMN only",
"Flail Arm / Flail Leg – segmental; longer survival"],
x=7.0, y=1.3, w=6.0, h=3.5,
font_size=13, title="Clinical Variants", title_color=TEAL, bg=WHITE)
# Bottom bar: PT role
add_rect(slide, 0.3, 5.1, 12.7, 2.0, NAVY)
add_text(slide,
"Role of Physiotherapy in MND",
0.5, 5.15, 12.3, 0.45,
font_size=14, bold=True, color=WHITE)
add_text(slide,
"Physiotherapy does NOT cure MND, but significantly improves quality of life, prolongs function, prevents "
"complications, and supports respiratory health across all stages. Management is multidisciplinary: "
"neurologist, PT, OT, SLT, dietitian, respiratory physician, palliative care.",
0.5, 5.6, 12.3, 1.4,
font_size=12, color=LIGHT_GREY, wrap=True)
# ═══════════════════════════════════════════════════════════════════════════
# SLIDE 3 – Disease Progression Timeline / Stages Overview
# ═══════════════════════════════════════════════════════════════════════════
slide = prs.slides.add_slide(blank)
add_rect(slide, 0, 0, 13.333, 7.5, LIGHT_GREY)
header_bar(slide, "MND Stages & Physiotherapy Framework",
"Staging guides goal-setting, exercise intensity, and equipment provision")
# Timeline arrow base
add_rect(slide, 0.3, 2.15, 12.4, 0.22, MID_GREY)
stage_data = [
("STAGE 1", "Early / Diagnosis", GREEN,
["Mild focal weakness", "Near-normal mobility", "Diagnosis shock"],
0.3),
("STAGE 2", "Moderate / Functional Loss", AMBER,
["Spreading weakness", "Mobility aids needed", "Fatigue prominent"],
3.55),
("STAGE 3", "Advanced / Dependence", ORANGE,
["Severe weakness", "Wheelchair use", "Respiratory compromise"],
6.8),
("STAGE 4", "End-Stage / Palliative", PURPLE,
["Minimal movement", "Ventilatory support", "Comfort focus"],
10.05),
]
for label, sub, color, features, x in stage_data:
w = 3.0
# Stage box
add_rect(slide, x, 1.3, w, 0.75, color)
add_text(slide, f"{label}\n{sub}", x, 1.3, w, 0.75,
font_size=11, bold=True, color=WHITE,
align=PP_ALIGN.CENTER, v_anchor=MSO_ANCHOR.MIDDLE)
# Arrow node
add_rect(slide, x + w/2 - 0.12, 2.02, 0.24, 0.38, color)
# Features below arrow
feat_text = "\n".join(f"› {f}" for f in features)
add_text(slide, feat_text, x, 2.5, w, 1.5,
font_size=11, color=DARK_GREY, wrap=True)
# ALSFRS-R scale indicator
add_rect(slide, 0.3, 4.15, 12.4, 0.06, MID_GREY)
add_text(slide, "ALSFRS-R Scale (48 → 0)", 0.3, 4.25, 3.0, 0.35,
font_size=11, bold=True, color=DARK_GREY)
vals = ["~40–48", "~25–39", "~10–24", "~0–9"]
for i, (val, x) in enumerate(zip(vals, [0.3, 3.55, 6.8, 10.05])):
add_rect(slide, x, 4.25, 3.0, 0.35, STAGE_COLORS[i])
add_text(slide, val, x, 4.25, 3.0, 0.35,
font_size=12, bold=True, color=WHITE,
align=PP_ALIGN.CENTER, v_anchor=MSO_ANCHOR.MIDDLE)
# Bottom: general PT principle
add_rect(slide, 0.3, 4.8, 12.7, 2.4, WHITE)
add_text(slide,
"Core PT Principle: Never Cause Overwork Weakness",
0.5, 4.88, 12.3, 0.45,
font_size=14, bold=True, color=TEAL)
add_text(slide,
"Denervated muscles are vulnerable to eccentric damage. Exercise must be SUBMAXIMAL. "
"As the disease progresses, shift emphasis: early (strengthen & mobilise) → middle (maintain & compensate) "
"→ late (prevent complications & assist) → palliative (comfort & dignity).",
0.5, 5.32, 12.3, 1.8,
font_size=12, color=DARK_GREY, wrap=True)
# ═══════════════════════════════════════════════════════════════════════════
# SLIDE 4 – Stage 1: Early MND
# ═══════════════════════════════════════════════════════════════════════════
slide = prs.slides.add_slide(blank)
add_rect(slide, 0, 0, 13.333, 7.5, LIGHT_GREY)
# Coloured top bar with stage label
add_rect(slide, 0, 0, 13.333, 1.25, GREEN)
add_rect(slide, 0, 1.25, 13.333, 0.06, TEAL)
add_text(slide, "STAGE 1 · Early MND", 0.3, 0.05, 9.0, 0.7,
font_size=28, bold=True, color=WHITE, v_anchor=MSO_ANCHOR.MIDDLE)
add_text(slide, "ALSFRS-R ~40–48 | Mild focal weakness | Near-normal independence",
0.3, 0.75, 11.0, 0.45, font_size=13, color=RGBColor(0xCC, 0xFF, 0xCC))
col_w = 4.0
col_y = 1.45
col_h = 4.7
gaps = [0.25, 4.45, 8.65]
add_bullet_box(slide,
["Asymmetric distal weakness (hand or foot)",
"Fatigue with prolonged activity",
"Near-normal gait; minor foot drop",
"Fasciculations / cramps",
"Mild dysarthria (bulbar onset)",
"Anxiety, adjustment to diagnosis"],
x=gaps[0], y=col_y, w=col_w, h=col_h,
font_size=12, title="Clinical Picture", title_color=GREEN, bg=WHITE)
add_bullet_box(slide,
["Submaximal resistance training (2–3×/week)",
"Aerobic exercise: cycling / swimming at 60–70% HRmax",
"Stretching: daily full ROM, Achilles + hip flexors",
"Gait analysis: AFO for foot drop if needed",
"Postural correction and ergonomic advice",
"Energy conservation strategies",
"Balance training: single-leg stance, foam pad"],
x=gaps[1], y=col_y, w=col_w, h=col_h,
font_size=12, title="Physiotherapy Goals & Interventions", title_color=GREEN, bg=WHITE)
add_bullet_box(slide,
["Baseline FVC, SNIP, PCF",
"Incentive spirometry",
"Diaphragmatic breathing technique",
"Educate on early NIV signs to watch",
"Walking stick (if unstable)",
"Wrist / ankle splints as needed",
"Home exercise programme (HEP)",
"Psychological support + peer referral"],
x=gaps[2], y=col_y, w=col_w, h=col_h,
font_size=12, title="Respiratory, Equipment & Education", title_color=TEAL, bg=WHITE)
# Bottom banner
add_rect(slide, 0.25, 6.3, 12.8, 0.9, GREEN)
add_text(slide,
"Goals: Maximise strength & endurance | Prevent deconditioning | Educate patient & family | Baseline documentation",
0.35, 6.3, 12.6, 0.9,
font_size=12, bold=True, color=WHITE,
align=PP_ALIGN.CENTER, v_anchor=MSO_ANCHOR.MIDDLE)
# ═══════════════════════════════════════════════════════════════════════════
# SLIDE 5 – Stage 2: Middle MND
# ═══════════════════════════════════════════════════════════════════════════
slide = prs.slides.add_slide(blank)
add_rect(slide, 0, 0, 13.333, 7.5, LIGHT_GREY)
add_rect(slide, 0, 0, 13.333, 1.25, AMBER)
add_rect(slide, 0, 1.25, 13.333, 0.06, TEAL)
add_text(slide, "STAGE 2 · Middle / Moderate MND", 0.3, 0.05, 9.0, 0.7,
font_size=28, bold=True, color=WHITE, v_anchor=MSO_ANCHOR.MIDDLE)
add_text(slide, "ALSFRS-R ~25–39 | Spreading weakness | Mobility aids required",
0.3, 0.75, 11.0, 0.45, font_size=13, color=WHITE)
col_w = 4.0
col_y = 1.45
col_h = 4.7
add_bullet_box(slide,
["Bilateral limb involvement",
"Fatigue limits ADLs significantly",
"Rollator / walking frame required",
"Dysphagia / dysarthria progressing",
"Dropped head in some patients",
"Nocturnal hypoventilation beginning",
"Depression / grief common"],
x=gaps[0], y=col_y, w=col_w, h=col_h,
font_size=12, title="Clinical Picture", title_color=AMBER, bg=WHITE)
add_bullet_box(slide,
["Maintain ROM: daily passive + active-assisted stretching",
"Reduce resistance training intensity; prioritise function",
"Aquatic therapy: buoyancy-assisted strengthening",
"Spasticity management: stretching, positioning, splinting",
"Falls prevention: home hazard assessment",
"Cervical collar for dropped head syndrome",
"Wheelchair assessment (manual → consider powered)",
"Adaptive ADL training with OT"],
x=gaps[1], y=col_y, w=col_w, h=col_h,
font_size=12, title="Physiotherapy Interventions", title_color=AMBER, bg=WHITE)
add_bullet_box(slide,
["Serial FVC every 3 months (SNIP, PCF)",
"Nocturnal oximetry if symptomatic",
"Initiate BiPAP/NIV when FVC <50%",
"Manual cough assist technique",
"Rollator → walking frame → wheelchair",
"Hospital bed + pressure-relief mattress",
"Ceiling hoist / transfer belt",
"PEG discussion if dysphagia + weight loss"],
x=gaps[2], y=col_y, w=col_w, h=col_h,
font_size=12, title="Respiratory, Equipment & Education", title_color=TEAL, bg=WHITE)
add_rect(slide, 0.25, 6.3, 12.8, 0.9, AMBER)
add_text(slide,
"Goals: Maintain independence as long as possible | Prevent contractures & falls | Initiate respiratory support | Timely equipment",
0.35, 6.3, 12.6, 0.9,
font_size=12, bold=True, color=WHITE,
align=PP_ALIGN.CENTER, v_anchor=MSO_ANCHOR.MIDDLE)
# ═══════════════════════════════════════════════════════════════════════════
# SLIDE 6 – Stage 3: Late / Advanced MND
# ═══════════════════════════════════════════════════════════════════════════
slide = prs.slides.add_slide(blank)
add_rect(slide, 0, 0, 13.333, 7.5, LIGHT_GREY)
add_rect(slide, 0, 0, 13.333, 1.25, ORANGE)
add_rect(slide, 0, 1.25, 13.333, 0.06, TEAL)
add_text(slide, "STAGE 3 · Advanced / Late MND", 0.3, 0.05, 9.0, 0.7,
font_size=28, bold=True, color=WHITE, v_anchor=MSO_ANCHOR.MIDDLE)
add_text(slide, "ALSFRS-R ~10–24 | Severe weakness | Full wheelchair dependence",
0.3, 0.75, 11.0, 0.45, font_size=13, color=WHITE)
col_w = 4.0
col_y = 1.45
col_h = 4.7
add_bullet_box(slide,
["Minimal or no voluntary limb movement",
"Wheelchair bound; needs hoisting",
"Severe dysarthria → AAC devices",
"Aspiration risk + weight loss",
"Significant respiratory compromise",
"Orthostatic hypotension risk",
"Skin integrity / pressure ulcer risk"],
x=gaps[0], y=col_y, w=col_w, h=col_h,
font_size=12, title="Clinical Picture", title_color=ORANGE, bg=WHITE)
add_bullet_box(slide,
["Passive ROM to ALL limbs: prevent pain + contracture",
"Positioning: anti-contracture splints; seating assessment",
"Pressure relief: 2-hourly turns if in bed",
"Oedema management: elevation + compression",
"Trunk support in wheelchair (customised seating)",
"Transfer training for carers (safe handling)",
"Minimal active exercise as tolerated",
"Hydrotherapy only if safe (aspiration risk)"],
x=gaps[1], y=col_y, w=col_w, h=col_h,
font_size=12, title="Physiotherapy Interventions", title_color=ORANGE, bg=WHITE)
add_bullet_box(slide,
["NIV: titrate to 24hr use as tolerated",
"Mechanical insufflation-exsufflation (CoughAssist)",
"Manual chest physiotherapy + suctioning",
"Discuss tracheostomy (patient decision)",
"Power wheelchair with head/eye control",
"Electric profiling bed; ceiling hoist",
"Specialised pressure-relieving cushion",
"Begin advance care planning discussions"],
x=gaps[2], y=col_y, w=col_w, h=col_h,
font_size=12, title="Respiratory, Equipment & Education", title_color=TEAL, bg=WHITE)
add_rect(slide, 0.25, 6.3, 12.8, 0.9, ORANGE)
add_text(slide,
"Goals: Prevent pressure ulcers & contractures | Airway clearance | Carer training | Advance care planning",
0.35, 6.3, 12.6, 0.9,
font_size=12, bold=True, color=WHITE,
align=PP_ALIGN.CENTER, v_anchor=MSO_ANCHOR.MIDDLE)
# ═══════════════════════════════════════════════════════════════════════════
# SLIDE 7 – Stage 4: Palliative / End-Stage MND
# ═══════════════════════════════════════════════════════════════════════════
slide = prs.slides.add_slide(blank)
add_rect(slide, 0, 0, 13.333, 7.5, LIGHT_GREY)
add_rect(slide, 0, 0, 13.333, 1.25, PURPLE)
add_rect(slide, 0, 1.25, 13.333, 0.06, TEAL)
add_text(slide, "STAGE 4 · Palliative / End-Stage MND", 0.3, 0.05, 9.0, 0.7,
font_size=28, bold=True, color=WHITE, v_anchor=MSO_ANCHOR.MIDDLE)
add_text(slide, "ALSFRS-R ~0–9 | Ventilator dependent | Comfort and dignity",
0.3, 0.75, 11.0, 0.45, font_size=13, color=RGBColor(0xCC, 0xCC, 0xFF))
col_w = 4.0
col_y = 1.45
col_h = 4.7
add_bullet_box(slide,
["Locked-in or near-locked-in state",
"Completely ventilator dependent",
"Eye movements ± preserved",
"Communication via eye tracking only",
"Severe pain, dyspnoea, anxiety",
"End-of-life decisions imminent"],
x=gaps[0], y=col_y, w=col_w, h=col_h,
font_size=12, title="Clinical Picture", title_color=PURPLE, bg=WHITE)
add_bullet_box(slide,
["Gentle passive movements for comfort",
"Positioning: pain-free postures; pressure relief",
"Lymphoedema management (elevation, gentle massage)",
"Breathlessness: fan to face (trigeminal stimulation)",
"Pursed-lip breathing / pacing as able",
"Family / carer education: positioning, turns",
"Coordinate with palliative team for pain control",
"Psychological & spiritual support"],
x=gaps[1], y=col_y, w=col_w, h=col_h,
font_size=12, title="Physiotherapy Interventions", title_color=PURPLE, bg=WHITE)
add_bullet_box(slide,
["Opioids for refractory dyspnoea (do NOT hasten death)",
"Suctioning for secretion management",
"Withdrawal of ventilation: patient-led decision",
"Symptom comfort: benzodiazepines for anxiety",
"Eye-gaze device for communication",
"Community / hospice co-ordination",
"Bereavement support for family",
"Physiotherapy role = comfort + dignity"],
x=gaps[2], y=col_y, w=col_w, h=col_h,
font_size=12, title="Respiratory, Symptom & Psychosocial", title_color=TEAL, bg=WHITE)
add_rect(slide, 0.25, 6.3, 12.8, 0.9, PURPLE)
add_text(slide,
"Goals: Dignity & comfort | Symptom management | Family support | Peaceful end-of-life care",
0.35, 6.3, 12.6, 0.9,
font_size=12, bold=True, color=WHITE,
align=PP_ALIGN.CENTER, v_anchor=MSO_ANCHOR.MIDDLE)
# ═══════════════════════════════════════════════════════════════════════════
# SLIDE 8 – Respiratory Physiotherapy Across All Stages
# ═══════════════════════════════════════════════════════════════════════════
slide = prs.slides.add_slide(blank)
add_rect(slide, 0, 0, 13.333, 7.5, LIGHT_GREY)
header_bar(slide, "Respiratory Physiotherapy Across MND Stages",
"Respiratory failure is the most common cause of death — early monitoring is life-saving")
# Four stage columns
resp_data = [
("Stage 1", GREEN,
["Baseline FVC, SNIP, PCF",
"Teach diaphragmatic breathing",
"Incentive spirometry",
"Educate on warning signs",
"Glossopharyngeal breathing intro"]),
("Stage 2", AMBER,
["Serial FVC every 3 months",
"Nocturnal oximetry if needed",
"Initiate BiPAP / NIV at FVC <50%",
"Manual assisted cough",
"Mucolytics / nebulised saline"]),
("Stage 3", ORANGE,
["NIV up to 24hr / day",
"CoughAssist (MI-E) device",
"Chest physiotherapy + suctioning",
"Tracheostomy decision making",
"ICU liaison if acute deterioration"]),
("Stage 4", PURPLE,
["Comfort ventilation only",
"Opioids for dyspnoea",
"Suctioning as needed",
"Fan therapy for air hunger",
"Ventilator withdrawal (patient choice)"]),
]
for i, (stg, col, items) in enumerate(resp_data):
x = 0.3 + i * 3.25
add_rect(slide, x, 1.28, 3.0, 0.5, col)
add_text(slide, stg, x, 1.28, 3.0, 0.5,
font_size=14, bold=True, color=WHITE,
align=PP_ALIGN.CENTER, v_anchor=MSO_ANCHOR.MIDDLE)
add_bullet_box(slide, items,
x=x, y=1.82, w=3.0, h=4.2,
font_size=12, bg=WHITE)
# Key thresholds box
add_rect(slide, 0.3, 6.15, 12.7, 1.05, NAVY)
thresholds = ("Key Thresholds: FVC <50% → initiate NIV | "
"SNIP <40 cmH₂O → NIV urgently | "
"PCF <270 L/min → cough assist | "
"FVC <20 mL/kg → ICU/intubation (GBS-style if acute)")
add_text(slide, thresholds, 0.5, 6.18, 12.3, 1.0,
font_size=11, bold=False, color=WHITE, wrap=True)
# ═══════════════════════════════════════════════════════════════════════════
# SLIDE 9 – Exercise Prescription Across Stages
# ═══════════════════════════════════════════════════════════════════════════
slide = prs.slides.add_slide(blank)
add_rect(slide, 0, 0, 13.333, 7.5, LIGHT_GREY)
header_bar(slide, "Exercise Prescription Across MND Stages",
"Submaximal loading — avoid overwork weakness at all stages")
# Table header
headers = ["Parameter", "Stage 1 (Early)", "Stage 2 (Middle)", "Stage 3 (Late)", "Stage 4 (Palliative)"]
col_colors = [NAVY, GREEN, AMBER, ORANGE, PURPLE]
col_x = [0.25, 2.65, 5.05, 7.45, 9.85]
col_w_vals = [2.3, 2.3, 2.3, 2.3, 3.2]
row_h = 0.62
for i, (hdr, col, x, w) in enumerate(zip(headers, col_colors, col_x, col_w_vals)):
add_rect(slide, x, 1.28, w, 0.5, col)
add_text(slide, hdr, x, 1.28, w, 0.5,
font_size=11, bold=True, color=WHITE,
align=PP_ALIGN.CENTER, v_anchor=MSO_ANCHOR.MIDDLE)
rows = [
("Resistance\nTraining",
"Low-mod resistance\n2–3×/week, 3×10 reps\nSubmax intensity",
"Light resistance only\nFocus on function\nAvoid fatigue",
"Passive/active-assisted\nGravity-eliminated\nAs tolerated",
"None / gentle\npassive movements"),
("Aerobic\nExercise",
"Cycling / swimming\n60–70% HRmax\n20–30 min, 3×/week",
"Aquatic therapy\nStationary cycling\nReduce duration",
"Supported seated\nexercise only\nShort sessions",
"Not applicable"),
("Stretching\n& ROM",
"Active: full ROM daily\nAchilles / hip flexors\nPosture correction",
"Active-assisted\n+ passive stretching\nAnti-spasticity",
"Passive ROM all limbs\nSplinting at night\nTurning schedule",
"Gentle passive\nmovements for\ncomfort only"),
("Balance\n& Gait",
"Single-leg stance\nFoam pad training\nAFO if foot drop",
"Walking frame\nFalls prevention\nGait re-education",
"Wheelchair mobility\nTransfer training\nCarer training",
"Positioning\nin bed / chair\nonly"),
("Key\nPrinciple",
"Strengthen &\nenergise",
"Maintain &\ncompensate",
"Prevent\ncomplications",
"Comfort\n& dignity"),
]
row_bgs = [WHITE, LIGHT_GREY, WHITE, LIGHT_GREY, MID_GREY]
for r_idx, (row, bg) in enumerate(zip(rows, row_bgs)):
y = 1.82 + r_idx * row_h
for c_idx, (cell, x, w) in enumerate(zip(row, col_x, col_w_vals)):
add_rect(slide, x, y, w, row_h, bg)
txt_color = DARK_GREY if c_idx == 0 else DARK_GREY
if c_idx == 0:
txt_color = NAVY
add_text(slide, cell, x + 0.05, y + 0.04, w - 0.1, row_h - 0.08,
font_size=9.5, color=txt_color,
bold=(c_idx == 0), wrap=True,
v_anchor=MSO_ANCHOR.TOP)
add_rect(slide, 0.25, 6.98, 12.8, 0.32, TEAL)
add_text(slide,
"⚠ OVERWORK WEAKNESS WARNING: Never exercise to exhaustion. If fatigue persists >30 min post-exercise, reduce intensity immediately.",
0.4, 6.98, 12.5, 0.32,
font_size=10, bold=True, color=WHITE, v_anchor=MSO_ANCHOR.MIDDLE)
# ═══════════════════════════════════════════════════════════════════════════
# SLIDE 10 – Equipment Progression Timeline
# ═══════════════════════════════════════════════════════════════════════════
slide = prs.slides.add_slide(blank)
add_rect(slide, 0, 0, 13.333, 7.5, LIGHT_GREY)
header_bar(slide, "Equipment & Assistive Device Progression",
"Timely provision prevents falls, maintains independence, and reduces carer burden")
categories = [
("Mobility", ["Walking stick", "Crutch / Nordic poles", "Rollator frame", "Manual wheelchair", "Power wheelchair", "Eye-gaze chair control"]),
("Seating\n& Bed", ["Ergonomic chair", "Riser-recliner chair", "Customised wheelchair seating", "Hospital bed + rails", "Profiling bed", "Pressure-relief mattress"]),
("Respiratory", ["Incentive spirometer", "NIV/BiPAP mask + machine", "CoughAssist (MI-E)", "Suction machine", "Tracheostomy (if chosen)", "Ventilator"]),
("Transfers\n& Hoisting", ["Grab rails + bath aids", "Transfer belt", "Rotunda turn table", "Mobile hoist", "Ceiling track hoist", "Full-body sling"]),
("Communication", ["Voice amplifier", "Voice banking app", "Speech-to-text app", "AAC tablet device", "Eye-gaze device", "Brain-computer interface"]),
]
cat_x = [0.25, 2.9, 5.55, 8.2, 10.85]
cat_w = 2.4
stage_bands = [(GREEN, "S1"), (AMBER, "S1–2"), (AMBER, "S2"), (ORANGE, "S2–3"), (ORANGE, "S3"), (PURPLE, "S3–4")]
for cat_idx, ((cat_name, items), x) in enumerate(zip(categories, cat_x)):
# Header
add_rect(slide, x, 1.28, cat_w, 0.48, NAVY)
add_text(slide, cat_name, x, 1.28, cat_w, 0.48,
font_size=12, bold=True, color=WHITE,
align=PP_ALIGN.CENTER, v_anchor=MSO_ANCHOR.MIDDLE)
# Items
for item_idx, (item, (col, stg)) in enumerate(zip(items, stage_bands)):
iy = 1.82 + item_idx * 0.87
add_rect(slide, x, iy, cat_w, 0.82, WHITE)
add_rect(slide, x, iy, 0.35, 0.82, col)
add_text(slide, stg, x, iy, 0.35, 0.82,
font_size=8, bold=True, color=WHITE,
align=PP_ALIGN.CENTER, v_anchor=MSO_ANCHOR.MIDDLE)
add_text(slide, item, x + 0.38, iy + 0.05, cat_w - 0.42, 0.72,
font_size=10.5, color=DARK_GREY, wrap=True,
v_anchor=MSO_ANCHOR.MIDDLE)
# Legend
lx = 0.25
for col, stg, label in [(GREEN, "S1", "Stage 1"), (AMBER, "S2", "Stage 2"),
(ORANGE, "S3", "Stage 3"), (PURPLE, "S4", "Stage 4")]:
add_rect(slide, lx, 7.18, 0.35, 0.22, col)
add_text(slide, f"{stg} = {label}", lx + 0.38, 7.18, 1.8, 0.22,
font_size=10, color=DARK_GREY)
lx += 2.3
# ═══════════════════════════════════════════════════════════════════════════
# SLIDE 11 – Outcome Measures & Monitoring
# ═══════════════════════════════════════════════════════════════════════════
slide = prs.slides.add_slide(blank)
add_rect(slide, 0, 0, 13.333, 7.5, LIGHT_GREY)
header_bar(slide, "Outcome Measures & Monitoring in MND",
"Serial measurement guides treatment decisions and triggers timely interventions")
om_left = [
("ALSFRS-R\n(ALS Functional Rating Scale-Revised)",
"48-item scale covering speech, swallowing, handwriting, dressing, turning in bed, walking, stairs, dyspnoea, orthopnoea, respiratory sufficiency. Score 0–48. Track rate of decline (≥1 pt/month = faster progression)."),
("FVC – Forced Vital Capacity",
"Primary respiratory predictor. Serial 3-monthly. FVC <50% → initiate NIV. FVC <30% → urgent NIV. Major independent predictor of survival."),
("SNIP – Sniff Nasal Inspiratory Pressure",
"More sensitive for early diaphragm weakness than FVC. SNIP <40 cmH₂O = poor prognosis; initiate NIV if symptomatic."),
("PCF – Peak Cough Flow",
"Measures cough effectiveness. <270 L/min = risk of secretion retention; <160 L/min = critical, CoughAssist essential."),
]
om_right = [
("Berg Balance Scale (BBS)",
"14-item balance assessment (0–56). Track fall risk in Stage 1–2 MND. Score <45 = high fall risk."),
("Timed Up and Go (TUG)",
"Functional mobility marker. Increasing time indicates mobility decline. Trigger for walking aid upgrade."),
("Grip / Pinch Dynamometry",
"Handheld dynamometry: track hand strength serially. Key for planning assistive devices."),
("ALSAQ-40 / ALS Assessment Questionnaire",
"Quality-of-life tool specific to ALS: 40 items across mobility, ADL, eating, communication, and emotional wellbeing."),
]
for i, (title, desc) in enumerate(om_left):
y = 1.35 + i * 1.45
add_rect(slide, 0.25, y, 6.1, 1.35, WHITE)
add_rect(slide, 0.25, y, 0.22, 1.35, TEAL)
add_text(slide, title, 0.55, y + 0.05, 5.6, 0.48,
font_size=11, bold=True, color=NAVY, wrap=True)
add_text(slide, desc, 0.55, y + 0.5, 5.6, 0.82,
font_size=10, color=DARK_GREY, wrap=True)
for i, (title, desc) in enumerate(om_right):
y = 1.35 + i * 1.45
add_rect(slide, 6.7, y, 6.4, 1.35, WHITE)
add_rect(slide, 6.7, y, 0.22, 1.35, TEAL)
add_text(slide, title, 7.0, y + 0.05, 5.9, 0.48,
font_size=11, bold=True, color=NAVY, wrap=True)
add_text(slide, desc, 7.0, y + 0.5, 5.9, 0.82,
font_size=10, color=DARK_GREY, wrap=True)
add_rect(slide, 0.25, 7.1, 12.8, 0.28, NAVY)
add_text(slide,
"Monitor at every visit: weight, pain score (NRS), fatigue, sleep quality, mood. Trigger MDT meeting if ALSFRS-R drops >2 points/month.",
0.4, 7.1, 12.5, 0.28,
font_size=10, color=WHITE, v_anchor=MSO_ANCHOR.MIDDLE)
# ═══════════════════════════════════════════════════════════════════════════
# SLIDE 12 – Summary & Key Principles
# ═══════════════════════════════════════════════════════════════════════════
slide = prs.slides.add_slide(blank)
add_rect(slide, 0, 0, 13.333, 7.5, NAVY)
add_rect(slide, 0, 0, 13.333, 1.3, TEAL)
add_text(slide, "Summary: Physiotherapy in MND", 0.4, 0.1, 12.5, 0.95,
font_size=30, bold=True, color=WHITE,
align=PP_ALIGN.CENTER, v_anchor=MSO_ANCHOR.MIDDLE)
add_text(slide, "A stage-guided, patient-centred, multidisciplinary approach",
0.4, 1.0, 12.5, 0.35,
font_size=14, color=WHITE, align=PP_ALIGN.CENTER)
principles = [
("Do No Harm", GREEN, "Never exercise to exhaustion. Submaximal is the rule throughout MND."),
("Adapt Early", AMBER, "Provide equipment proactively, before falls and crises occur."),
("Breathe First", ORANGE, "Respiratory monitoring and NIV initiation are the highest priority as disease progresses."),
("Family-Centred", PURPLE, "Train carers at every stage. Their confidence improves patient safety at home."),
("Dignity in Palliation",TEAL, "In Stage 4, physiotherapy is not about recovery — it is about comfort, dignity, and peaceful end-of-life."),
("MDT Always", RGBColor(0x4A, 0x90, 0xD9), "No physiotherapist works alone. Coordinate with SLT, OT, dietitian, palliative team at every stage."),
]
for i, (title, col, desc) in enumerate(principles):
row = i // 3
col_pos = i % 3
x = 0.3 + col_pos * 4.35
y = 1.55 + row * 2.5
add_rect(slide, x, y, 4.0, 2.2, RGBColor(0x1A, 0x3A, 0x6A))
add_rect(slide, x, y, 4.0, 0.38, col)
add_text(slide, title, x + 0.1, y, 3.8, 0.38,
font_size=13, bold=True, color=WHITE, v_anchor=MSO_ANCHOR.MIDDLE)
add_text(slide, desc, x + 0.1, y + 0.42, 3.8, 1.7,
font_size=11, color=RGBColor(0xCC, 0xDD, 0xFF), wrap=True)
add_text(slide,
"References: Goldman-Cecil Medicine 22e · Bradley & Daroff's Neurology · Adams & Victor's Neurology 12e · NICE NG42 · Hospice Foundation Ireland MND Guidelines",
0.3, 7.18, 12.7, 0.28,
font_size=8.5, color=MID_GREY, align=PP_ALIGN.CENTER)
# ─── Save ───────────────────────────────────────────────────────────────────
out_path = "/tmp/workspace/mnd-pptx/Physiotherapy_Progression_MND_Stages.pptx"
buf = BytesIO()
prs.save(buf)
with open(out_path, "wb") as f:
f.write(buf.getvalue())
print(f"Saved: {out_path}")
import os
print(f"Size: {os.path.getsize(out_path):,} bytes")
print(f"Slides: {len(prs.slides)}")
cd /tmp/workspace/mnd-pptx && python create_mnd_pptx.py
Physiotherapy Progression MND Stages
Presentation · PPTX
| # | Slide | Highlights |
|---|---|---|
| 1 | Title Slide | Stage colour pills (green/amber/orange/purple), references |
| 2 | What is MND? | Key facts, clinical variants, PT role overview |
| 3 | Stages Framework | ALSFRS-R ranges, timeline arrow, core PT principle (no overwork) |
| 4 | Stage 1 - Early | Clinical picture, exercise, respiratory + equipment (green theme) |
| 5 | Stage 2 - Middle | Spreading weakness, aquatic therapy, BiPAP initiation (amber theme) |
| 6 | Stage 3 - Advanced | Passive care, CoughAssist, carer training (orange theme) |
| 7 | Stage 4 - Palliative | Comfort, fan therapy, opioids, advance care planning (purple theme) |
| 8 | Respiratory PT | 4-column stage-by-stage respiratory management + key thresholds |
| 9 | Exercise Prescription Table | Resistance, aerobic, stretching, balance across all 4 stages |
| 10 | Equipment Timeline | Mobility, seating, respiratory, hoisting, communication devices by stage |
| 11 | Outcome Measures | ALSFRS-R, FVC, SNIP, PCF, Berg Balance, TUG, dynamometry, ALSAQ-40 |
| 12 | Summary | 6 key principles (Do No Harm, Adapt Early, Breathe First, etc.) |