Give me notes on pharmacology
Asking for Preferences
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
I have enough rich content from Lippincott's to now write comprehensive nursing pharmacology notes. Let me compile them:
Pharmacology Notes - Nursing/Allied Health
Source: Lippincott Illustrated Reviews: Pharmacology
SECTION 1: PHARMACOKINETICS (What the Body Does to the Drug)
The four core processes are ADME: Absorption, Distribution, Metabolism, Elimination.
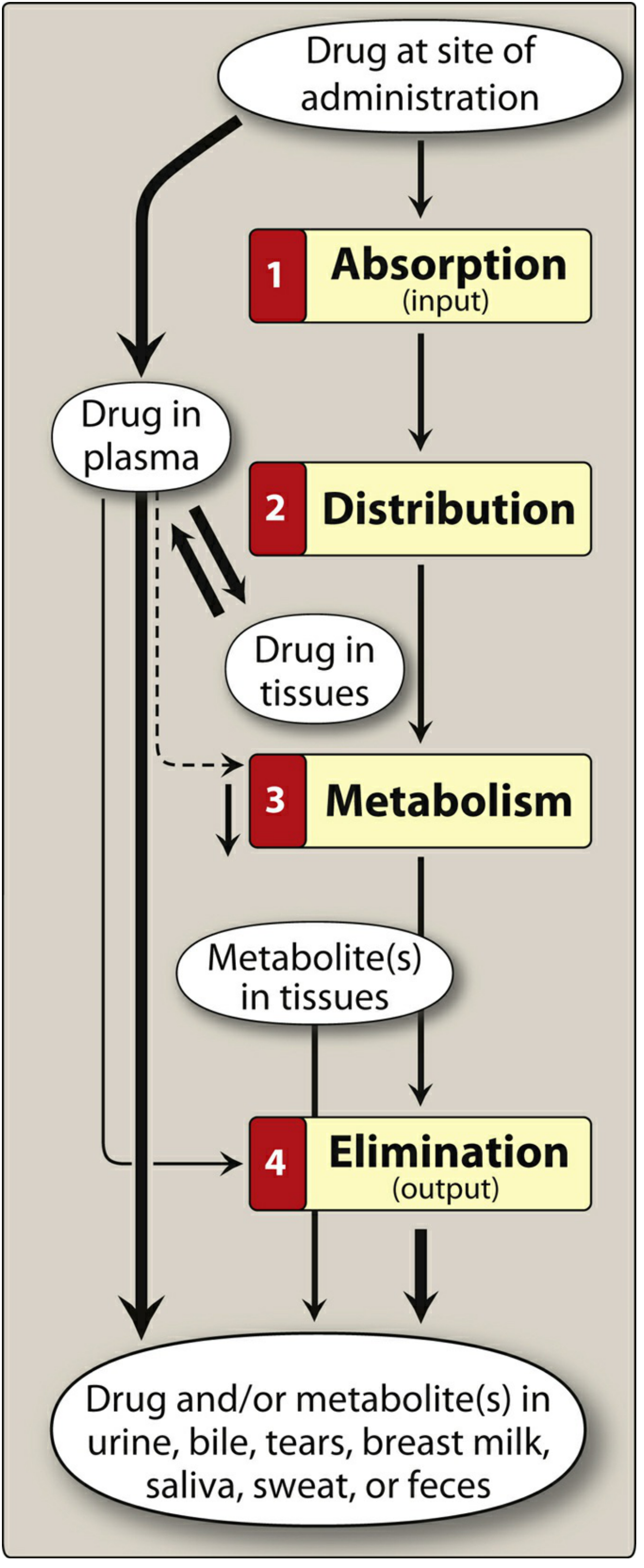
1. Absorption
How drug enters the bloodstream from the site of administration.
| Route | Key Points | Examples |
|---|---|---|
| Oral (PO) | Most common, convenient, economical. Low gastric pH inactivates some drugs. Subject to first-pass metabolism. | Acetaminophen, amoxicillin |
| Sublingual / Buccal | Placed under tongue or between cheek/gum. Bypasses first-pass metabolism. Rapid effect. | Nitroglycerin, buprenorphine |
| Intravenous (IV) | 100% bioavailability. Immediate effect. No absorption needed. Ideal for emergencies. Risk: infection, phlebitis. | Morphine IV, vancomycin |
| Intramuscular (IM) | Good for oily or poorly soluble drugs. Moderate absorption speed. | Vaccines, haloperidol decanoate |
| Subcutaneous (SC) | Slower, sustained absorption. Limited to small volumes. | Insulin, heparin |
| Transdermal | Systemic effect via skin patch. Rate depends on skin lipid solubility. | Nicotine patch, fentanyl patch |
| Inhalation | Delivers drug directly to lungs, minimizes systemic side effects. | Albuterol, fluticasone |
| Rectal | Useful when patient is vomiting or unconscious. Absorption erratic. | Diazepam rectal, promethazine suppository |
Enteric-coated preparations - protect acid-labile drugs or reduce gastric irritation (e.g., omeprazole, aspirin EC).
Extended-release (ER/XR/SR/CR) - slower absorption, less frequent dosing, better compliance, fewer peaks/troughs. Useful for drugs with short half-lives (e.g., morphine ER dosed 2x/day vs. 6x/day for IR).
First-pass metabolism - when an orally absorbed drug is metabolized by the liver/gut wall before reaching systemic circulation - reduces bioavailability. Drugs with high first-pass effect (e.g., morphine, propranolol, lidocaine) may need much higher oral doses vs. IV.
2. Distribution
Movement of drug from bloodstream to tissues.
- Volume of Distribution (Vd) - hypothetical volume in which a drug is distributed. Large Vd = drug distributes widely into tissues (e.g., fat, muscle). Small Vd = drug stays in plasma.
- Plasma protein binding - drugs bound to albumin are pharmacologically inactive. Only free drug is active. Low albumin (e.g., elderly, malnourished) increases free drug and risk of toxicity.
- Blood-brain barrier (BBB) - only lipid-soluble, non-ionized drugs cross easily. Water-soluble drugs may require intrathecal injection to reach CNS.
- P-glycoprotein - efflux pump that pushes drugs OUT of cells. Reduces absorption and CNS penetration. Linked to multidrug resistance in cancer.
3. Metabolism (Biotransformation)
Primarily in the liver. Converts drugs to more water-soluble metabolites for excretion.
- CYP450 enzyme system - major pathway. Key isoforms: CYP3A4 (most common), CYP2D6, CYP1A2, CYP2C9
- Enzyme inducers (e.g., rifampin, carbamazepine, St. John's Wort) - speed up metabolism, reducing drug levels
- Enzyme inhibitors (e.g., erythromycin, fluconazole, grapefruit juice) - slow metabolism, raising drug levels and risk of toxicity
- Phase I reactions - oxidation, reduction, hydrolysis (often via CYP450) - may activate prodrugs or inactivate drugs
- Phase II reactions - conjugation (glucuronidation, sulfation) - makes drug more water-soluble
Nursing note: Hepatic impairment reduces first-pass metabolism and slows drug clearance - watch for toxicity.
4. Elimination
Removal of drug from the body.
- Kidneys - primary route for water-soluble drugs and metabolites. Renal impairment = drug accumulation.
- Half-life (t½) - time to reduce plasma concentration by 50%. Steady state is reached in ~5 half-lives.
- Clearance - volume of plasma cleared of drug per unit time.
Nursing note: In renal failure, renally-excreted drugs (e.g., gentamicin, digoxin, metformin) must be dose-reduced or avoided.
SECTION 2: PHARMACODYNAMICS (What the Drug Does to the Body)
- Agonist - binds receptor and activates it (mimics endogenous ligand)
- Antagonist - binds receptor and blocks it without activating it
- Partial agonist - activates receptor but less than a full agonist
- Therapeutic index (TI) - ratio of toxic dose to effective dose. Narrow TI drugs (e.g., digoxin, warfarin, lithium, aminoglycosides) require close monitoring.
- Tolerance - reduced drug effect with repeated use; requires higher doses
- Tachyphylaxis - rapid tolerance (hours/days)
- Adverse drug reactions (ADRs) - dose-related (predictable) or non-dose-related (hypersensitivity, idiosyncratic)
SECTION 3: CARDIOVASCULAR DRUGS
Antiarrhythmic Drugs (Vaughan-Williams Classification)
| Class | Mechanism | Key Drugs | Notes |
|---|---|---|---|
| Ia | Na+ channel block (moderate) - slows conduction, prolongs AP | Quinidine, procainamide, disopyramide | Prolongs QT |
| Ib | Na+ channel block (weak) - shorten AP | Lidocaine, mexiletine | Ventricular arrhythmias only |
| Ic | Na+ channel block (strong) - slows conduction greatly | Flecainide, propafenone | Only use in absence of structural heart disease |
| II | Beta-blockers - slow phase 4, decrease heart rate and AV conduction | Metoprolol, esmolol, propranolol | Post-MI, SVT, atrial fibrillation |
| III | K+ channel block - prolong repolarization | Amiodarone, sotalol, dronedarone, dofetilide | Amiodarone = broadest use including structural heart disease |
| IV | Ca2+ channel block - slow AV node conduction | Verapamil, diltiazem | SVT, rate control in A-fib |
Digoxin (not in Vaughan-Williams):
- Inhibits Na+/K+-ATPase, prolongs AV refractory period
- Used for rate control in A-fib, heart failure with reduced ejection fraction (HFrEF)
- Therapeutic range: 0.5-0.9 ng/mL (HF) or 1.0-2.0 ng/mL (A-fib/flutter)
- Digoxin toxicity signs: bradycardia, nausea/vomiting, visual changes (yellow-green halos, blurred vision), confusion, loss of appetite
- Risk factors for toxicity: hypokalemia, hypomagnesemia, renal impairment
- Treatment: digoxin immune Fab (Digibind)
Antihypertensives
| Drug Class | Examples | Mechanism | Key Nursing Points |
|---|---|---|---|
| ACE inhibitors | Lisinopril, enalapril | Block conversion of angiotensin I → II; reduce vasoconstriction and aldosterone | Dry cough (use ARB instead), hyperkalemia, contraindicated in pregnancy (teratogenic) |
| ARBs | Losartan, valsartan | Block angiotensin II receptor | Same as ACEi but no cough; also contraindicated in pregnancy |
| Beta-blockers | Metoprolol, atenolol | Block beta-adrenergic receptors, lower HR and cardiac output | Avoid abrupt withdrawal (rebound hypertension/angina); caution in asthma |
| Calcium channel blockers (CCBs) | Amlodipine (DHP), verapamil, diltiazem (non-DHP) | Block L-type Ca2+ channels | DHPs = peripheral vasodilation; non-DHPs = also slow heart rate. Verapamil causes constipation |
| Thiazide diuretics | Hydrochlorothiazide (HCTZ) | Inhibit Na+/Cl- cotransporter in distal tubule | Hypokalemia, hyponatremia, hyperuricemia (gout) |
| Loop diuretics | Furosemide, bumetanide | Inhibit Na+/K+/2Cl- cotransporter in loop of Henle | Potent diuresis, hypokalemia, ototoxicity (esp. IV furosemide), sulfa allergy cross-reactivity |
| K+-sparing diuretics | Spironolactone, eplerenone, amiloride | Block aldosterone or ENaC | Hyperkalemia risk; spironolactone = anti-androgen (gynecomastia) |
SECTION 4: CNS DRUGS
Analgesics
| Drug | Class | Mechanism | Key Points |
|---|---|---|---|
| Morphine, oxycodone, fentanyl | Opioids | Mu-opioid receptor agonists | Respiratory depression, constipation, miosis, euphoria. Naloxone reverses. High first-pass (morphine); transdermal fentanyl avoids. |
| Acetaminophen | Non-opioid analgesic | Inhibits prostaglandin synthesis centrally | Max 4g/day (3g/day in elderly, liver disease). Hepatotoxicity in overdose - treat with N-acetylcysteine |
| Ibuprofen, naproxen, ketorolac | NSAIDs | Inhibit COX-1 and COX-2 | GI ulcers (use PPI with chronic use), renal impairment, platelet inhibition, contraindicated in 3rd trimester pregnancy |
| Aspirin | NSAID | Irreversible COX-1 and COX-2 inhibition | Antiplatelet effect lasts 7-10 days (lifespan of platelet). Reye syndrome in children with viral illness. |
Antidepressants
| Class | Examples | Mechanism | Side Effects |
|---|---|---|---|
| SSRIs | Fluoxetine, sertraline, escitalopram | Inhibit serotonin reuptake | Nausea, insomnia, sexual dysfunction, serotonin syndrome (with other serotonergic agents), SIADH |
| SNRIs | Venlafaxine, duloxetine | Inhibit serotonin + norepinephrine reuptake | Similar to SSRIs + hypertension (high dose), urinary retention (NE effect) |
| TCAs | Amitriptyline, nortriptyline | Inhibit NE + 5-HT reuptake; also antihistamine, anticholinergic | Sedation, dry mouth, urinary retention, constipation, arrhythmia in overdose (QRS widening - treat with sodium bicarb) |
| MAOIs | Phenelzine, tranylcypromine | Inhibit monoamine oxidase | Tyramine-rich food avoidance (hypertensive crisis), multiple drug interactions |
| Bupropion | Atypical antidepressant | Inhibits NE + dopamine reuptake | No sexual dysfunction, lowers seizure threshold, used for smoking cessation |
| Mirtazapine | Atypical | Alpha-2 antagonist + antihistamine | Sedation, weight gain, no sexual dysfunction |
Serotonin syndrome - triad: altered mental status, autonomic instability, neuromuscular abnormalities (clonus, hyperreflexia). Treat by stopping offending agent; cyproheptadine for mild cases.
Antipsychotics
| Class | Examples | Notes |
|---|---|---|
| First-generation (typical) | Haloperidol, chlorpromazine, fluphenazine | D2 receptor blockade. Risk: EPS (dystonia, akathisia, parkinsonism, tardive dyskinesia), hyperprolactinemia, NMS |
| Second-generation (atypical) | Clozapine, olanzapine, quetiapine, risperidone, aripiprazole | Lower EPS risk. Metabolic syndrome (weight gain, dyslipidemia, hyperglycemia). Clozapine: agranulocytosis (requires WBC monitoring), seizures. |
Neuroleptic Malignant Syndrome (NMS) - hyperthermia, rigidity, altered mental status, autonomic instability. Medical emergency. Stop antipsychotic; give dantrolene, bromocriptine.
Extrapyramidal symptoms (EPS):
- Acute dystonia (hours-days) - treat with benztropine or diphenhydramine
- Akathisia - treat with propranolol or benzodiazepine
- Parkinsonism - reduce dose or switch drug
- Tardive dyskinesia (months-years) - may be irreversible; switch to clozapine or quetiapine
Benzodiazepines & Sedatives
| Drug | Use | Key Points |
|---|---|---|
| Diazepam, lorazepam, midazolam | Anxiety, seizures, alcohol withdrawal, procedural sedation | CNS depression, respiratory depression, physical dependence, tolerance. Flumazenil reverses. |
| Zolpidem | Insomnia | Non-BZD GABA-A modulator; less dependence than BZDs but risk still exists |
| Buspirone | Anxiety (chronic) | No sedation, no dependence, no cross-tolerance with BZDs. Slow onset (weeks). |
SECTION 5: RESPIRATORY DRUGS
| Drug Class | Examples | Mechanism | Key Points |
|---|---|---|---|
| SABA (Short-acting beta-2 agonist) | Albuterol, levalbuterol | Bronchodilation via beta-2 receptors | Rescue inhaler for acute bronchospasm. Tremor, tachycardia at high doses. |
| LABA (Long-acting beta-2 agonist) | Salmeterol, formoterol | Same mechanism, prolonged effect | Not for acute attack. Never use LABA alone in asthma (always with ICS). |
| ICS (Inhaled corticosteroids) | Fluticasone, budesonide, beclomethasone | Reduce airway inflammation | Rinse mouth after use (prevent oral candidiasis). First-line maintenance for asthma. |
| LAMA (Long-acting muscarinic antagonist) | Tiotropium, ipratropium | Block muscarinic receptors, reduce bronchoconstriction and secretions | Preferred for COPD maintenance. Dry mouth, urinary retention. |
| Leukotriene modifiers | Montelukast | Block leukotriene receptors | Oral, mild-moderate asthma or allergic rhinitis. |
| Methylxanthines | Theophylline | Phosphodiesterase inhibitor, bronchodilation | Narrow therapeutic index. Toxicity: seizures, arrhythmias. Monitor levels. |
SECTION 6: ANTIBIOTICS / ANTIMICROBIALS
| Class | Mechanism | Examples | Coverage/Key Points |
|---|---|---|---|
| Penicillins | Inhibit cell wall synthesis (bind PBPs) | Amoxicillin, ampicillin, piperacillin | Bactericidal. Allergy cross-reactivity with cephalosporins (~1%). |
| Cephalosporins | Inhibit cell wall synthesis | Cefazolin (1st), cefuroxime (2nd), ceftriaxone (3rd), cefepime (4th) | Broader coverage with each generation. 3rd/4th gen cover gram-negatives well. |
| Carbapenems | Inhibit cell wall synthesis | Meropenem, imipenem | Broadest beta-lactam spectrum. Reserved for resistant organisms. |
| Vancomycin | Inhibit cell wall synthesis (different site - binds D-Ala-D-Ala) | - | MRSA, C. diff (oral). Nephrotoxicity, ototoxicity, Red Man Syndrome (infusion-related, slow rate). |
| Aminoglycosides | Inhibit 30S ribosome | Gentamicin, tobramycin, amikacin | Bactericidal gram-negatives, synergy with beta-lactams. Nephrotoxicity, ototoxicity, neuromuscular blockade. Monitor levels. |
| Macrolides | Inhibit 50S ribosome | Azithromycin, erythromycin, clarithromycin | Atypicals (Mycoplasma, Legionella, Chlamydia). QT prolongation. CYP3A4 inhibitors (erythromycin, clarithromycin). |
| Fluoroquinolones | Inhibit DNA gyrase and topoisomerase IV | Ciprofloxacin, levofloxacin | Gram-negatives including Pseudomonas (cipro). QT prolongation, tendinopathy/tendon rupture (esp. with steroids), avoid in children. |
| Tetracyclines | Inhibit 30S ribosome | Doxycycline, minocycline | Atypicals, Lyme, MRSA (doxy). Avoid in pregnancy/children <8 years (teeth/bone deposition). Take with water, avoid dairy/antacids. |
| Sulfonamides/TMP-SMX | Inhibit folate synthesis | Trimethoprim-sulfamethoxazole | UTIs, PCP prophylaxis, MRSA. Hyperkalemia, bone marrow suppression, Steven-Johnson syndrome. Avoid in G6PD deficiency. |
| Metronidazole | DNA strand breakage (anaerobes/protozoa) | Flagyl | Anaerobes, C. diff, H. pylori, Trichomonas, Giardia. Disulfiram-like reaction with alcohol (avoid alcohol). |
| Antifungals | Ergosterol disruption | Fluconazole (azole), amphotericin B (polyene), nystatin | Amphotericin B: nephrotoxicity, infusion reactions (fever/chills - premedicate). Fluconazole: CYP inhibitor, drug interactions. |
SECTION 7: ENDOCRINE / DIABETES DRUGS
Insulin Types
| Type | Onset | Peak | Duration | Examples |
|---|---|---|---|---|
| Rapid-acting | 15 min | 30-90 min | 3-5 h | Lispro, aspart, glulisine |
| Short-acting (regular) | 30 min | 2-3 h | 6-8 h | Regular insulin |
| Intermediate-acting | 1-2 h | 4-8 h | 12-16 h | NPH insulin |
| Long-acting | 1-2 h | Peakless | 20-24 h | Glargine, detemir |
| Ultra-long-acting | 6 h | Peakless | 36-42 h | Degludec |
Nursing notes for insulin:
- Hypoglycemia is the main adverse effect - always have glucose source available
- Rotate injection sites to prevent lipodystrophy
- Glargine (Lantus) must NOT be mixed with other insulins
- Rapid-acting analogs given with meals; long-acting given once daily
Oral Antidiabetic Drugs
| Drug | Class | Mechanism | Key Points |
|---|---|---|---|
| Metformin | Biguanide | Decreases hepatic glucose production, increases insulin sensitivity | First-line for T2DM. GI side effects. Lactic acidosis risk - hold before contrast dye and in renal impairment (eGFR <30). |
| Glipizide, glibenclamide | Sulfonylureas | Stimulate insulin release from beta cells | Hypoglycemia, weight gain. |
| Sitagliptin | DPP-4 inhibitor | Increase incretin levels, stimulate insulin release | Well tolerated, weight neutral. Risk of pancreatitis. |
| Empagliflozin, dapagliflozin | SGLT2 inhibitors | Block glucose reabsorption in kidney; glucosuria | Cardiovascular and renal protective. Risk: UTI/genital yeast infections, DKA (even with normal glucose in T2DM), Fournier's gangrene. |
| Liraglutide, semaglutide | GLP-1 agonists | Stimulate insulin release (glucose-dependent), suppress glucagon, delay gastric emptying, reduce appetite | Weight loss benefit. Nausea/vomiting. Risk of pancreatitis, medullary thyroid cancer (avoid in MEN2/family history). |
SECTION 8: ANTICOAGULANTS
| Drug | Mechanism | Monitoring | Reversal |
|---|---|---|---|
| Heparin (UFH) | Activates antithrombin III (inhibits thrombin + Xa) | aPTT (target 60-100 sec) | Protamine sulfate |
| Low Molecular Weight Heparins (LMWH) | Activates antithrombin III (mainly inhibits Xa) | Anti-Xa (routine monitoring usually not required) | Protamine (partial) |
| Warfarin | Inhibits vitamin K-dependent clotting factors (II, VII, IX, X, protein C, S) | INR (target 2-3 for most indications) | Vitamin K, FFP, 4-factor PCC (Kcentra) for emergent reversal |
| Dabigatran | Direct thrombin inhibitor | No routine monitoring | Idarucizumab (Praxbind) |
| Rivaroxaban, apixaban | Direct Xa inhibitors | No routine monitoring | Andexanet alfa (AnxexXa) |
Heparin-Induced Thrombocytopenia (HIT): Platelet drop >50% within 5-10 days of starting heparin. Stop all heparin products. Switch to argatroban or bivalirudin. Do NOT give warfarin alone until platelets recover.
SECTION 9: GASTROINTESTINAL DRUGS
| Drug | Class | Mechanism | Use | Key Points |
|---|---|---|---|---|
| Omeprazole, pantoprazole | PPI | Irreversible H+/K+-ATPase inhibition | GERD, peptic ulcer, H. pylori (triple therapy) | Take 30-60 min before meal. Long-term risk: hypomagnesemia, C. diff, bone fractures, vitamin B12 deficiency |
| Ranitidine, famotidine | H2 blocker | Block H2 receptors on parietal cells | Mild-moderate GERD, peptic ulcer | Less potent than PPIs |
| Ondansetron | 5-HT3 antagonist | Block serotonin receptors in GI tract and CNS | Nausea/vomiting (chemo, post-op) | QT prolongation at high doses |
| Metoclopramide | Dopamine antagonist + prokinetic | Increase GI motility | GERD, gastroparesis | EPS/tardive dyskinesia risk with long-term use |
| Loperamide | Opioid receptor agonist | Decrease GI motility | Diarrhea | Does not cross BBB at therapeutic doses; no CNS effects |
SECTION 10: KEY NURSING PRINCIPLES IN PHARMACOLOGY
The "5 Rights" (expanded to 10)
- Right patient
- Right drug
- Right dose
- Right route
- Right time
- Right documentation
- Right reason
- Right response
- Right to refuse
- Right education
High-Alert Medications (requires extra caution)
- Insulin - hypoglycemia
- Anticoagulants (heparin, warfarin) - bleeding
- Concentrated electrolytes (KCl, NaCl 3%) - cardiac arrest if given incorrectly
- Opioids - respiratory depression
- Chemotherapy agents - cytotoxicity
Common Drug-Food Interactions
| Drug | Interaction | Avoid |
|---|---|---|
| Warfarin | Vitamin K foods reduce effect | Large amounts of leafy greens |
| MAOIs | Tyramine-containing foods cause hypertensive crisis | Aged cheese, cured meats, wine |
| Tetracyclines | Divalent cations reduce absorption | Dairy, antacids (calcium, magnesium) |
| Fluoroquinolones | Same as tetracyclines | Antacids, dairy, calcium-fortified foods |
| Metronidazole | Disulfiram-like reaction | All alcohol |
| Grapefruit juice | CYP3A4 inhibitor - increases drug levels | With statins, CCBs, cyclosporine, many others |
Pharmacokinetics in Special Populations
| Population | Consideration |
|---|---|
| Elderly | Decreased renal/hepatic function, lower albumin, altered Vd (more fat), polypharmacy risk. Use lower doses. |
| Pediatric | Use weight-based dosing (mg/kg). Immature liver enzymes. Avoid aspirin (Reye's), tetracyclines, fluoroquinolones. |
| Pregnancy | Avoid ACEi/ARBs (all trimesters), warfarin (1st/3rd trimester), tetracyclines, fluoroquinolones, NSAIDs (3rd trimester), thalidomide. Use heparin for anticoagulation. |
| Renal impairment | Reduce/avoid renally-excreted drugs: metformin, aminoglycosides, digoxin, vancomycin, LMWH. |
| Hepatic impairment | Reduce drugs with high first-pass or hepatic metabolism: morphine, warfarin, statins. |
QUICK REVIEW: ANTIDOTES
| Poison/Drug | Antidote |
|---|---|
| Opioids | Naloxone (Narcan) |
| Benzodiazepines | Flumazenil |
| Acetaminophen | N-acetylcysteine (NAC) |
| Heparin (UFH) | Protamine sulfate |
| Warfarin | Vitamin K / FFP / 4-factor PCC |
| Dabigatran | Idarucizumab (Praxbind) |
| Digoxin | Digoxin immune Fab (Digibind) |
| Beta-blocker overdose | Glucagon, calcium gluconate, high-dose insulin |
| TCAs (overdose) | Sodium bicarbonate (IV) |
| Iron poisoning | Deferoxamine |
| Lead poisoning | EDTA, dimercaprol, succimer |
| Organophosphates | Atropine + pralidoxime |
Sources: Lippincott Illustrated Reviews: Pharmacology (9781975170561); Katzung's Basic and Clinical Pharmacology, 16th Ed. (9781260463309)
Make a PowerPoint deck covering the major drug classes
Reading File
Reading File
Running Command
Writing File
Running Command
Running Command
Your deck is ready (969 KB, 22 slides):
Pharmacology Major Drug Classes
Presentation · PPTX
What's inside (22 slides, navy/teal/gold color scheme):
| # | Section | Slides |
|---|---|---|
| 1 | Pharmacokinetics & Pharmacodynamics | ADME overview, Routes of Administration table, PD key concepts |
| 2 | Cardiovascular | Vaughan-Williams antiarrhythmics table, Digoxin toxicity, Antihypertensives table |
| 3 | CNS Drugs | Analgesics table, Antidepressants table, Antipsychotics/EPS, Benzodiazepines |
| 4 | Respiratory | SABA/LABA/ICS/LAMA/theophylline table |
| 5 | Antibiotics | Cell wall inhibitors table, Protein/DNA inhibitors table |
| 6 | Endocrine / Diabetes | Insulin types table, Nursing essentials, Oral antidiabetics table |
| 7 | Anticoagulants | Overview table, HIT + bleeding nursing alerts |
| 8 | GI Drugs | PPIs/H2B/antiemetics/prokinetics/antidiarrheals table |
| 9 | Antidotes & Nursing | Full antidotes table, Special populations (two-column), 10 Rights, High-alert medications |
This is a shared conversation. Sign in to Orris to start your own chat.