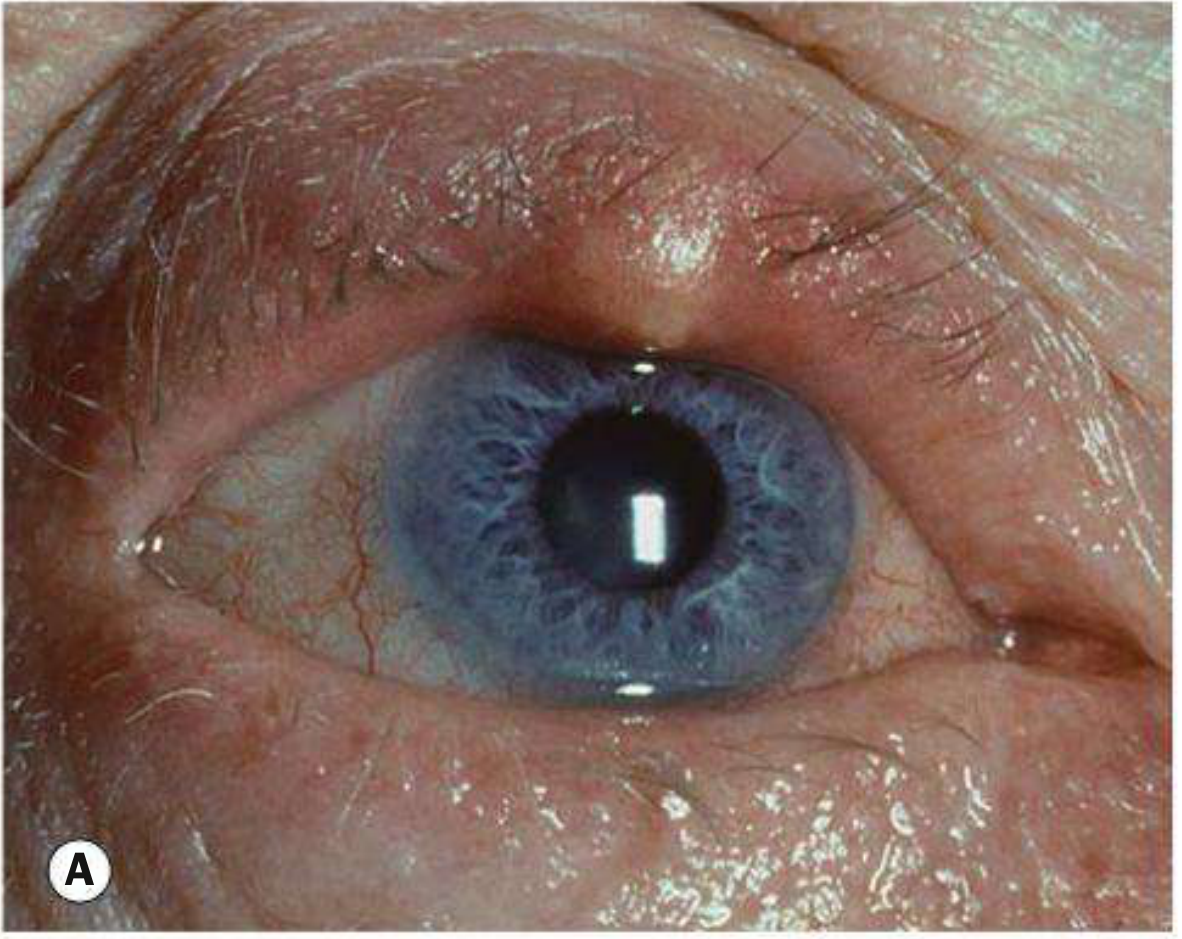
A generalized painful swelling on the upper eyelid which has occurred most probably due to rubbing the eye
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information. Here is the full answer:
Acute Hordeolum (Stye) - Upper Eyelid
The clinical picture you describe - generalized painful swelling of the upper eyelid following eye rubbing - is most consistent with an internal hordeolum, though the rubbing mechanism can also precipitate preseptal (periorbital) cellulitis if the skin barrier is disrupted.
Most Likely Diagnosis: Internal Hordeolum

Types of Hordeolum
| Feature | External Hordeolum (Stye) | Internal Hordeolum |
|---|---|---|
| Gland affected | Zeis (sebaceous) or Moll (sweat) gland at lash follicle | Meibomian gland within tarsal plate |
| Location of pointing | Anterior - through the skin at the lid margin, usually with a lash at apex | Posterior - points toward the inner (conjunctival) surface of the tarsal plate |
| Cause | Acute Staphylococcus abscess | Acute Staphylococcal infection of meibomian gland |
| Swelling extent | Usually localized to the lid margin | Can cause more diffuse/generalized lid swelling |
| Pain | Painful, tender | Painful, tender - similar to external |
The key point for your case: generalized painful swelling (rather than a discrete small pustule at the lash line) after eye rubbing points more toward an internal hordeolum or early preseptal cellulitis.
- Rosen's Emergency Medicine notes: "A hordeolum is caused by acute inflammation of an oil (Zeis or meibomian) gland or hair follicle. It is typically painfully tender, erythematous, associated with swelling, and can be infected."
- Kanski's Clinical Ophthalmology explains: "An external hordeolum presents as a tender swelling in the lid margin pointing anteriorly through the skin, usually with a lash at its apex. Multiple lesions may be present and occasionally an abscess may involve the entire lid margin."
Why Eye Rubbing is the Precipitant
Eye rubbing directly inoculates Staphylococcus aureus (the dominant pathogen, carried on skin and fingertips) into:
- Lash follicles and adjacent Zeis/Moll glands (external hordeolum)
- Meibomian gland orifices (internal hordeolum)
Rubbing also breaks the skin barrier, raising the risk of spreading infection beyond the gland itself into the preseptal space (preseptal cellulitis).
Differential Diagnoses to Consider
| Condition | Key Distinguishing Feature |
|---|---|
| Chalazion | Chronic, sterile, granulomatous - usually not acutely painful; may evolve from a hordeolum |
| Preseptal cellulitis | Diffuse lid erythema, warmth, tenderness, low-grade fever - no discrete abscess/pustule |
| Orbital (postseptal) cellulitis | Proptosis, ophthalmoplegia, pain on eye movement, chemosis - a dangerous diagnosis |
| Blepharitis | Diffuse lid margin inflammation, itching/burning, crusting; not a discrete lump |
| Allergic reaction | Swelling + redness without pain/fever, history of allergen exposure (makeup, soaps) |
Important red flag: If the swelling is accompanied by proptosis, restricted eye movement, pain on moving the eye, or fever - suspect postseptal (orbital) cellulitis, which requires urgent CT imaging and IV antibiotics.
Management
First-line (conservative):
- Warm compresses applied for 10-15 minutes, 3-5 times daily - promotes spontaneous drainage
- Topical antibiotics: Erythromycin ophthalmic ointment twice daily for 7-10 days
- Do not squeeze or manually express the lesion
Escalation:
- Oral antibiotics if significant surrounding cellulitis (e.g., amoxicillin-clavulanate or a macrolide)
- Epilation of the associated eyelash can help in external hordeolum
- Incision and drainage - refer to ophthalmologist if the lesion does not respond to conservative treatment
- Recurrent or nonresponsive cases warrant ophthalmology review (and biopsy if needed to exclude sebaceous cell carcinoma masquerading as a chronic lesion)
Sources: Tintinalli's Emergency Medicine, p. 1581 | Rosen's Emergency Medicine, pp. 893-894 | Kanski's Clinical Ophthalmology (10th ed.), p. 81
There is no lesion, just generalized swelling
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Thank you for the clarification. With no discrete lesion - just diffuse, generalized swelling of the upper eyelid after eye rubbing - the diagnosis shifts significantly. Here is the updated picture:
Revised Diagnosis: Preseptal (Periorbital) Cellulitis
The combination of generalized painful swelling (without a focal pustule or nodule) of the upper eyelid, precipitated by rubbing the eye, is most consistent with preseptal cellulitis - a soft-tissue infection of the eyelid anterior to the orbital septum.

Eye rubbing introduces skin flora (predominantly S. aureus, Streptococcus) through micro-abrasions in the eyelid skin, seeding the preseptal soft tissue.
Preseptal Cellulitis - Key Features
| Feature | Detail |
|---|---|
| Location | Anterior to the orbital septum (eyelid skin and soft tissue only) |
| Swelling | Diffuse, tense edema of the entire eyelid - no focal lesion |
| Pain | Present, with warmth and erythema |
| Precipitant | Trauma, rubbing, skin abrasion, insect bite, spread from adjacent infection |
| Organisms | S. aureus, Streptococcus; consider H. influenzae in non-immunized children |
| Fever | May be present, especially in children |
Critical distinguishing signs (all absent in preseptal cellulitis):
- No proptosis
- No restricted eye movement (ophthalmoplegia)
- No pain on moving the eye
- No chemosis (conjunctival edema)
- Vision is intact
If any of these are present, suspect postseptal (orbital) cellulitis - a sight-threatening emergency requiring urgent CT and IV antibiotics.
The Rubbing Mechanism
Eye rubbing causes micro-abrasions in the thin eyelid skin, allowing normal skin commensals to inoculate the preseptal soft tissue. The Wills Eye Manual explicitly lists "local skin abrasions" and "trauma" as direct precipitants of preseptal cellulitis. Andrews' Diseases of the Skin notes that rubbing and scratching secondary to allergic conjunctivitis is also a recognized route.
Differential Diagnosis (no focal lesion, generalized swelling)
| Condition | Key Distinguishing Features |
|---|---|
| Preseptal cellulitis | Painful, warm, erythematous, tense diffuse swelling; history of trauma/rubbing |
| Allergic eyelid edema / angioedema | Sudden onset, non-tender, itchy, no warmth or erythema; often bilateral |
| Contact dermatitis | Itching > pain, history of allergen exposure (makeup, eye drops, soaps); eczematous skin changes |
| Insect bite | Rapid onset, often history of outdoor exposure; may be non-tender initially |
| Orbital cellulitis | Proptosis + restricted motility + pain on eye movement - postseptal extension |
| Viral conjunctivitis | Secondary eyelid swelling with follicular conjunctivitis present |
| Angioedema | Non-pitting, non-tender, no erythema; may have systemic allergic features |
Workup
- Full ocular exam: check eye movements, proptosis, pupil reflexes, visual acuity
- Check facial sensation (V1/V2 trigeminal distributions)
- Palpate regional lymph nodes
- Vital signs - fever suggests systemic infection
- CT orbits with contrast if any concern for postseptal spread, sinusitis, or significant trauma
- Blood cultures + CBC if febrile or severe
Treatment (Preseptal Cellulitis)
Mild (afebrile, outpatient, >5 years old):
- Amoxicillin/clavulanate 875/125 mg PO q12h (adults), or
- Cefpodoxime 200 mg PO q12h, or Cefdinir 600 mg PO daily
- If MRSA suspected: Trimethoprim-sulfamethoxazole or Clindamycin 450 mg PO TID
If allergic reaction is suspected instead:
- Oral antihistamine (cetirizine/loratadine)
- Short course topical/oral corticosteroid
- Identify and remove allergen
Follow-up: All patients need review in 24-48 hours to ensure the swelling is resolving and not progressing toward orbital involvement.
Sources: Wills Eye Manual (6.10 Preseptal Cellulitis), pp. 403-408 | Andrews' Diseases of the Skin (Eyelid Dermatitis) | Rosen's Emergency Medicine, p. 893-894
This is a shared conversation. Sign in to Orris to start your own chat.