Radiology -Imaging congenital renal abnormalities and lesions 1.embryology 2. Classification 3. Imaging protocol ct and MRI 4. Renal agenesis and associated syndromes 5. Renal hypoplasia,suprapneumary kidney, cross fused ectopia it's types 6. Abnormal positioned kidney ,renal ectopia 7. Fusion abnormalities 8. Duplex pelvic calyces system 8. Normal mimicer 9. All cystic renal dysplasia and it's association
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching the Web
CT MRI protocol congenital renal anomalies imaging radiology 2024
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Here is a complete, organized reference covering all the topics you requested.
Radiology - Imaging of Congenital Renal Abnormalities
1. Embryology
The kidney develops through three sequential phases:
- Pronephros (weeks 3-4): rudimentary, non-functional, completely regresses
- Mesonephros (weeks 4-8): temporarily functional, gives rise to the Wolffian (mesonephric) duct
- Metanephros (week 5+): the permanent kidney, arising from two elements:
- Ureteric bud: outgrowth of the Wolffian duct - forms ureter, renal pelvis, calyces, and collecting ducts
- Metanephric blastema (mesenchyme): forms nephrons, glomeruli, and tubules
Key events:
- Ureteric bud must contact the metanephric mesenchyme at precisely the right time - early or late budding leads to renal malformations, dysplasia, hypoplasia, or agenesis
- Weeks 6-9: kidneys ascend from pelvis to L1-L2 retroperitoneum with 90° medial rotation (hilum faces anteromedially)
- Arterial supply shifts progressively cranially; failure of earlier arteries to involute = accessory renal arteries (~30% unilateral, 10% bilateral)
- Failure of ascent = ectopic kidney; failure of fusion arrest at midline = horseshoe/fused kidney
Key molecular regulators:
| Pathway | Role | Clinical relevance |
|---|---|---|
| GDNF/RET | GDNF (from mesenchyme) activates RET on ureteric bud, drives branching | Loss → agenesis |
| EYA1/SIX1 | Metanephric mesenchyme transcription; also expressed in ear/branchial tissue | Mutations → BOR syndrome |
| SHH/GLI3 | Hedgehog signaling regulates ureteric branching | Loss → agenesis (Smith-Lemli-Opitz, Pallister-Hall) |
2. Classification
Renal abnormalities are sub-classified by six categories:
| Category | Examples |
|---|---|
| Number | Agenesis, supernumerary kidney |
| Size/Parenchyma | Hypoplasia, dysplasia |
| Position | Pelvic/iliac/thoracic ectopia, malrotation |
| Fusion | Horseshoe kidney, crossed fused ectopia, pancake kidney |
| Collecting system | Duplex system, ureterocele, UPJ obstruction, bifid pelvis |
| Cystic | ADPKD, ARPKD, MCDK, obstructive dysplasia, simple cysts |
3. Imaging Protocol - CT and MRI
First-line: Ultrasound
- Antenatal US: most anomalies first detected here
- Normal kidney: slightly less echogenic than liver (difference increases with age)
- Neonatal corticomedullary differentiation can mimic hydronephrosis (normal)
- Fetal lobulation visible up to age 5
CT Urography (CTU) Protocol
| Phase | Timing | Purpose |
|---|---|---|
| Non-contrast | Baseline | Calculi, gross anatomy |
| Arterial/corticomedullary | 25-30 s | Vascular supply, accessory arteries (pre-op) |
| Nephrographic | 70-100 s | Parenchymal assessment, fusion anomalies, isthmus |
| Excretory/urographic | 5-10 min | Collecting system: duplication, ureterocele, ectopic insertion, UPJ |
- Multiplanar reconstructions (coronal, sagittal) are mandatory for positional and fusion anomalies
- CTU is the gold standard for complex collecting system anomalies in adults
MRI / MR Urography (MRU)
- Preferred in children and pregnancy (no radiation)
- T2 HASTE/SSFSE coronal: collecting system, fusion, position (bright urine)
- T1 pre/post gadolinium: parenchymal enhancement, function
- Static MRU: heavy T2-weighted, no contrast - outlines dilated collecting systems
- Excretory MRU: gadolinium + furosemide - functional and anatomical mapping
- DWI: adjunct for cystic lesion characterization and dysplastic kidney assessment
Nuclear Medicine
- DMSA scan: cortical scarring, split function, confirms ectopic/fused renal tissue
- MAG3/DTPA diuretic renogram: UPJ obstruction assessment
- VCUG: VUR, posterior urethral valves, ureterocele
4. Renal Agenesis and Associated Syndromes
Unilateral renal agenesis (1 in 500-1,000 births): failure of ureteric bud to join metanephric blastema; absent/rudimentary ipsilateral ureter in most cases.
| Population | Associated anomalies |
|---|---|
| Males (up to 70%) | Absent epididymis, vas deferens, seminal vesicle; seminal vesicle cyst |
| Females (70%) | Müllerian anomalies: vaginal/uterine agenesis, unicornuate uterus = MRKH syndrome |
| All (10%) | Absent ipsilateral adrenal gland |
| All | VACTERL; Turner syndrome; trisomy 21/22; cardiac, skeletal anomalies |
Imaging clue on plain film: Left renal agenesis - splenic flexure lies medially to the lesser curve of the stomach (bowel occupies renal fossa)
Bilateral renal agenesis (1 in 4,000 births): Potter sequence - oligohydramnios → pulmonary hypoplasia + facial anomalies (low-set ears, broad flat nose, prominent infraorbital folds)
Associated syndromes:
| Syndrome | Gene | Renal phenotype |
|---|---|---|
| BOR (Branchio-Oto-Renal) | EYA1, SIX1 | Agenesis, hypodysplasia, VUR, duplication |
| Fraser syndrome | FRAS1, FREM2 | Bilateral agenesis/hypoplasia |
| Pallister-Hall | GLI3 | Agenesis, dysplasia, hydronephrosis |
| Smith-Lemli-Opitz | DHCR7 | Agenesis, hypodysplasia |
| Okihiro (radial ray) | SALL4 | Unilateral agenesis, VUR, cross-fused ectopia |
5. Renal Hypoplasia, Supernumerary Kidney, and Cross-Fused Ectopia
Renal Hypoplasia
- Small kidney with reduced nephron number - developmental arrest in first trimester
- Distinct from dysplasia (abnormal tissue patterning) and acquired atrophy (irregular scarred surface)
- Imaging: Small, smooth kidney; preserved but diminished parenchyma; may show hyperechoic cortex or small cysts on US
Supernumerary Kidney
- Extra kidney (beyond the normal pair); rare
- Usually on the left (probable ureteric bud duplication)
- Located caudal to the normal kidney
- Drained by a separate ureter or a branch of a bifid ureter
- CT/MRU: separate renal unit with its own parenchyma, collecting system, and vascular supply
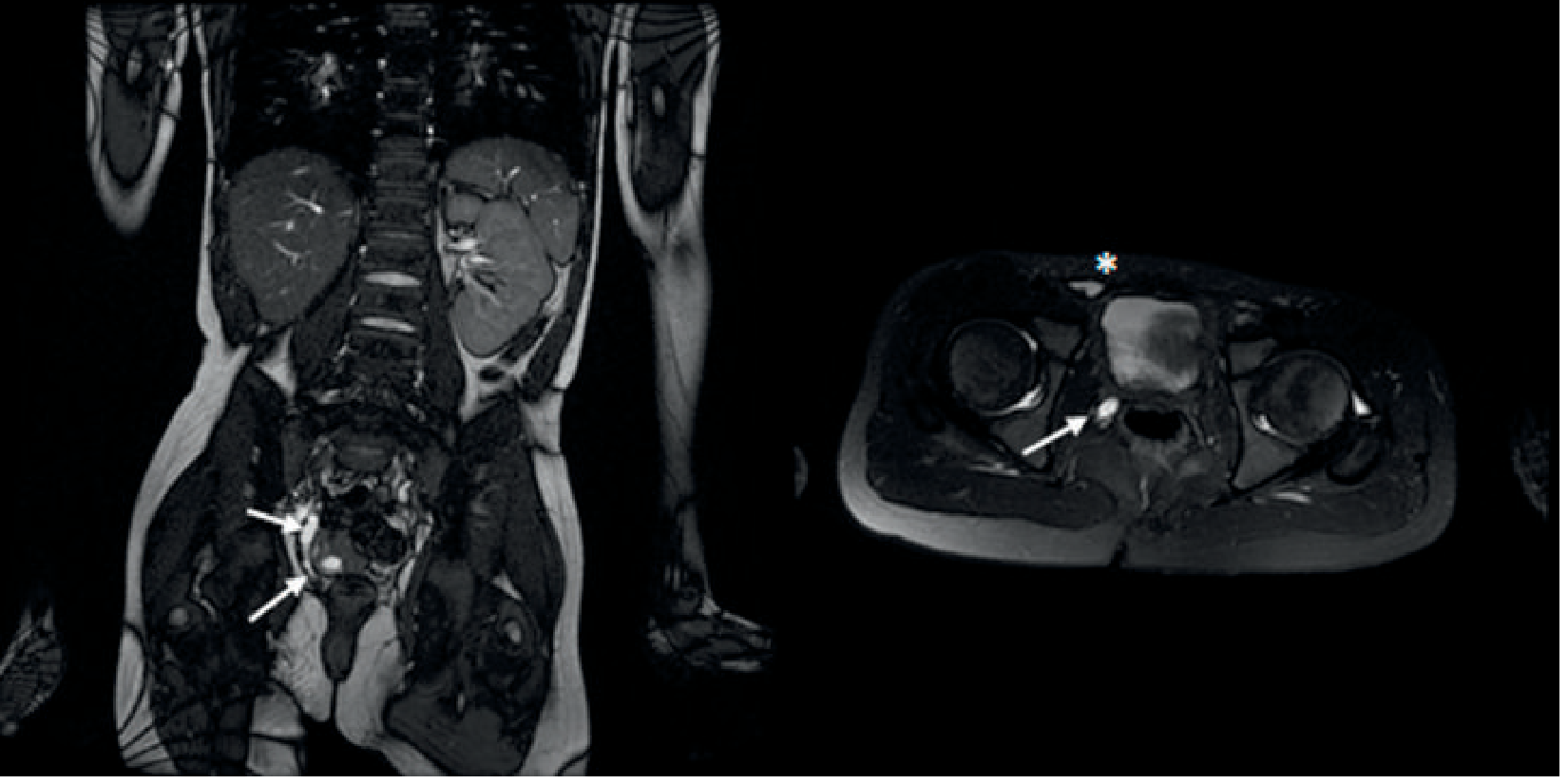
Cross-Fused Renal Ectopia
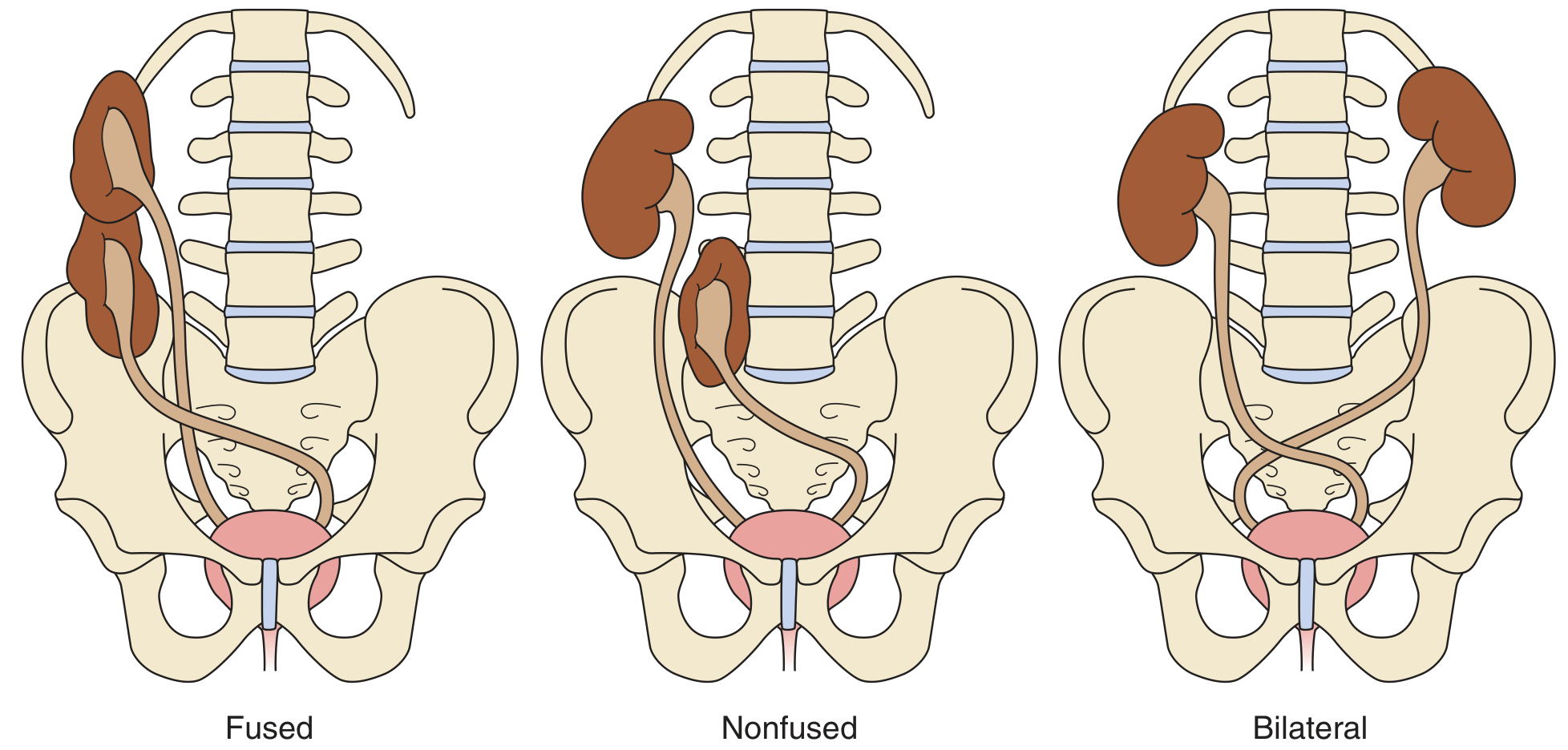
| Type | Description |
|---|---|
| Crossed fused (most common) | Kidney migrates across midline, fuses to the lower pole of the contralateral kidney |
| Simple crossed (nonfused) | Kidney crosses midline, does not fuse; lies at the pelvic rim |
| Bilateral ectopia | Both kidneys cross the midline; native ureters still insert normally into the bladder |
- More common in males; the left kidney is more commonly the ectopic one
- The ectopic kidney's ureter crosses the midline and inserts ipsilaterally into the bladder
- Complications: UPJ obstruction, stones, VUR, infection
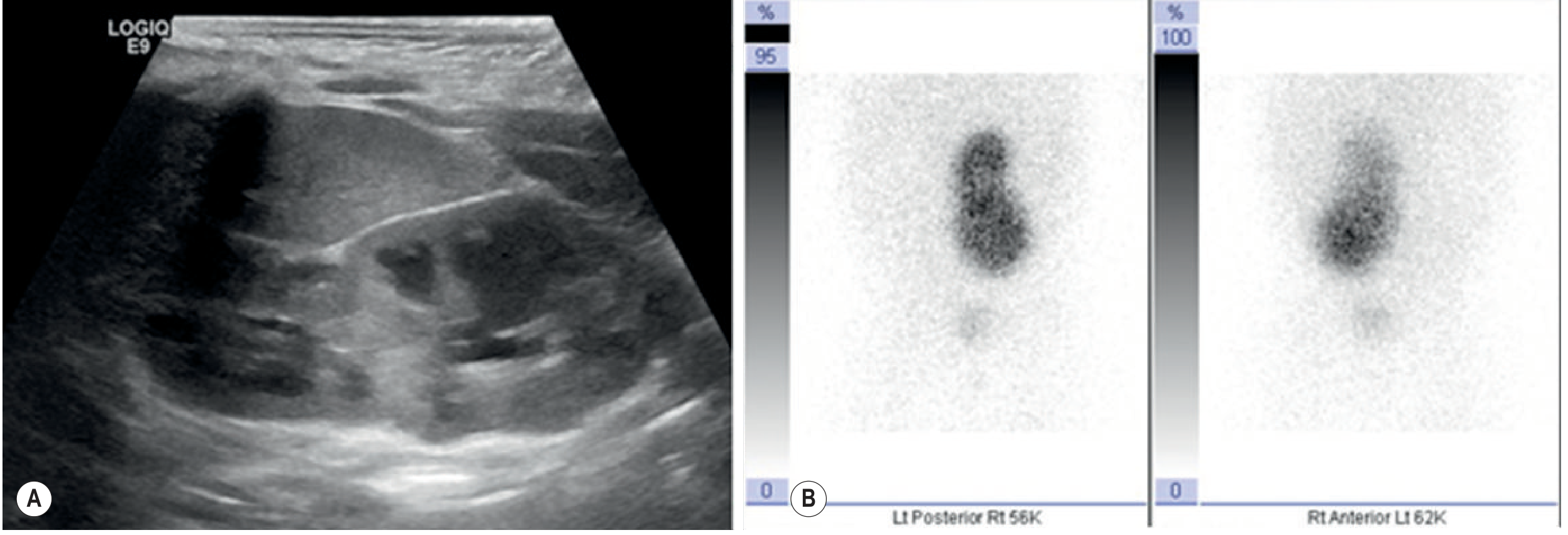
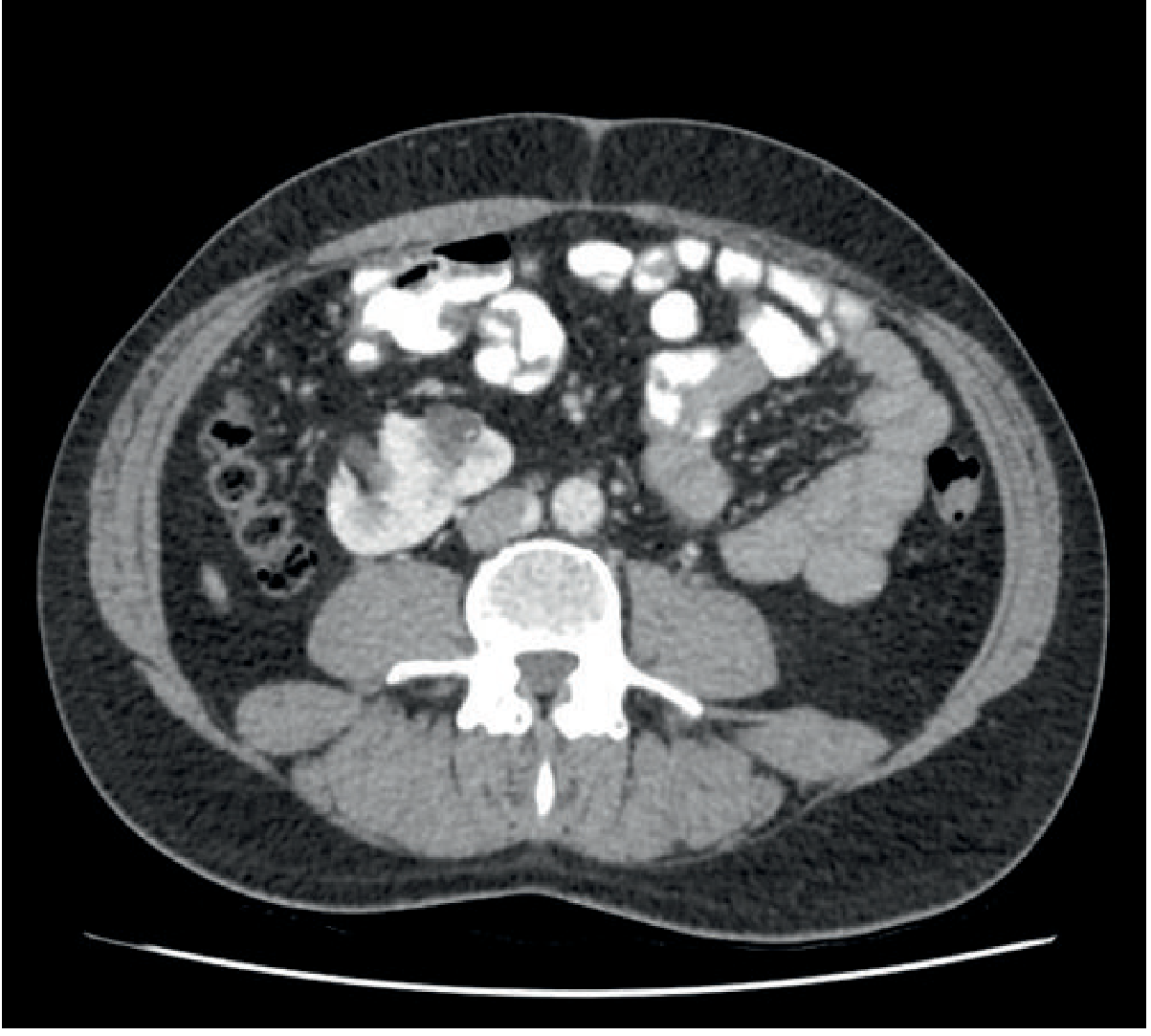
Imaging:
- US: parenchymal band between kidneys; abnormal position
- DMSA: confirms functional renal tissue in the ectopic location
- CT/MRU: defines fusion, vascular supply, collecting system
6. Abnormally Positioned Kidney / Renal Ectopia
Normal ascent: pelvis → L1-2 retroperitoneum, with 90° medial rotation. Failure at any point = ectopia.
| Position | Notes |
|---|---|
| Pelvic kidney | Most common ectopic type; true pelvis; prone to UPJ obstruction, trauma |
| Iliac kidney | Iliac fossa |
| Abdominal/lumbar | Between pelvis and normal position |
| Thoracic kidney | Rare; through Bochdalek diaphragmatic defect; diagnosed on chest X-ray/CT |
| Crossed ectopia | Crosses midline (see above) |
Complications: Decreased function, UPJ obstruction, VUR, nephrolithiasis, increased trauma risk.
Malrotation: Abnormal rotation around the long axis; UPJ faces anteriorly (most common); may cause extrinsic obstruction.
Imaging approach: If kidney absent in retroperitoneal fossa, systematically scan pelvis, iliac fossa, and mediastinum. CT/MRI define position, vasculature (multiple anomalous vessels common), and collecting system. DMSA confirms function.
7. Fusion Abnormalities
Horseshoe Kidney
- Most common fusion anomaly: 1 in 400-1,000 births; 2:1 male predominance
- Both kidneys (usually lower poles, 90%) fuse across the midline during ascent
- The isthmus lies anterior to the aorta and IVC, posterior to the inferior mesenteric artery (IMA) - which halts further ascent
- Isthmus composition: fibrous or functioning parenchyma (85-95%)
- Lower poles point medially (reversed renal axes)
Associations:
- Turner syndrome (7%), trisomy 18, trisomy 21, neural tube defects
- UPJ obstruction (high ureteric insertion), VUR, nephrolithiasis
- Increased risk: Wilms tumor, carcinoid, transitional cell carcinoma, lymphoma
Pancake (Disc) Kidney
- Bilateral pelvic kidneys that fuse anteriorly, producing a single flat pelvic renal mass with two collecting systems
Other Fusion Types (variants of crossed fused ectopia)
- Sigmoid/S-shaped kidney: the two kidneys fuse at opposite poles
- L-shaped kidney: perpendicular configuration
- Lump/cake kidney: irregular complete fusion
8. Duplex Pelvicalyceal System (Ureteral Duplication)
Most common congenital urinary tract anomaly: incidence 0.8-5%
Arises when two separate ureteric buds develop from a single Wolffian duct.
Types
- Partial (bifid) duplex:
- Bifid pelvis: two pelvices joined proximal to UPJ
- Y-ureter (bifid ureter): ureters join distal to UPJ; can cause yo-yo (ureteroureteral) reflux if one segment disproportionately enlarged
- Complete duplex: two entirely separate ureters from kidney to bladder (or ectopically)
Weigert-Meyer Rule
Upper moiety ureter inserts ectopically - below and medial to the normal orifice, sometimes extravesical. Lower moiety ureter inserts normally (above and lateral).
- Upper pole: tends to obstruct (ectopic/ureterocele)
- Lower pole: tends to reflux (laterally displaced orifice, shorter submucosal tunnel)
Ureterocele
- Cystic dilatation of the intravesical distal ureter
- Orthotropic (simple): at normal position; typically in adults; usually asymptomatic
- Ectopic: in duplex system, upper moiety, inserts below trigone; more common in females; may prolapse into urethra
- Cobra-head / spring-onion sign on IVU or CTU
Imaging approach:
- US: echogenic band (column of Bertin) between moieties; dilated upper pole in obstruction; ureterocele as thin-walled cyst at bladder base
- CTU/MRU: full anatomical map of both moieties, ureteric courses, insertion sites
- VCUG: VUR into lower moiety; may opacify ureterocele
- Approximately 1/3 of patients with complete duplication have an additional congenital anomaly
9. Normal Mimickers
| Mimicker | What It Simulates | Key Distinguishing Features |
|---|---|---|
| Persistent fetal lobulation | Renal mass or cortical scar | Regular scalloping along inter-lobar septa; no parenchymal loss; isoechoic/isodense to cortex |
| Column of Bertin (prominent septum) | Cortical mass / pseudotumor | Isoechoic to cortex on US; isodense on all CT phases; located between pyramids; no mass effect; normal enhancement on contrast CT |
| Dromedary hump | Left renal mass | Left lateral cortical bulge from splenic impression; isodense to rest of cortex on all CT phases |
| Junctional parenchymal defect | Cortical scar or angiomyolipoma | Triangular hyperechoic/fat-containing defect at upper pole anteriorly (junction of lobar units); contains fat on CT |
| Extrarenal pelvis | Hydronephrosis | Pelvis extends outside sinus; calyces normal caliber; no obstruction on renogram |
| Corticomedullary differentiation in neonates | Hydronephrosis/dilated calyces | Normal US appearance; hypoechoic medullary pyramids; resolves with age |
| Accessory renal arteries | Pathological vascular structure | Normal variant (~30% unilateral); supplies lower pole; critical to identify pre-operatively (can cross UPJ causing obstruction) |
| Retro-aortic / circum-aortic left renal vein | Venous obstruction | Normal variant; no associated renal deformity; gonadal/adrenal veins drain differently |
10. Cystic Renal Dysplasia - Full Spectrum and Associations
Renal Dysplasia (General Definition)
Abnormality of tissue patterning: decreased nephron number, loss of corticomedullary differentiation, metaplastic transformation of mesenchyme to cartilage/bone, disorganized stroma.
Multicystic Dysplastic Kidney (MCDK)
- Extreme form: kidney almost entirely replaced by large polymorphic non-communicating cysts, no identifiable renal pelvis, no functioning parenchyma
- Incidence ~1 in 4,000; more common in males; usually unilateral
- Natural history: gradual spontaneous involution
- Antenatal US: large peripheral cysts, no parenchyma
- DMSA: absent/minimal function
- Associations: contralateral UPJ obstruction (~5-10%), VUR, contralateral hypoplasia
Obstructive Cystic Renal Dysplasia
- Due to prolonged gestation urinary obstruction (posterior urethral valves, ureterocele, urethral agenesis)
- US: hyperechoic thinned cortex, loss of corticomedullary differentiation, dilated collecting system, parenchymal cysts
Autosomal Recessive PKD (ARPKD)
- PKHD1 gene, chromosome 6; 1 in 20,000 births
- Kidneys: cystic dilatation of collecting ducts → microcysts <2 mm
- Liver: congenital hepatic fibrosis, Caroli disease, portal hypertension
- Early US: bilaterally enlarged echogenic kidneys (microcysts too small to resolve); oligohydramnios antenatally
- With age: cysts become large enough to see individually
Autosomal Dominant PKD (ADPKD)
- PKD1 (chr 16, ~85%) and PKD2 (chr 4, ~15%); 1 in 400-1,000 births
- Most common inherited cause of ESRD
- Imaging: bilaterally enlarged kidneys, innumerable cysts of variable size
Extra-renal associations:
- Intracranial (berry) aneurysms (~10%)
- Colonic diverticulosis
- Mitral and aortic valve dysfunction
- Aortic dissection
- Von Meyenberg complexes (biliary hamartomas)
- Cysts in liver, spleen, pancreas
Medullary Sponge Kidney (MSK)
- Cystic dilatation of medullary collecting tubules
- Associated with nephrocalcinosis and recurrent stones
- CTU/IVU: "paintbrush" or "bouquet of flowers" - contrast fills dilated tubules
Nephronophthisis
- Autosomal recessive; most common genetic cause of ESRD in children
- Small/normal-sized kidneys; corticomedullary cysts; loss of differentiation
- Associated with: retinal dystrophy (Senior-Løken syndrome), Joubert syndrome (cerebellar vermis hypoplasia)
Summary Table - Cystic Renal Diseases
| Condition | Inheritance | Gene | Cyst Location | Key Associations | US Appearance |
|---|---|---|---|---|---|
| ARPKD | AR | PKHD1 (chr 6) | Collecting ducts (<2mm microcysts) | Hepatic fibrosis, Caroli, portal HTN | Enlarged echogenic kidneys |
| ADPKD | AD | PKD1/PKD2 | All nephron segments | Berry aneurysms, liver/pancreas cysts | Bilateral enlarged, innumerable cysts |
| MCDK | Sporadic | -- | Large non-communicating cysts | Contralateral UPJ obstruction, VUR | Cysts without pelvis, involutes |
| Obstructive dysplasia | Acquired (obstruction) | -- | Parenchymal + dilated system | PUV, ureterocele | Echogenic cortex, dilated system |
| Nephronophthisis | AR | NPHP1-20 | Corticomedullary interface | Senior-Løken, Joubert syndrome | Small kidneys, interface cysts |
| Medullary sponge | Sporadic/AD | -- | Collecting tubules (medullary) | Nephrocalcinosis, stones | Echogenic medullary pyramids |
| Simple cysts | Acquired | -- | Cortex/medulla | -- | Anechoic, posterior acoustic enhancement |
References:
- Grainger & Allison's Diagnostic Radiology, Chapters 27-28 (Congenital Abnormalities of the Urinary Tract; Congenital Cystic Renal Disease)
- Brenner & Rector's The Kidney, Chapter 72 (Spectrum of Kidney and Urinary Tract Disorders in Children)
- Campbell-Walsh Wein Urology (CAKUT genetics, Radiologic Anatomy of the Renal Parenchyma)
This is a shared conversation. Sign in to Orris to start your own chat.