MI 3.7 - Kala-azar (Visceral Leishmaniasis): Leishmania donovani, diagnosis, treatment • MI 3.8 - Filariasis: Wuchereria bancrofti, life cycle, diagnosis In dono competency ko mujhe apporba sastry book ke according conceptually samjhao poori detail me concepts and flowchart and pnemonics ke saath
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive data for both topics. Let me now compose the full, detailed, exam-oriented response with flowcharts, mnemonics, and conceptual explanations in the style expected for Apurba Sastry's Microbiology (the library doesn't have this specific book, but the content from Murray's Medical Microbiology 9e, Jawetz, and Harrison's covers the same syllabus topics).
🔬 MI 3.7 - Kala-azar (Visceral Leishmaniasis)
Note: Apurba Sastry's book is not in the digital library, but the content below is based on Murray's Medical Microbiology 9e, Jawetz Microbiology 28e, and Harrison's 22e - which cover the same MBBS competency topics. The concepts align with Apurba Sastry's syllabus framework.
🧠 CONCEPT FIRST: What Is Leishmania donovani?
Leishmania donovani ek obligate intracellular parasite hai jo macrophages ke andar rehta hai. Iska "kala-azar" naam Hindi se aata hai - "black fever" - kyunki chronic cases mein skin dark ho jaati hai (melanin ka deposition due to adrenal involvement).
🦟 THE ORGANISM - Morphology
Dono forms yaad karo - "PAM" mnemonic:
P - Promastigote (sandfly mein / culture mein)
A - Amastigote (human macrophage mein)
M - Macro size difference
| Feature | Promastigote | Amastigote |
|---|---|---|
| Kahan | Sand fly (gut), NNN medium | Human macrophage cytoplasm |
| Shape | Elongated, flagellated | Oval, non-flagellated |
| Size | 15-20 μm | 2-4 μm |
| Also called | Leptomonad form | Leishman-Donovan (LD) body |
| Infective to? | Human (inoculated by sandfly) | Sandfly (when it bites) |
🎯 Key Point: LD Bodies
- Amastigotes = LD bodies (Leishman-Donovan bodies)
- Nucleus = "dot", Kinetoplast = "dash" → "dot-dash" appearance
- Found intracellularly in macrophages of spleen, liver, bone marrow, lymph nodes
🔄 LIFE CYCLE - Flowchart
SAND FLY BITES HUMAN
↓
Promastigotes deposited in skin
↓
Phagocytosed by skin macrophages
↓
Transform into AMASTIGOTES (LD bodies)
↓
Multiply inside macrophage → Cell bursts
↓
Released amastigotes → phagocytosed by new macrophages
↓
Spread via RES: Spleen → Liver → Bone Marrow → Lymph nodes
↓
↕ [When sandfly bites infected human]
Sandfly ingests amastigotes in blood meal
↓
In sandfly gut: Amastigotes → Promastigotes (flagellated)
↓
Promastigotes multiply → migrate to proboscis
↓
Ready to infect next human (INFECTIVE STAGE = Promastigote)
🦟 Vector: Phlebotomus argentipes (India/South Asia)
- Only female sand fly bites (for blood meal)
- Bites at dusk/dawn (crepuscular)
- Cannot fly in wind >1 m/s (small, fragile)
🌍 EPIDEMIOLOGY
Mnemonic: "BINS" countries = 90% burden
- B - Bangladesh
- I - India (Bihar highest)
- N - Nepal
- S - Sudan
India has achieved 98.7% decline in VL incidence (WHO elimination program). Bihar was the epicenter due to widespread antimonial resistance.
Reservoir:
- India: Humans only (anthroponotic) → so vector control + treatment = elimination possible
- Mediterranean/Americas: Dogs, foxes, jackals (zoonotic, L. infantum) → harder to eliminate
⚡ PATHOGENESIS
Key concept: The outcome depends on the immune response
L. donovani enters macrophage
↓
Survives phagolysis by:
- Inhibiting respiratory burst
- Preventing phagolysosome fusion
- Scavenging ROS
↓
┌──────────────────────────┐
↓ ↓
Strong Th1 response Weak/Th2 response
(IL-12, IFN-γ, TNF) (IL-4, IL-10)
↓ ↓
Macrophage activation Impaired killing
Parasite killed Parasite multiplies
ASYMPTOMATIC KALA-AZAR disease
(Positive leishmanin (Negative leishmanin
skin test = immunity) skin test = anergy)
Why pancytopenia?
- Spleen enlarges massively → hypersplenism → destroys all blood cells
- Bone marrow infiltrated by parasites → decreased production
- Autoantibodies form (hypergammaglobulinemia) → hemolysis
🩺 CLINICAL FEATURES
Mnemonic: "SAFE" + dark skin
| S | Splenomegaly (massive, hallmark) |
|---|---|
| A | Anemia, Anorexia |
| F | Fever (prolonged, irregular, biphasic - "Pel-Ebstein-like") |
| E | Emaciation (weight loss) |
| + | Dark skin (hyperpigmentation of face/hands/feet = "Kala-azar" name) |

Massive splenomegaly in a child with Kala-azar (Harrison's 22e)
Lab findings:
- Pancytopenia (leukopenia + anemia + thrombocytopenia)
- Elevated ESR
- Hypoalbuminemia
- Hypergammaglobulinemia (polyclonal IgG rise) → reversal of A:G ratio
- Elevated liver enzymes
Post-Kala-Azar Dermal Leishmaniasis (PKDL):
- Occurs months-years after treatment in India (20-30%) and Sudan (50%)
- Macular/papular/nodular skin lesions (hypopigmented or erythematous)
- Patient remains reservoir for sandfly transmission - important for elimination!
🔬 DIAGNOSIS - Complete Flowchart
SUSPECTED KALA-AZAR
(Fever + Splenomegaly + from endemic area)
↓
┌─────────────────────┐
↓ ↓
SEROLOGICAL PARASITOLOGICAL
(Non-invasive) (Gold Standard)
↓ ↓
rK39 RDT ←─ FIELD Splenic aspirate (>95% sensitivity)
(best for Bone marrow biopsy (60-85%)
field/endemic) Lymph node aspirate (50%)
↓ ↓
ELISA / IFAT ←─ LAB Giemsa stain → LD bodies seen
↓ ↓
└────────► PCR / LAMP (Most sensitive, species ID)
(Gold standard for research/confirmation)
Also: Aldehyde test (Chopra's test) - historical
Formol-gel test - hypergammaglobulinemia proxy
🎯 Key Points on Diagnosis:
| Test | Sensitivity | Notes |
|---|---|---|
| Splenic aspirate | >95% | Gold standard but dangerous if inexperienced |
| Bone marrow biopsy | 60-85% | Safer than splenic |
| rK39 RDT | ~98% | Field test, fingerprick blood, result in 15 min |
| ELISA / IFAT | High | Lab-based antibody detection |
| PCR / LAMP | Highest | Also quantitative, species ID |
| Aldehyde test | Non-specific | Detects hypergammaglobulinemia (not Leishmania-specific) |
Important: Antibody tests stay positive years after cure → cannot use for cure assessment or relapse detection!
Leishmanin skin test (Montenegro test):
- Negative in active kala-azar (patient is anergic = Th2 predominance)
- Becomes positive after successful treatment (immunity restored)
- Used for epidemiological surveys, not active disease diagnosis
💊 TREATMENT
Mnemonic: "LAMB Is My First" (in India)
INDIA (Bihar - antimonial resistant):
First line: Liposomal Amphotericin B (LAMB)
OR Miltefosine (oral, first oral drug for VL!)
OR Conventional AmB deoxycholate
REST OF WORLD:
First line: Pentavalent Antimonials (SbV)
- Sodium stibogluconate (Pentostam): 20 mg/kg/day x 28-30 days
- Meglumine antimoniate (Glucantime): same dose
→ Resistance widespread in Bihar → NOT used there
| Drug | Route | Key Points |
|---|---|---|
| Liposomal AmB (LAMB) | IV | DOC in India, Mediterranean; fewer side effects |
| Miltefosine | Oral | First oral drug; teratogenic - avoid in pregnancy |
| Sodium stibogluconate | IV/IM | DOC in rest of world; QT prolongation risk |
| Pentamidine | IM | 2nd line; now rarely used |
| Paromomycin | IM | Used in combination regimens in India |
Treatment monitoring: Clinical response (fever resolves, spleen shrinks), NOT by antibody tests (remain positive).
🔑 MNEMONICS SUMMARY FOR KALA-AZAR
"BINS" = Bangladesh, India, Nepal, Sudan (90% burden)
"DOT-DASH" = LD body (nucleus=dot, kinetoplast=dash)
"SAFE + dark" = Splenomegaly, Anemia, Fever, Emaciation + dark skin
"LAMB First in India" = Liposomal AmB preferred in Bihar
"Sandfly = Phlebotomus" (P for P for Phlebotomus = Promastigote deposited)
"PKDL = Persistent Kala-azar Dermal Lesion" (source of infection post-treatment)
🪱 MI 3.8 - Filariasis: Wuchereria bancrofti
🧠 CONCEPT FIRST: What Is Filariasis?
Wuchereria bancrofti ek tissue nematode hai jo lymphatic system mein rehta hai aur elephantiasis cause karta hai. "Filar" = thread (worm is thread-like/long). This is a chronic, disabling disease - adult worms lymphatics mein ruk jaate hain aur obstruction cause karte hain.
🦠 THE ORGANISM - Classification
Kingdom: Animalia
Phylum: Nematoda (roundworms)
Class: Secernentea
Order: Spirurida
Family: Onchocercidae
Genus: Wuchereria
Species: bancrofti
KEY FACT: W. bancrofti harbors bacterial endosymbionts
→ WOLBACHIA spp. inside worm
→ Wolbachia is essential for worm's
metabolism, fertility & survival
→ Target for antibiotic therapy (doxycycline)!
📏 MORPHOLOGY
| Adult worm | Microfilaria | |
|---|---|---|
| Size | ♀: 8-10 cm; ♂: 4 cm | 244-296 μm long |
| Location | Lymphatics | Blood (circulating) |
| Sheath | - | Present (sheathed) |
| Nuclear column | - | Nuclei absent from tail tip |
| Diagnostic? | No (hard to find) | Yes (blood smear) |
Sheath importance:
- W. bancrofti sheath: does NOT stain with Giemsa (pale/unstained)
- B. malayi sheath: stains bright pink with Giemsa
- This helps differentiate species in blood smear!
🔄 LIFE CYCLE - COMPLETE FLOWCHART
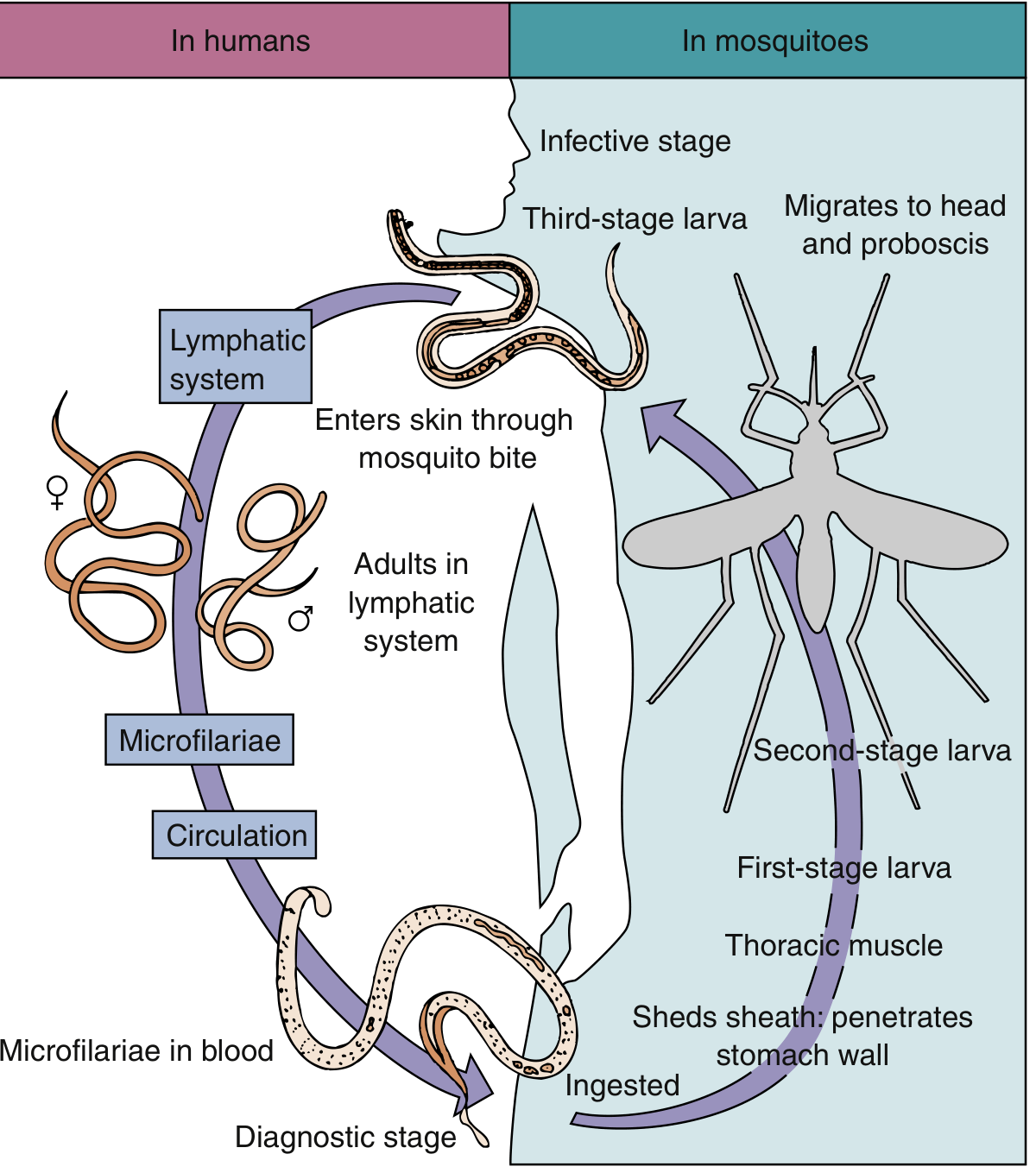
Life cycle of Wuchereria bancrofti (Murray's Medical Microbiology 9e)
═══════════ IN MOSQUITO (Definitive host) ═══════════
Mosquito bites infected human
↓
Ingests MICROFILARIAE (L1 - diagnostic stage for human)
↓
Microfilariae lose sheath → penetrate stomach wall
↓
Migrate to THORACIC MUSCLES → L1 → L2 (sausage stage)
↓
L2 → L3 (infective/filariform larva)
↓
Migrate to HEAD & PROBOSCIS → ready to infect
↓ (mosquito bites next human)
═══════════ IN HUMAN (Intermediate host) ═══════════
L3 larvae deposited near bite wound (NOT injected)
↓
Penetrate skin → enter lymphatics
↓
Migrate to LYMPHATIC VESSELS (arms, legs, groin, scrotum)
↓
L3 → L4 → Adult worms (takes 3-12 months)
↓
♂ fertilizes ♀ → ♀ produces MICROFILARIAE
↓
Microfilariae enter BLOOD CIRCULATION
(NOCTURNAL PERIODICITY - peak at night, 10pm-4am)
↓
Ready to be ingested by next feeding mosquito
🦟 Vectors (Mosquito species):
Mnemonic: "CAn A" mosquito carry filaria?
- C - Culex (most important in India: Culex quinquefasciatus)
- A - Aedes
- A - Anopheles
Key: In India, Culex quinquefasciatus is the principal vector
⏰ NOCTURNAL PERIODICITY - Why Important?
Normal form: Microfilariae in PERIPHERAL blood at NIGHT
(10 PM - 4 AM)
During day → sequestered in PULMONARY capillaries
Why? Synchronized with mosquito biting habits
(Culex bites at night)
Subperiodic form: Pacific islands (Wuchereria bancrofti var. pacifica)
Microfilariae always present (no strict periodicity)
PRACTICAL IMPLICATION:
Blood sample for microfilaria MUST be taken at NIGHT!
💥 PATHOGENESIS & CLINICAL FEATURES
Mnemonic: "LEAF" for stages
L - Latent (asymptomatic microfilaremia)
E - Early/Acute (fever, lymphangitis, lymphadenitis)
A - Advancing (lymph node enlargement, orchitis, hydrocele)
F - Final/Chronic (elephantiasis, chyluria)
Stage 1: ASYMPTOMATIC
- Microfilariae in blood but NO symptoms
- Most common outcome in endemic areas
Stage 2: ACUTE (Lymphangitis/Adenolymphangitis = ADL)
- Fever + chills - recurring attacks
- Lymphangitis (red streaks along lymphatics)
- Lymphadenitis (tender, enlarged lymph nodes)
- Retrograde lymphangitis (from nodes outward) - distinguishes from bacterial
- Orchitis, epididymitis, funiculitis (scrotal involvement common)
- Caused by: inflammatory response to dying adult worms
Stage 3: CHRONIC (Obstructive)
- Lymphedema → Elephantiasis
- Lower limbs (most common), scrotum, vulva, breast, arm
- Skin becomes thick, fissured, warty
- Hydrocele (commonest manifestation overall)
- Chyluria (milky urine - lymph in urine due to lymphatic-urinary fistula)
Stage 4: TROPICAL PULMONARY EOSINOPHILIA (TPE)
Separate syndrome - immunological:
- Hyperimmune response to microfilariae trapped in lungs
- Features: Paroxysmal nocturnal cough + wheeze + high eosinophilia (>3000/μL)
- Antifilarial antibodies very high
- Microfilariae ABSENT from blood (trapped in lung)
- CXR: diffuse miliary shadows or interstitial infiltrates (lower lobes)
- Responds rapidly to DEC → dramatic improvement = supports diagnosis
🔬 DIAGNOSIS - Flowchart
CLINICAL SUSPICION
(Lymphedema/Elephantiasis + endemic area)
↓
┌──────────────────────────────────┐
↓ ↓
DIRECT (Parasitological) INDIRECT
↓ ↓
Night blood smear (10PM-4AM) Serology:
↓ - Antifilarial antibodies
Giemsa stain - Circulating antigen test
→ Microfilariae seen (for W. bancrofti, 96-100% sens)
(sheathed, nuclei don't - NOT for Brugia
reach tail tip)
↓ Eosinophilia (blood count)
Thick smear preferred
↓ Imaging:
Membrane filtration technique - USG of scrotal lymphatics:
(concentration, ↑sensitivity) "filarial dance sign" = live
adult worms moving in dilated
Buffy coat method lymphatics (PATHOGNOMONIC)
↓
PCR / NAAT (most sensitive) DEC provocative test (rarely used)
🎯 Key Diagnostic Points:
| Test | Notes |
|---|---|
| Night blood smear | Simplest, commonest - collect 10PM-4AM |
| Giemsa stain | Sheath present, no nuclei in tail tip |
| Circulating antigen test | Can be done any time (day/night) |
| Filarial dance sign (USG) | Pathognomonic for live adult worms |
| TPE diagnosis | Eosinophilia + nocturnal symptoms + antifilarial Ab + DEC response |
💊 TREATMENT
Mnemonic: "DEC is the KEY"
Drug of Choice: DIETHYLCARBAMAZINE (DEC)
- Kills microfilariae primarily
- Also kills adult worms (partial)
- Dose: 6 mg/kg/day in divided doses x 12 days
- Side effects: Mazzotti reaction (fever, rash, lymphadenitis)
due to dying parasite antigens
COMBINATION THERAPY (Mass Drug Administration - MDA):
DEC + Albendazole (standard MDA)
OR
Ivermectin + Albendazole (where onchocerciasis co-exists)
DOXYCYCLINE:
- Targets WOLBACHIA endosymbiont inside worm
- Kills adult worms (macrofilaricidal)
- 200 mg/day x 6-8 weeks
- Novel approach: "targeting the worm's bacteria"
FOR CHRONIC DISEASE:
- Lymphedema: elevation, elastic bandage, hygiene, physiotherapy
- Hydrocele: surgical correction
- Chyluria: dietary fat restriction, surgery if persistent
- Elephantiasis: irreversible (treatment of little benefit)
🔑 COMPLETE SUMMARY MNEMONICS
FILARIASIS MNEMONICS:
"WBLC" = Wuchereria Bancrofti: Lymphatic; Culex vector
"Night Blood" = take blood sample at NIGHT for microfilaria
"LEAF" = Latent → Early acute → Advanced → Final chronic
"No Nuclei in Tail Tip" = W. bancrofti microfilaria (vs Brugia)
"Sheath" = both W. bancrofti AND B. malayi are sheathed
"DEC is KEY" = Drug of choice
"WOLBACHIA = Target for Doxycycline"
"Filarial Dance Sign" = USG finding = pathognomonic
"TPE = Trapped Pulmonary Eosinophilia" = hyperimmune form
📊 COMPARISON TABLE: W. bancrofti vs B. malayi
| Feature | W. bancrofti | B. malayi |
|---|---|---|
| Distribution | Worldwide (tropics) | South/Southeast Asia |
| Vector | Culex quinquefasciatus | Mansonia species |
| Reservoir | Humans only | Cats, monkeys, humans |
| Microfilaria sheath | Present, does not stain (Giemsa) | Present, stains bright pink |
| Nuclei in tail | None in tail tip | 2 discrete nuclei in tail tip |
| Periodicity | Nocturnal (classic) | Nocturnal/subperiodic |
| Genital involvement | Yes (hydrocele, orchitis) | Rare |
| Elimination possible? | Yes (no animal reservoir) | Harder (animal reservoirs) |
🗂️ INTEGRATED FLOWCHART: Both Topics Side-by-Side
PARASITIC DISEASE
↓
┌──────────────────────┬─────────────────────────┐
│ KALA-AZAR │ FILARIASIS │
│ (L. donovani) │ (W. bancrofti) │
├──────────────────────┼─────────────────────────┤
│ Vector: Sand fly │ Vector: Culex mosquito │
│ (Phlebotomus) │ (quinquefasciatus) │
├──────────────────────┼─────────────────────────┤
│ Site: Macrophages │ Site: Lymphatics │
│ (intracellular) │ (extracellular) │
├──────────────────────┼─────────────────────────┤
│ Diagnostic form: │ Diagnostic form: │
│ LD body (amastigote) │ Microfilaria in blood │
├──────────────────────┼─────────────────────────┤
│ Gold std diagnosis: │ Gold std diagnosis: │
│ Splenic aspirate │ Night blood smear │
│ rK39 RDT (field) │ Circulating Ag test │
├──────────────────────┼─────────────────────────┤
│ DOC in India: │ DOC: │
│ Liposomal AmB / │ DEC (Diethylcarba- │
│ Miltefosine │ mazine) │
├──────────────────────┼─────────────────────────┤
│ Hallmark features: │ Hallmark features: │
│ Huge splenomegaly │ Elephantiasis │
│ Pancytopenia │ Nocturnal microfilaremia │
│ Dark skin │ Hydrocele │
└──────────────────────┴─────────────────────────┘
⭐ EXAM HIGH-YIELD POINTS (Apurba Sastry Style)
Kala-azar:
- LD body = amastigote = "dot-dash" appearance = INTRACELLULAR in macrophage
- Vector = Phlebotomus argentipes in India; only in South Asia = anthroponotic
- Leishmanin test NEGATIVE in active disease, POSITIVE after cure
- rK39 RDT = field gold standard (98% sensitivity outside East Africa)
- PKDL = dangerous because treated patient becomes reservoir again
- DOC in India/Bihar = Liposomal AmB (due to antimonial resistance)
- Miltefosine = ONLY oral drug for VL; teratogenic
Filariasis:
- Blood sample MUST be at night (10PM-4AM) for microfilaria detection
- Sheath present in W. bancrofti + B. malayi (mnemonic: W+B = "WITH" sheath)
- W. bancrofti: NO nuclei reach tail tip (B. malayi: 2 discrete nuclei in tail tip)
- "Filarial dance sign" on USG = pathognomonic = live adult worms
- TPE = trapped microfilariae in lungs = eosinophilia + nocturnal cough + no microfilariae in blood
- Wolbachia inside worm → target for DOXYCYCLINE (macrofilaricidal)
- DEC = DOC for microfilariae; combination with albendazole ± ivermectin in MDA
- India's NDA (National Filariasis Control Programme) uses annual MDA
Sources: Murray's Medical Microbiology 9e, Jawetz Melnick & Adelberg Medical Microbiology 28e, Harrison's Principles of Internal Medicine 22e
This is a shared conversation. Sign in to Orris to start your own chat.