hartmann and paul mikulicz procedure same or different
Reading File
Searching the Web
Hartmann procedure vs Paul Mikulicz procedure differences colostomy
Finding Sources
Finding Sources
Reading Web Page
https://pesquisa.bvsalud.org/portal/resource/pt/emr-176942
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
I now have everything needed for a thorough, well-cited answer. Here is the complete comparison:
Hartmann's Procedure vs. Paul-Mikulicz Procedure - They Are DIFFERENT
Both are two-stage operations for emergency left-sided colonic pathology (obstruction, volvulus, perforation, perforated diverticulitis), but they differ in a critical way - what happens to the distal bowel stump.
Hartmann's Procedure
- The diseased segment (typically sigmoid colon) is resected
- The proximal end is brought out as an end colostomy
- The distal end (rectal stump) is closed and returned to the abdomen as a blind pouch - "Hartmann's pouch"
- The rectum remains inside, shut off
Second stage: Reversal ("Hartmann's reversal") involves re-opening the abdomen and anastomosing the colostomy to the Hartmann's pouch - a more complex re-do operation.
Paul-Mikulicz Procedure (Double-Barrel Colostomy / Exteriorization Resection)
- The diseased segment is resected (or the loop is exteriorized)
- Both the proximal and distal ends are brought out through the abdominal wall as a double-barreled colostomy (side by side, two openings)
- There is no blind intra-abdominal rectal stump
Second stage: Closure is simpler - the two limbs are anastomosed at skin level using a crushing clamp (no need to re-enter the abdomen).
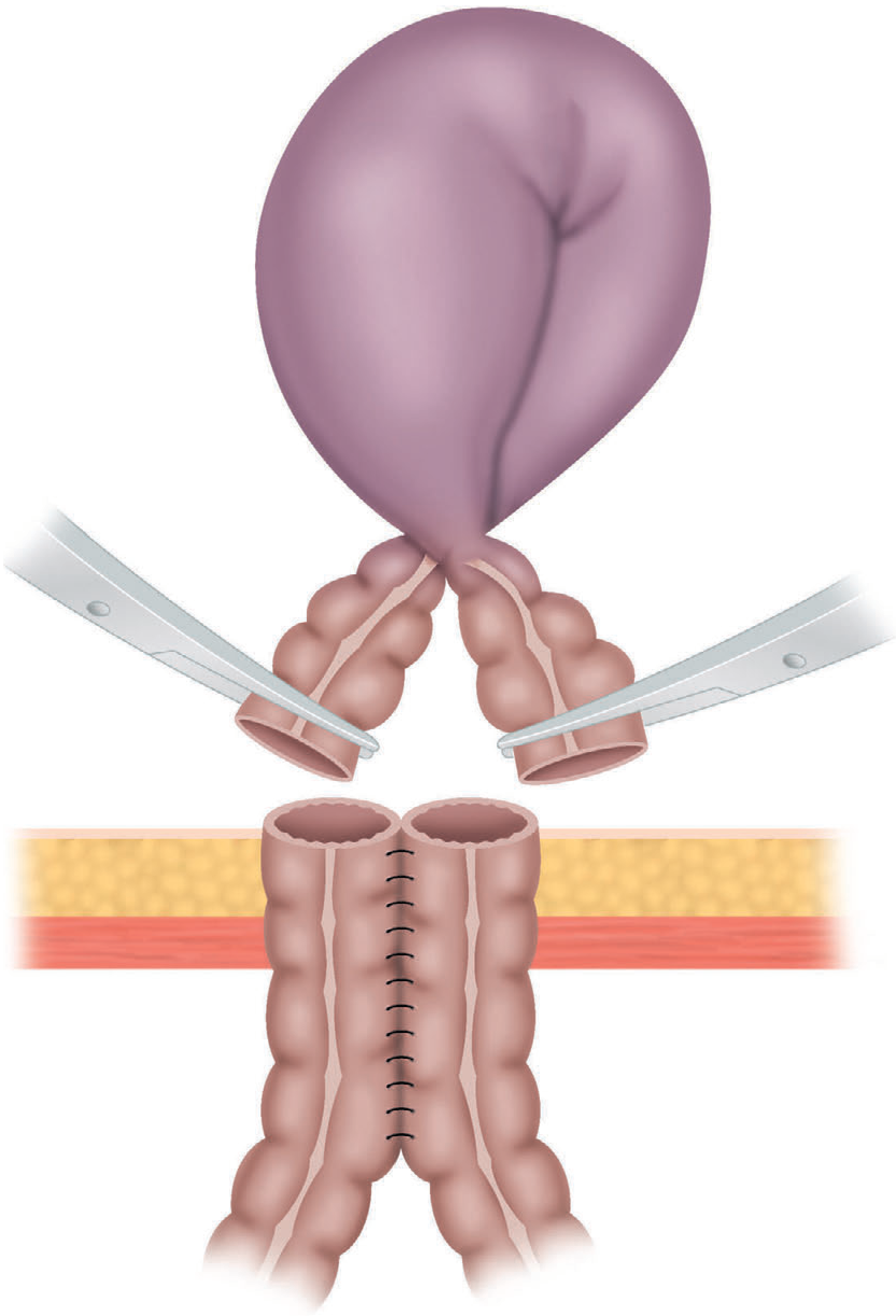
Figure 78.20 from Bailey & Love - The Paul-Mikulicz operation applied to volvulus of the pelvic colon. Note both limbs of bowel being brought out through the abdominal wall as a double-barrel stoma.
Side-by-Side Comparison
| Feature | Hartmann's Procedure | Paul-Mikulicz Procedure |
|---|---|---|
| Diseased segment | Resected | Resected (or exteriorized) |
| Proximal end | End colostomy | One barrel of double colostomy |
| Distal end | Closed, left in abdomen (Hartmann's pouch) | Brought out as second barrel |
| Stoma type | Single-barrel end colostomy | Double-barrel colostomy |
| Reversal complexity | High (re-entry into abdomen, low pelvic dissection) | Lower (anastomosis at abdominal wall level) |
| Preferred when | Distal bowel cannot reach the abdominal wall | Distal bowel can reach the wall |
| Risk of blind stump | Yes (blowout, pelvic sepsis risk) | No |
The Key Practical Distinction (from Bailey & Love's)
"When possible the distal bowel should be brought out at the same time (Paul-Mikulicz procedure) to facilitate subsequent closure. In the majority of cases, the distal bowel will not reach and is closed and returned to the abdomen (Hartmann's procedure)."
- Bailey and Love's Short Practice of Surgery, 28th Ed.
So in practice, Hartmann's is more commonly performed because the distal rectal stump often does not have sufficient reach/mobility to be exteriorized, especially after sigmoid resection. The Paul-Mikulicz is preferred when there is enough distal bowel length, as reversal is technically easier.
Common Indications for Both
- Gangrenous sigmoid volvulus
- Perforated diverticulitis with fecal peritonitis
- Obstructing left-sided colon cancer (emergency)
- Colonic trauma or ischemia
This is a shared conversation. Sign in to Orris to start your own chat.