3 Physiological optics. Physical refraction, clinical refraction (emmetropia, myopia, astigmatism). Research methods. Correction methods. 4 Oral survey. TPCBL. Situational tasks.
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the necessary content. Here is the comprehensive study guide for the topic.
Physiological Optics — Clinical Refraction: Study Guide
1. Physical Optics of the Eye
The Eye as a Refracting System
The eye contains four refracting surfaces: the anterior and posterior surfaces of the cornea, and the anterior and posterior surfaces of the crystalline lens. The total refractive power of the normal eye is approximately +59 diopters (D) when the lens is relaxed.
- Cornea: Provides ~+43 D (the single most powerful refracting surface, due to the large air-to-tissue refractive index difference)
- Crystalline lens: Provides ~+15–20 D (variable via accommodation)
- Aqueous and vitreous humors: Refractive index ≈ 1.336
Diopter (D): Unit of lens power = reciprocal of focal length in meters. A lens with a focal length of 1 m = 1 D; 0.5 m = 2 D.
Snell's Law (Physical Refraction)
When light passes from one medium to another of different density, it bends. The degree of bending follows:
n₁ · sin θ₁ = n₂ · sin θ₂
where n₁, n₂ are refractive indices and θ₁, θ₂ are angles of incidence and refraction.
Accommodation
The lens can change its shape to alter refractive power, allowing focus at varying distances:
- Ciliary muscle contracts → zonular fibers relax → lens becomes thicker and more convex → increased refractive power → near focus
- Controlled by parasympathetic nerves via CN III
- Power of accommodation: ~14 D in children, declining to ~2 D at age 45–50, and ~0 D at 70 (presbyopia)
2. Clinical Refraction: Ametropia
Emmetropia (Normal)
Parallel light rays from a distant object focus exactly on the retina when the ciliary muscle is completely relaxed. The emmetropic eye sees all distant objects clearly without accommodation.
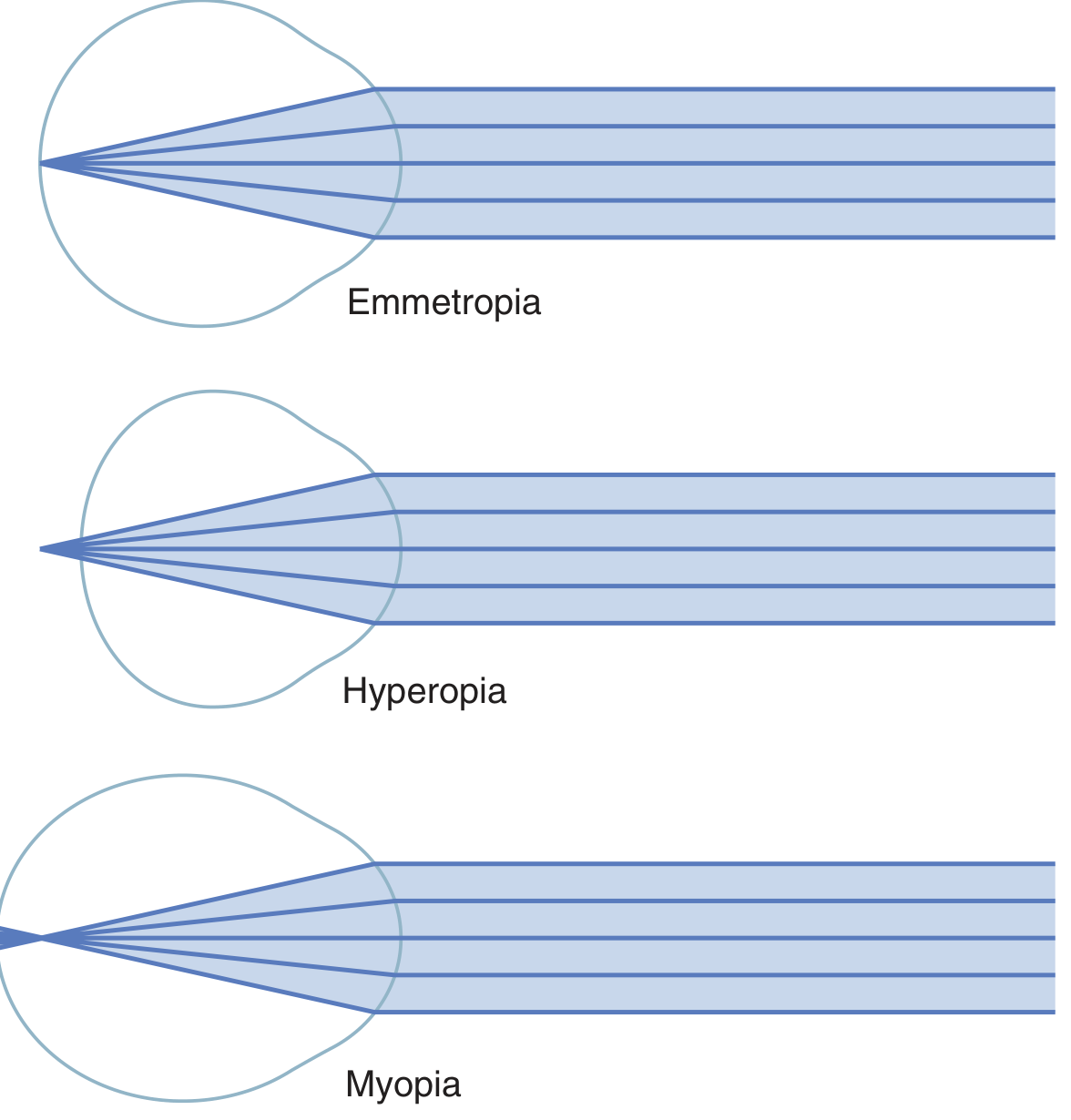
Myopia (Nearsightedness)
| Feature | Detail |
|---|---|
| Cause | Eyeball too long, or lens system too powerful |
| Focus | Parallel light focuses in front of the retina |
| Vision | Distant objects blurred; near objects clear |
| Far point | A definite limiting distance for clear vision |
| Accommodation | Cannot compensate (can't reduce lens power below minimum) |
Hyperopia / Hypermetropia (Farsightedness)
| Feature | Detail |
|---|---|
| Cause | Eyeball too short, or lens system too weak |
| Focus | Parallel light would focus behind the retina |
| Vision | Distant objects may still be seen by using accommodation; near objects require even more effort |
| Accommodation | Partially compensates for distance; fails in presbyopia |
Astigmatism
Definition: Refractive error in which the curvature of the cornea (or less often the lens) differs in two perpendicular meridians, so light rays from a single point focus at two different planes rather than one.
Example: An egg-shaped cornea — the curvature in the vertical plane is greater than in the horizontal plane. Light in the steeper plane focuses closer than light in the flatter plane.
Key property: Accommodation cannot correct astigmatism, because the ciliary muscle increases lens curvature equally in all meridians.
Types by axis:
- Regular astigmatism — principal meridians are perpendicular (with-the-rule, against-the-rule, oblique)
- Irregular astigmatism — no consistent perpendicular relationship (e.g., keratoconus)
3. Research (Examination) Methods
Subjective Refraction
| Method | Principle |
|---|---|
| Trial frame & lens box | "Best vision" found by systematically adding spherical then cylindrical lenses |
| Snellen chart | Standard distance visual acuity (6/6 or 20/20 = normal) |
| Cross-cylinder test | Refines cylinder axis and power |
| Duochrome (bichrome) test | Uses chromatic aberration of the eye to balance under/over-correction |
| Near vision testing (Jaeger chart) | Tests reading vision |
Objective Refraction
| Method | Principle |
|---|---|
| Retinoscopy (skiascopy) | Observe reflex of light from the fundus; neutralize movement with lenses; works under cycloplegia |
| Autorefractometer | Automated infrared optometer; gives objective sphere/cylinder/axis |
| Keratometry (ophthalmometry) | Measures anterior corneal curvature in two meridians; quantifies astigmatism (Javal–Schiötz keratometer) |
| Corneal topography | Placido disc-based mapping of the entire anterior corneal surface; detects keratoconus, irregular astigmatism |
| Corneal pachymetry | Measures corneal thickness; essential pre-refractive surgery |
| Wavefront aberrometry | Maps higher-order aberrations of the entire optical system |
Cycloplegia (cyclopentolate, atropine) paralyzes accommodation — essential for accurate refraction in children and young adults.
4. Correction Methods
4A. Spectacle (Ophthalmic) Lenses
| Error | Lens Type | Mechanism |
|---|---|---|
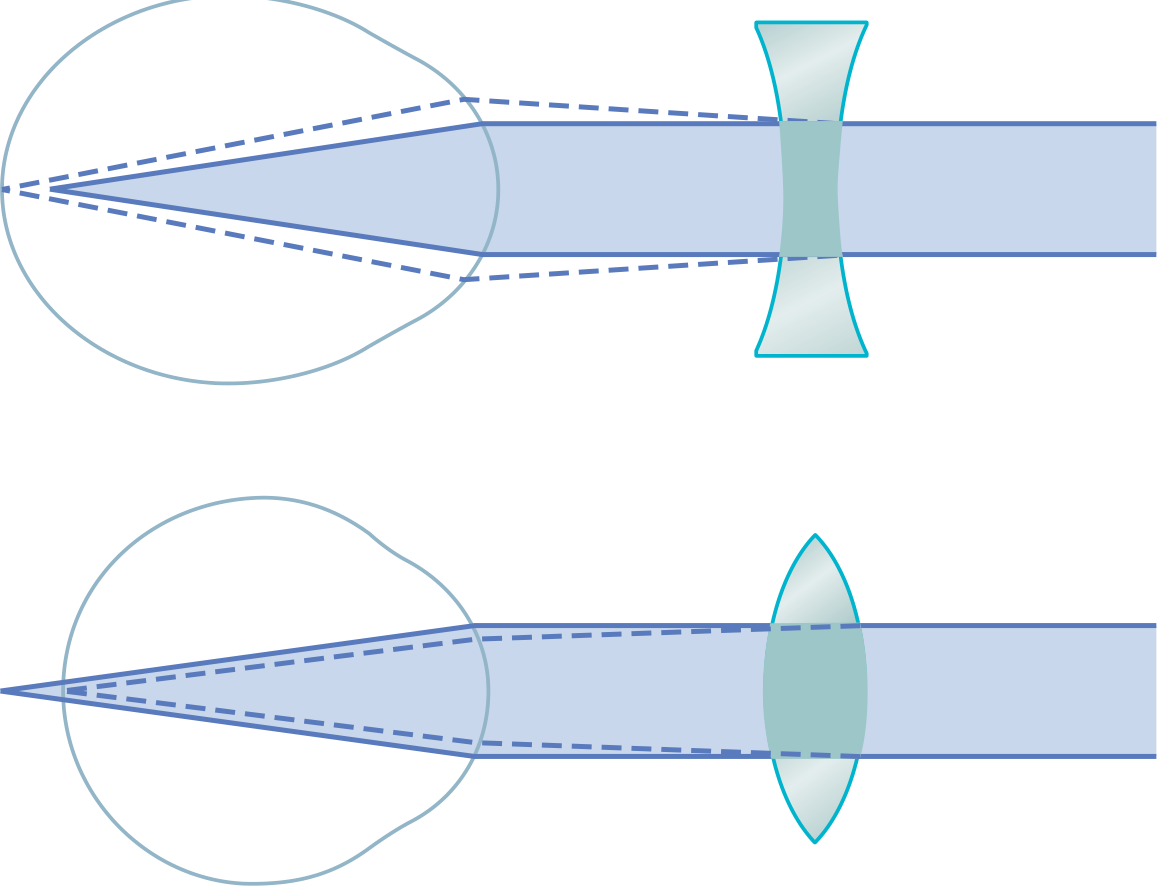
| Myopia | Concave (diverging, –) | Diverges rays so the image moves back to the retina |
| Hyperopia | Convex (converging, +) | Converges rays so the image moves forward to the retina |
| Astigmatism | Cylindrical (combined with spherical) | Corrects one meridian more than the other |
| Presbyopia | Bifocal / trifocal / progressive | Upper segment for distance, lower for reading |
4B. Contact Lenses
- Soft lenses: Flexible hydrogel; drape the cornea; correct sphere and cylinder
- Rigid gas-permeable (RGP): Replace corneal surface; correct irregular astigmatism; tear film fills the gap
- Orthokeratology: Worn overnight; temporarily flatten cornea to reduce myopia
4C. Surgical Correction (Refractive Surgery)
Laser corneal procedures
| Procedure | Full Name | Mechanism | Range |
|---|---|---|---|
| PRK | Photorefractive keratectomy | Surface ablation — removes epithelium, ablates stroma | Myopia ≤ –6 D, astigmatism ≤ 3 D |
| LASEK | Laser epithelial keratomileusis | Preserves epithelial flap | Similar to PRK |
| LASIK | Laser in situ keratomileusis | Corneal flap raised, stroma ablated, flap replaced | Myopia –6 to –8 D, hyperopia ≤ 3–4 D, astigmatism ≤ 5 D |
| SMILE | Small incision lenticule extraction | Femtosecond laser cuts a lenticule; removed through a small incision; no flap | Myopia and myopic astigmatism |
LASIK: Central ablation flattens cornea for myopia; mid-peripheral ablation steepens center for hyperopia. Residual stromal bed must be ≥ 250 μm to prevent ectasia.
Intraocular procedures
| Procedure | Indication | Notes |
|---|---|---|
| Phakic IOL (iris claw / ICL) | High myopia or hyperopia not suitable for laser | Implanted in anterior or posterior chamber; natural lens preserved |
| Clear lens extraction (CLE/RLE) | Very high refractive errors; presbyopia | Replaces natural lens with monofocal, multifocal, toric, or EDOF IOL |
| Toric IOL | Astigmatism correction at time of cataract surgery | Correct axis alignment critical |
| Limbal relaxing incisions (LRI) / arcuate keratotomy | Mild–moderate astigmatism | Paired arcuate incisions flatten the steep corneal meridian |
5. Situational Task Summary (Exam-Ready Points)
- Emmetropia: No refractive error; parallel rays → sharp retinal focus; no lens needed at rest.
- Myopia: Concave (–) lens; LASIK central ablation; "far point" is the limit of clear distant vision.
- Hyperopia: Convex (+) lens; may be latent (masked by accommodation) — reveal with cycloplegia.
- Astigmatism: Cylindrical lens; LASIK/PRK/toric IOL; accommodation cannot correct it.
- Presbyopia: Loss of accommodation (lens elasticity); corrected with bifocals or multifocal IOL.
- Retinoscopy: Gold standard objective method; performed under cycloplegia in children.
- Keratometry: Measures corneal curvature → corneal astigmatism; unit: diopters or mm radius.
- LASIK contraindications: Dry eye, thin cornea (<480 µm), keratoconus, unstable refraction, autoimmune disease, pregnancy.
- SMILE advantage: No flap → no flap complications; better corneal biomechanical stability.
- Phakic IOL: For myopia > –8 D when LASIK is not feasible due to insufficient corneal thickness.
Sources: Guyton & Hall Textbook of Medical Physiology (Ch. 50); Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed. (Ch. 8)
This is a shared conversation. Sign in to Orris to start your own chat.