Poisoning management
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have everything needed to provide a thorough, well-structured answer. Let me compile the comprehensive response.
Poisoning Management
A structured approach to poisoning applies regardless of the specific toxin involved. Management is organized into five core pillars: initial stabilization, toxidrome recognition, decontamination, enhanced elimination, and antidotal therapy.
1. Initial Assessment & Stabilization
ABCs First
- Airway: Intubate early if the patient has depressed consciousness, absent gag reflex, or caustic ingestion. Use rapid-sequence intubation; anticipate difficulty with angioedema (ACE inhibitors, envenomation), caustic burns, or swelling from huffed hydrocarbons. Avoid succinylcholine in organophosphate poisoning (prolonged paralysis) or rhabdomyolysis - use vecuronium or rocuronium instead.
- Breathing: Hypoxemia occurs with CNS depressants (opioids, barbiturates, sedative-hypnotics, clonidine) and neuromuscular blockers (organophosphates, botulinum, tetrodotoxin, elapid envenomation). Respiratory acidosis worsens toxicity of cyclic antidepressants and salicylates - ventilate promptly.
- Circulation: Always check glucose and administer naloxone empirically in altered mental status. Institute ECG monitoring.
Advanced Life Support Modifications
Standard ACLS algorithms must be modified for specific poisons:
| Poison | Standard ACLS Problem | Specific Fix |
|---|---|---|
| Beta-blockers, CCAs, cardiac glycosides | Atropine often ineffective for bradycardia | IV calcium (CCAs), glucagon (beta-blockers/CCAs), digoxin-Fab (glycosides) |
| Beta-blockers, CCAs | Myocardial depression | High-dose insulin-glucose (1 U/kg bolus + infusion) |
| Cocaine, TCAs, class IA/IC antiarrhythmics | Na-channel blockade, wide QRS | IV sodium bicarbonate |
| Cocaine | Tachycardia | Benzodiazepines (NOT beta-blockers - risk of unopposed alpha vasoconstriction) |
| Drug-induced hypertension | Hypertension | Nitroprusside; phentolamine for cocaine alpha-agonism |
- Goldman-Cecil Medicine (International Edition), Chapter 96
2. Toxidrome Recognition
Recognizing the toxidrome focuses treatment even before lab results are available.
| Toxidrome | Key Features | Common Agents |
|---|---|---|
| Adrenergic | Hypertension, hyperthermia, tachycardia, diaphoresis, mydriasis, agitation | Amphetamines, cocaine, caffeine, synthetic cannabinoids |
| Anticholinergic | "Hot, dry, blind, mad, red, full" - hyperthermia, dry flushed skin, mydriasis, urinary retention, delirium, absent bowel sounds | Diphenhydramine, atropine, TCAs, Datura |
| Cholinergic | SLUDGE/DUMBELS - miosis, bradycardia, bronchospasm, diaphoresis, lacrimation, urination, defecation | Organophosphates, carbamates, muscarine mushrooms |
| Opioid | Miosis, respiratory depression, coma - "classic triad" | Heroin, morphine, fentanyl, methadone |
| Sedative-hypnotic | CNS/respiratory depression, ataxia, normal pupils | Benzodiazepines, barbiturates, alcohol |
| Serotonin syndrome | Hyperthermia, clonus, agitation, diaphoresis, diarrhea | SSRIs, MAOIs, tramadol, linezolid combinations |
3. Decontamination
The algorithm below (from Goldman-Cecil Medicine) guides decontamination decisions:
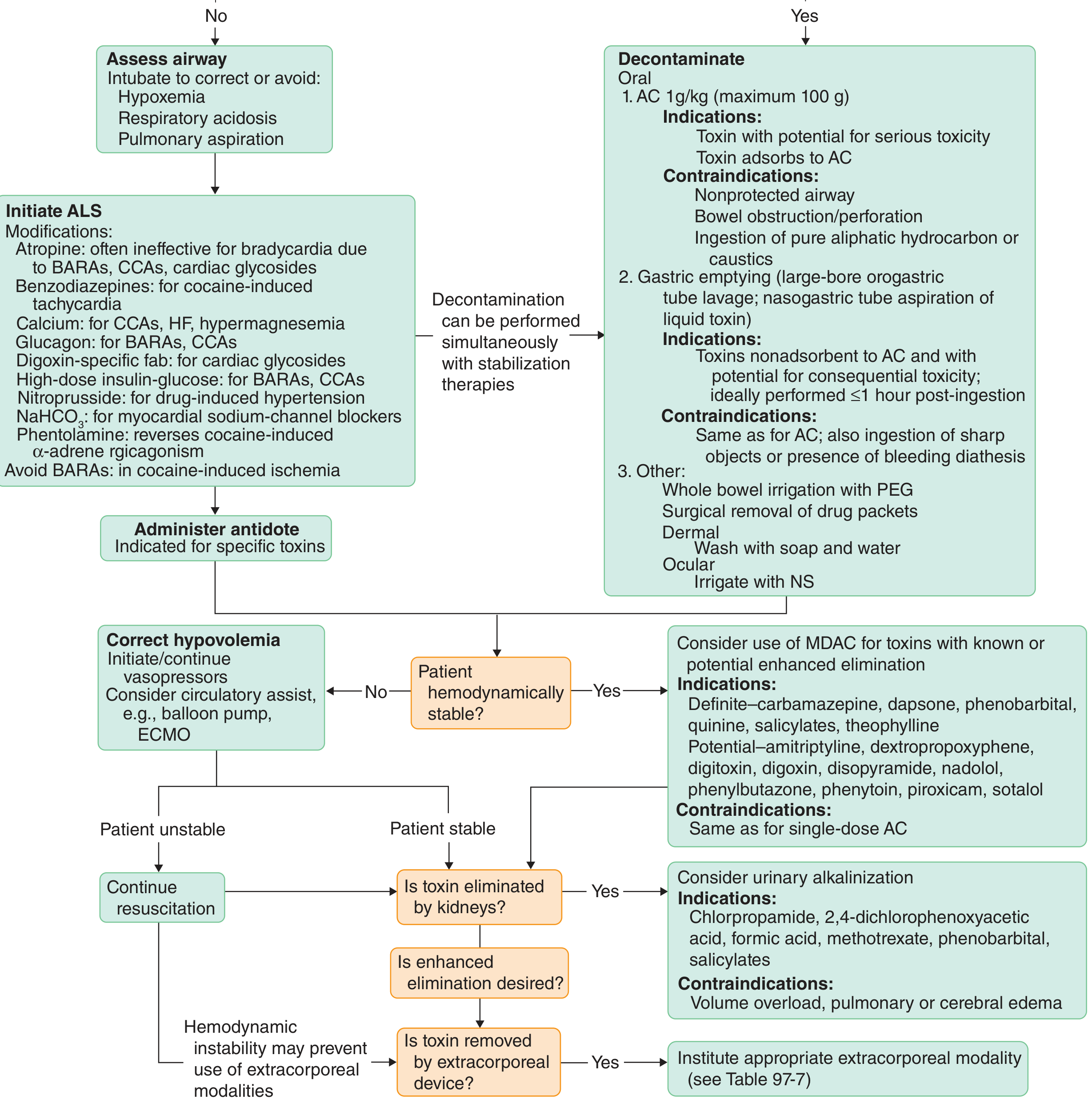
GI Decontamination (for ingestions)
Activated Charcoal (AC)
- Dose: 1 g/kg orally (max 100 g)
- Best within 1 hour of ingestion
- Indications: toxin with serious potential AND adsorbs to AC
- Contraindications: unprotected airway, bowel obstruction/perforation, pure aliphatic hydrocarbons or caustics
- Does NOT adsorb: LIMAL - Lead/heavy metals, Iron, Methanol/alcohols, Alkalis (lithium, potassium)
Gastric Lavage
- Large-bore orogastric tube; ideally within 1 hour of ingestion
- Reserved for toxins non-adsorbent to AC with serious toxicity potential
- Routine gastric lavage is NOT recommended; risks include aspiration, perforation
- Added contraindications: sharp object ingestion, bleeding diathesis
Whole Bowel Irrigation (WBI)
- Polyethylene glycol electrolyte solution (PEG)
- Used for: body packers ("drug mules"), sustained-release preparations, iron, lithium (substances not bound by AC)
Induced emesis (syrup of ipecac): NOT recommended in current practice
Dermal/Ocular decontamination
- Skin: wash with soap and water
- Eyes: irrigate with normal saline to neutral pH
- Lippincott Illustrated Reviews: Pharmacology, p. 1521
- Tintinalli's Emergency Medicine, Chapter 195
4. Enhanced Elimination
Once the patient is stabilized, consider whether enhanced elimination is appropriate.
Multiple-Dose Activated Charcoal (MDAC)
Works by interrupting enterohepatic recirculation and creating a gut-to-blood concentration gradient ("gut dialysis").
- Definite benefit: carbamazepine, dapsone, phenobarbital, quinine, salicylates, theophylline
- Potential benefit: digitoxin, digoxin, phenytoin, piroxicam, sotalol, amitriptyline
- Requirement: bowel sounds must be present before each dose (risk of obstruction)
Urinary Alkalinization
- IV sodium bicarbonate to achieve urine pH 7.5-8 (serum pH must not exceed 7.55)
- Traps acidic drugs in ionized form in urine, preventing tubular reabsorption
- Indications: salicylates, phenobarbital, chlorpropamide, methotrexate, formic acid, 2,4-D
- Contraindications: volume overload, pulmonary or cerebral edema
Hemodialysis
Effective when the toxin has: low protein binding + small volume of distribution + small molecular weight + water solubility
- Dialyzable substances: methanol, ethylene glycol, salicylates, theophylline, phenobarbital, lithium
- Ethylene glycol/methanol: fomepizole (or ethanol) blocks metabolism; hemodialysis removes the toxic alcohol
Other Extracorporeal Methods
- Hemoperfusion, CRRT, ECMO (for refractory cardiovascular failure)
- Lippincott Illustrated Reviews: Pharmacology, p. 1521-1522
5. Antidotal Therapy
| Toxin/Poison | Antidote | Key Notes |
|---|---|---|
| Acetaminophen | N-Acetylcysteine (NAC) | IV preferred; most effective within 8 hrs; continue if AST elevated |
| Opioids | Naloxone | 0.4-2 mg IV/IN; repeat dosing or infusion for long-acting opioids; titrate to respiratory rate only |
| Benzodiazepines | Flumazenil | Caution: may precipitate seizures in mixed overdose/chronic users |
| Organophosphates/Carbamates | Atropine + Pralidoxime (2-PAM) | Atropine: large doses to dry secretions; 2-PAM reactivates cholinesterase (within hours) |
| Digoxin/cardiac glycosides | Digoxin-specific Fab antibodies | Reverses bradycardia and dysrhythmias |
| Beta-blockers | Glucagon + High-dose insulin | Glucagon: 3-5 mg IV bolus, then infusion; HDI: 1 U/kg bolus + infusion |
| Calcium-channel blockers | IV Calcium + High-dose insulin | Calcium chloride 1g IV; HDI insulin-glucose |
| Cyanide | Hydroxocobalamin (or Na nitrite + Na thiosulfate) | Hydroxocobalamin preferred in fire smoke inhalation |
| Methanol/Ethylene glycol | Fomepizole (or ethanol) | Inhibits alcohol dehydrogenase; prevents formation of toxic metabolites |
| Methemoglobinemia | Methylene blue | 1-2 mg/kg IV over 5 min; max 7 mg/kg; avoid in G6PD deficiency |
| Heparin | Protamine sulfate | 1 mg per 100 units heparin |
| Warfarin | Vitamin K + FFP/4-factor PCC | Vitamin K reverses over hours-days; PCC/FFP for immediate reversal |
| Iron | Deferoxamine | IV infusion in severe toxicity |
| Lead | DMSA (succimer) or EDTA | Oral DMSA first-line in children |
| TCA overdose | IV Sodium bicarbonate | Reverses Na-channel blockade, narrow QRS |
| Salicylates | Sodium bicarbonate (urine alkalinization) + HD | No specific antidote; supportive care |
| Local anesthetic toxicity | Intralipid (20% lipid emulsion) | 1.5 mL/kg bolus, then infusion; "lipid sink" mechanism |
- Goldman-Cecil Medicine (International Edition), Table 96-6
6. General Supportive Measures
- Seizures: benzodiazepines first-line (diazepam/lorazepam)
- Hyperthermia: aggressive external cooling; benzodiazepines for agitation (especially sympathomimetics/serotonin syndrome)
- Rhabdomyolysis: aggressive IV fluids, monitor CK, urine output, renal function
- Dysrhythmias: correct electrolytes, consider toxin-specific therapy before antiarrhythmics
- Hypotension: IV crystalloids first; vasopressors if refractory; avoid epinephrine in cocaine toxicity
- Psychiatric assessment: all intentional overdoses require mental health evaluation before discharge
- Poison Control Center: consult early (in the US: 1-800-222-1222)
Quick Reference: "DONT" Empiric Regimen for Altered Mental Status
- Dextrose (50 mL of 50% D50W IV) - rule out hypoglycemia
- Oxygen - pulse oximetry, supplemental O2
- Naloxone 0.4-2 mg IV - for opioid toxicity
- Thiamine 100 mg IV - before glucose in alcoholic/malnourished patients (Wernicke's prevention)
Sources: Goldman-Cecil Medicine, International Edition (Chapter 96); Lippincott Illustrated Reviews: Pharmacology (Chapter 46); Tintinalli's Emergency Medicine, A Comprehensive Study; Brenner & Rector's The Kidney
This is a shared conversation. Sign in to Orris to start your own chat.