Internal capsule
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
Finding Sources
I now have comprehensive, well-illustrated content. Let me compile the full answer.
The Internal Capsule
Definition and Overview
The internal capsule is a compact lamina of white matter - the largest projection fiber tract in the brain - containing both afferent and efferent nerve fibers passing to and from the cerebral hemispheres and the brainstem. It continues rostrally with the corona radiata and caudally with the cerebral peduncles (basis pedunculi). - Localization in Clinical Neurology, 8e, p. 31
Anatomy and Relations
On a horizontal (axial) section, the internal capsule forms a V- or chevron-shape (like two letter Vs with points facing inward). A simple rule applies to all adjacent structures:
- Always medial to the internal capsule: caudate nucleus, thalamus
- Always lateral to the internal capsule: lentiform nucleus (putamen + globus pallidus)
From lateral to medial, structures encountered in sequence are: insula → extreme capsule → claustrum → external capsule → putamen → external medullary lamina → external globus pallidus → internal medullary lamina → internal globus pallidus → internal capsule. - Neuroanatomy through Clinical Cases 3rd Ed., p. 16
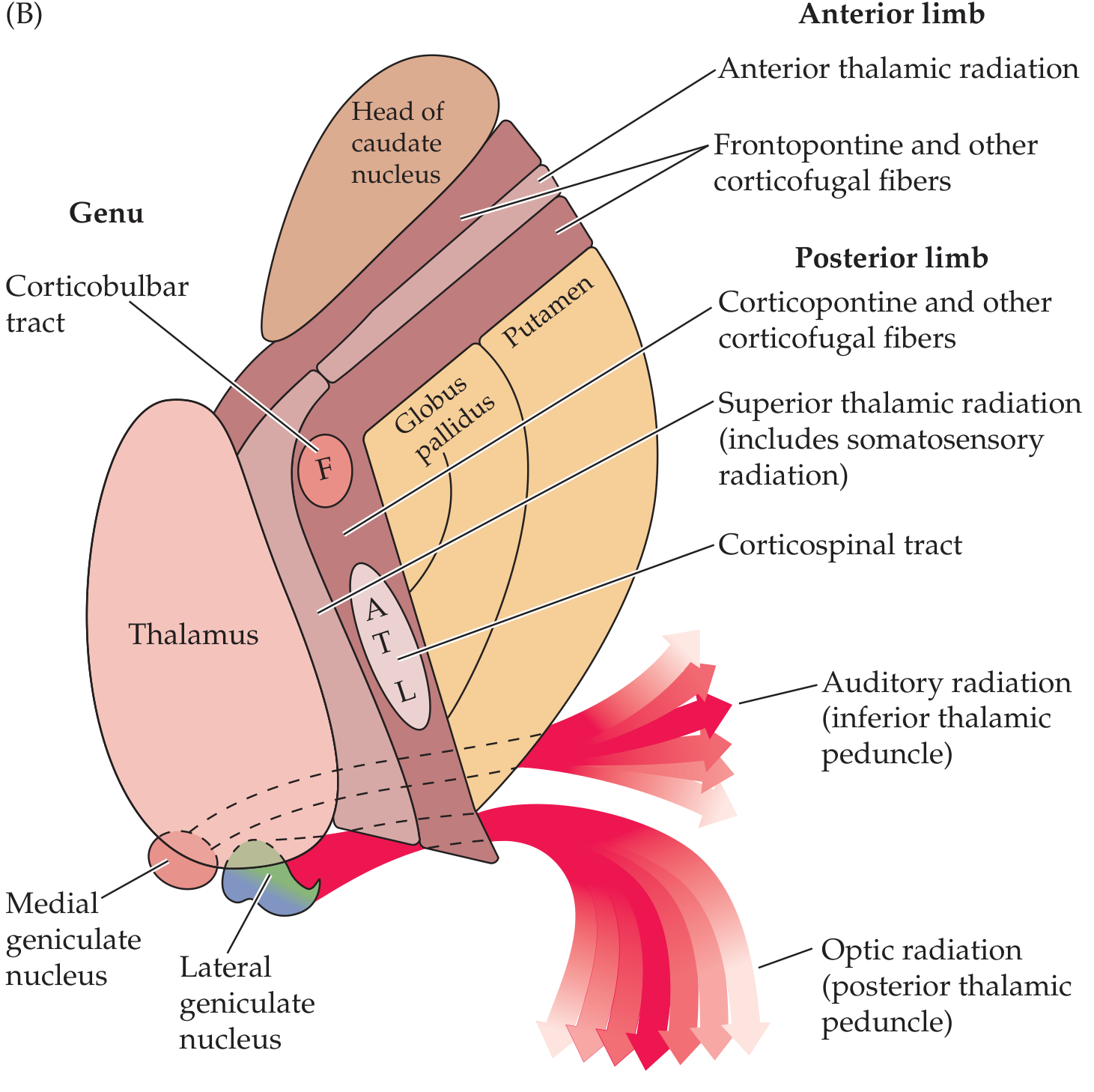
Five Segments
| Segment | Location | ~Length | Key Fiber Tracts |
|---|---|---|---|
| Anterior limb | Between head of caudate (medial) and lentiform nucleus (lateral) | ~2 cm | Frontopontine fibers; anterior thalamic radiation; corticothalamic/thalamocortical fibers (frontal lobe - thalamus); caudate-putaminal fibers |
| Genu | At the "knee" (transition between anterior and posterior limbs), at the level of the foramen of Monro | - | Corticobulbar tract (to brainstem motor nuclei); corticoreticular fibers (descend to bilateral reticular formation); motor corticopontine fibers |
| Posterior limb | Between lentiform nucleus (lateral) and thalamus (medial) | ~3-4 cm | Corticospinal tract (somatotopically arranged - face most anterior, then arm, trunk, leg most posterior); superior thalamic radiation (somatosensory); corticothalamic/thalamocortical fibers; corticorubral fibers |
| Retrolenticular segment | Behind the lentiform nucleus | - | Optic (visual) radiations (geniculocalcarine tract / radiation of Gratiolet); corticotectal, corticonigral, corticotegmental fibers |
| Sublenticular segment | Below the lentiform nucleus | - | Auditory radiations (inferior thalamic peduncle); temporopontine fibers |
- Localization in Clinical Neurology, 8e, pp. 31-32
Somatotopic Organization in the Posterior Limb
The corticospinal fibers within the posterior limb are somatotopically arranged, with fibers to the upper extremity more anterior and fibers to the lower extremity, bladder, and rectum more posterior (shoulder → elbow → wrist → fingers → trunk → hip → knee → ankle → toes). As the tract descends, its fibers intermix with corticoreticular, corticopontine, and corticocortical fibers. - Localization in Clinical Neurology, 8e, p. 31
Because all these fibers are densely packed, a single small capsular lesion can produce complete contralateral hemiparesis (face + arm + leg). Occasionally, more selective deficits occur. - Neuroanatomy through Clinical Cases 3rd Ed., p. 258
Blood Supply
| Segment | Artery | Source |
|---|---|---|
| Anterior limb | Recurrent artery of Heubner | Anterior cerebral artery (ACA) |
| Genu + middle and inferior posterior limb | Anterior choroidal artery | Internal carotid artery |
| Superior anterior and posterior limb | Lenticulostriate arteries | Middle cerebral artery (MCA) |
These are all deep perforating end-arteries, which explains why the internal capsule is so prone to lacunar infarcts and hypertensive hemorrhages. - Localization in Clinical Neurology, 8e, p. 32
Clinical Syndromes
1. Pure Motor Hemiparesis (PMH)
The most classic capsular syndrome. A small lacunar infarct or demyelinating lesion in the posterior limb interrupts the densely packed corticobulbar + corticospinal fibers, producing contralateral weakness of the face, arm, and leg without sensory loss, visual changes, or cortical signs. Common causes: lacunar infarct (hypertension, small vessel disease), demyelination, small hemorrhage. - Neuroanatomy through Clinical Cases 3rd Ed., p. 730
2. Capsular Genu Syndrome
Lesion at the genu affecting corticobulbar fibers - produces predominantly facial and lingual hemiparesis with mild limb involvement. - Localization in Clinical Neurology, 8e, p. 31
3. Lateral/Posterior Internal Capsule Syndrome (Anterior Choroidal Artery territory)
From Bradley & Daroff's Neurology in Clinical Practice:
- Contralateral hemiparesis
- Contralateral diminished pain and temperature
- Dysarthria
- Homonymous hemianopia (usually with a tongue of sparing along the horizontal meridian)
- Memory impairment
- Visuoperceptual abnormalities (with right-sided lesions)
4. Internal Capsular Hemorrhage
- 60% of all intracerebral hemorrhages occur in the internal capsule (the small perforating arteries are especially prone to rupture in hypertension). The next most common sites are cerebral cortex, pons, thalamus, and cerebellum (10% each). - Ganong's Review of Medical Physiology, 26th Ed., p. 250
- Decorticate rigidity (flexion posturing on the hemiplegic side) is the classic sign.
- Small hemorrhages in the genu or posterior limb may cause PMH or a mixed sensorimotor syndrome.
- Bilateral posterior-limb hemorrhages rarely produce paraparesis. - Localization in Clinical Neurology, 8e, p. 1395
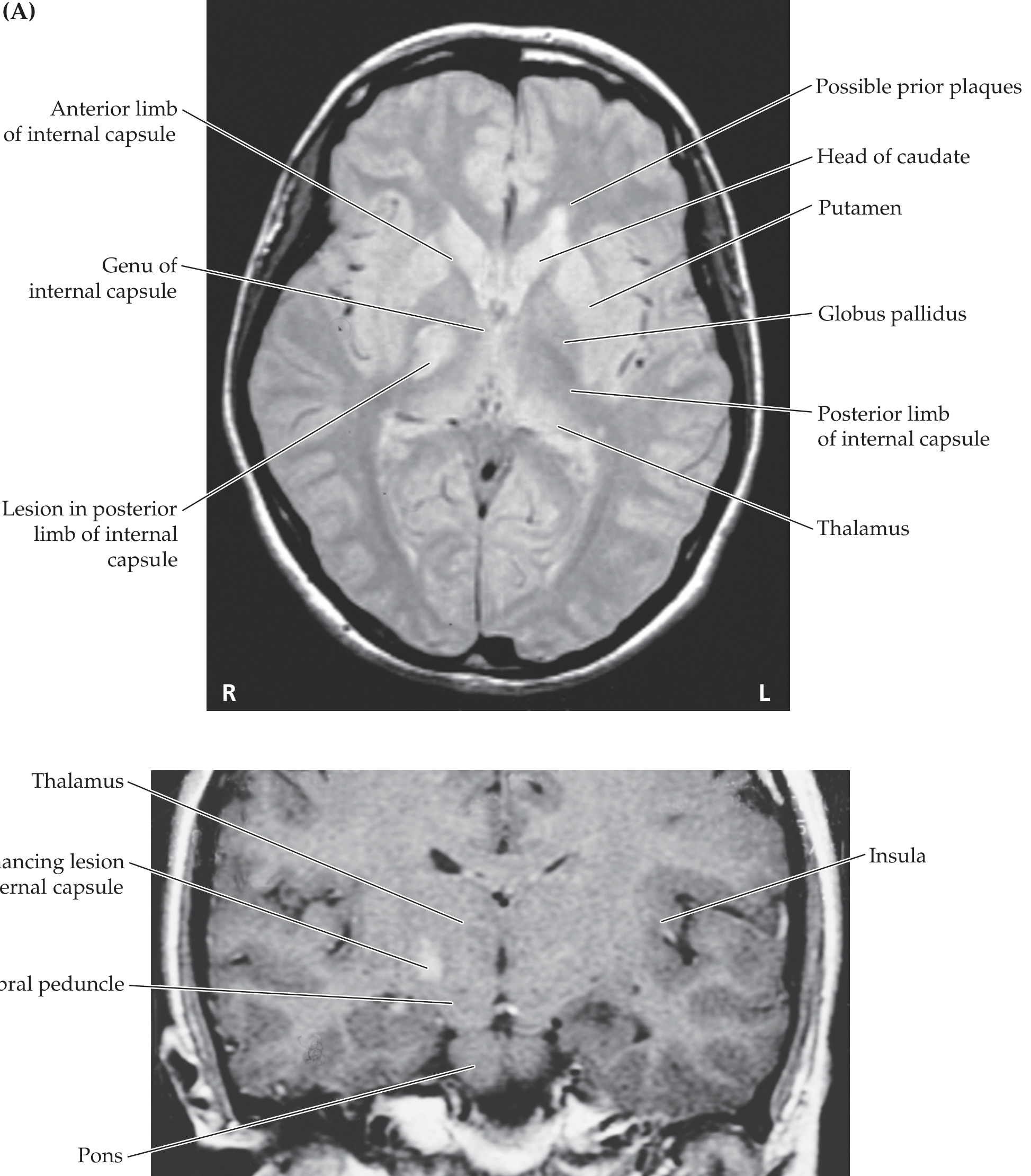
MRI Appearance - Lesion in the Posterior Limb
The axial MRI below shows a lesion (hyperintense) in the posterior limb of the right internal capsule causing pure motor hemiparesis, with normal contralateral side for comparison:
Key Points Summary
| Feature | Detail |
|---|---|
| Nature | Compact white matter (largest projection fiber system) |
| Shape on axial section | V-shaped / chevron |
| Medial structures | Caudate nucleus + thalamus |
| Lateral structures | Lentiform nucleus (putamen + globus pallidus) |
| Segments | 5: anterior limb, genu, posterior limb, retrolenticular, sublenticular |
| Key tract per segment | Anterior limb = frontopontine; Genu = corticobulbar; Posterior limb = corticospinal + somatosensory; Retrolenticular = optic radiation; Sublenticular = auditory radiation |
| Continues rostrally | Corona radiata |
| Continues caudally | Cerebral peduncles |
| Most important clinical site | Posterior limb - dense packing makes small lesions devastating |
| Most common pathology | Hypertensive lacunar infarct or hemorrhage |
| Classic syndrome | Pure motor hemiparesis (contralateral face + arm + leg weakness, no sensory loss) |
This is a shared conversation. Sign in to Orris to start your own chat.