Screening and diagnosis of hypoxia in fetus during intrauterine period
Reading File
Finding Sources
Finding Sources
Searching PubMed
"fetal hypoxia" AND "intrauterine" AND diagnosis
Finding Sources
Finding Sources
Searching PubMed
"fetal surveillance" AND "hypoxia" AND "intrauterine"
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Searching PubMed
"fetal growth restriction" AND "Doppler" AND surveillance
Reading File
I now have comprehensive content. Let me compile the full answer.
Screening and Diagnosis of Intrauterine Fetal Hypoxia
Intrauterine fetal hypoxia refers to inadequate oxygen delivery to the fetus during the antenatal period. Because no single test satisfies all clinical requirements, a multi-modal approach is used that integrates maternal history, fetal behavioral assessment, biophysical surveillance, and Doppler hemodynamic studies.
1. Pathophysiologic Basis
Fetal oxygenation depends on:
- Adequate uteroplacental blood flow
- Intact fetoplacental gas exchange
- Normal fetal cardiovascular adaptation
When placental insufficiency develops, fetal responses occur in a predictable sequence:
- Redistribution of blood flow — "brain-sparing" centralization (increased cerebral and cardiac flow, decreased renal/peripheral flow)
- Oligohydramnios — reduced renal perfusion → decreased urinary output → reduced amniotic fluid
- Cardiac decompensation — rising venous pressures, abnormal ductus venosus waveform
- Acidemia and end-organ failure
The fetal heart rate (FHR) is increasingly dominated by the parasympathetic system as gestation advances, producing a gradual decrease in baseline rate, increased variability, and responsiveness to acute changes. The ability to accelerate the FHR in response to movement is directly related to fetal oxygenation — this is the physiologic basis of the nonstress test.
2. Indications for Fetal Surveillance (When to Screen)
Antepartum fetal surveillance is indicated when the risk of intrauterine fetal compromise is elevated:
| Category | Examples |
|---|---|
| Maternal conditions | Hypertension, diabetes, CKD, autoimmune disease, severe anemia, cardiac disease |
| Placental/uterine | Preeclampsia, placental insufficiency, prior stillbirth |
| Fetal conditions | Suspected FGR (<10th percentile), multiple gestation, Rh isoimmunization |
| Pregnancy complications | Oligohydramnios, polyhydramnios, decreased fetal movement, post-term pregnancy |
ACOG guidance includes single umbilical artery, oligohydramnios, and placental abruption among indications for outpatient antenatal surveillance.
3. Screening and Diagnostic Methods
3.1 Maternal Perception of Fetal Movement (Kick Counting)
The simplest and most accessible method. Decreased fetal movement may be an early sign of fetal compromise. Various counting protocols exist (e.g., Cardiff count-to-ten). It serves as a trigger for further evaluation but lacks adequate specificity or sensitivity alone.
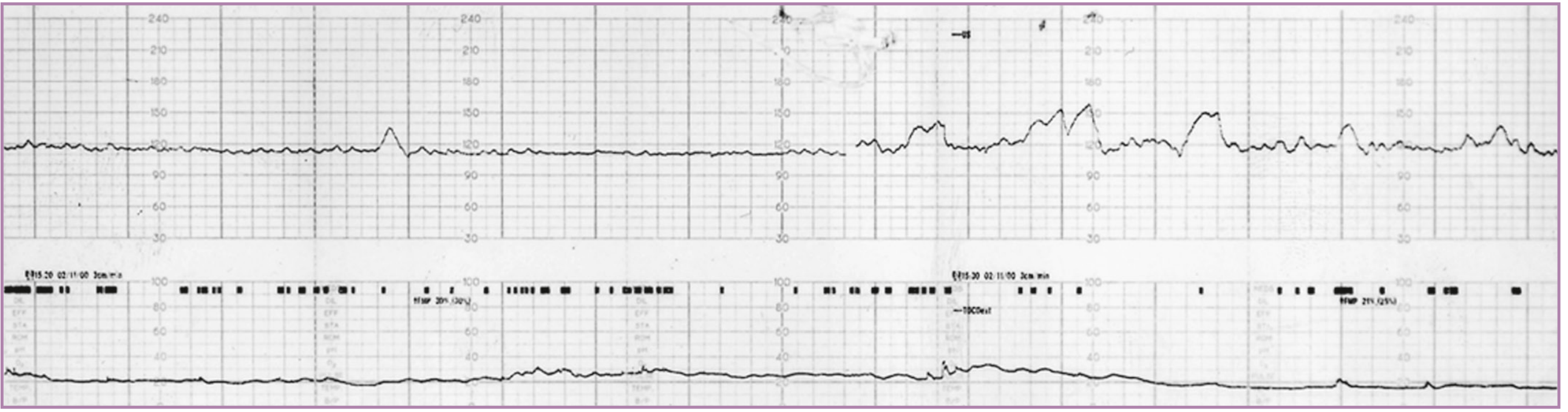
3.2 Non-Stress Test (NST)
Principle: FHR accelerations in response to fetal movement indicate intact neurologic control and adequate oxygenation.
Reactive (normal) NST:
- ≥2 FHR accelerations within a 20–30 minute window
- Accelerations are graded by gestational age (e.g., ≥15 bpm for ≥15 sec at ≥32 weeks; ≥10 bpm for ≥10 sec at <32 weeks)
- Also requires moderate baseline variability
Non-reactive NST: Absence of qualifying accelerations. About 10–12% of fetuses in the third trimester do not meet criteria at 30 minutes, but this falls to <6% by 40 minutes. The most common cause of a non-reactive NST is a fetal sleep cycle rather than true compromise.
Performance:
- False-negative rate (fetal death within 1 week of reactive NST): ~1.9 per 1,000 in the largest studies
- The NST is best used as a first-line test, with additional assessment added to improve sensitivity
Vibroacoustic Stimulation (VAS): An electromechanical device producing broad-band noise can convert a non-reactive NST to a reactive one by inducing a fetal state change, thereby reducing testing time and false-positive rates.
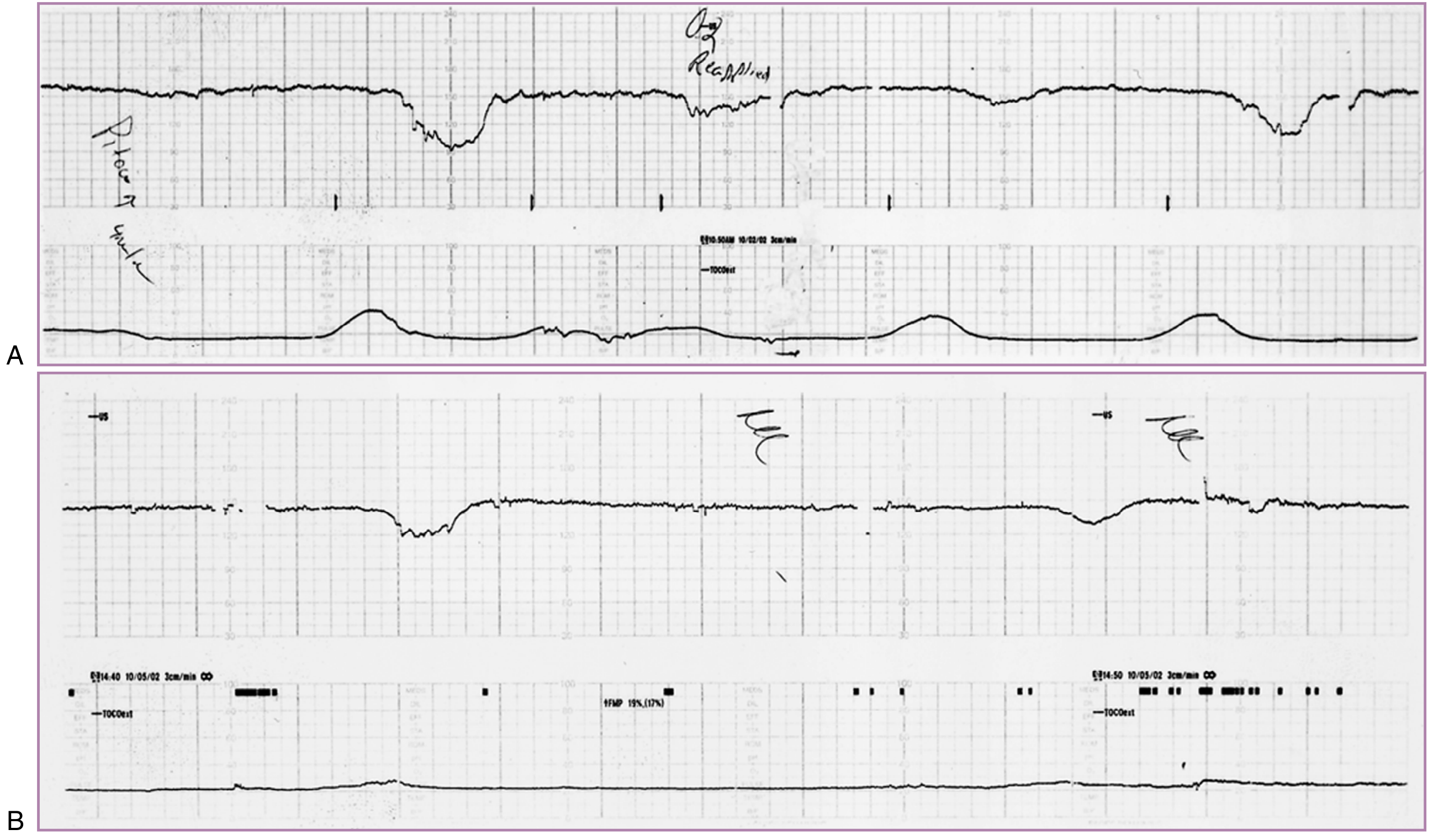
3.3 Contraction Stress Test (CST) / Oxytocin Challenge Test (OCT)
Principle: Uterine contractions temporarily reduce uteroplacental blood flow. A hypoxic fetus cannot tolerate this and exhibits late decelerations.
- Positive CST (abnormal): Persistent late decelerations with most contractions — indicates uteroplacental insufficiency
- Negative CST (normal): No late decelerations with ≥3 contractions in 10 minutes
- Requires ≥3 contractions/10 min; achieved by nipple stimulation or IV oxytocin
The CST was first introduced in the 1970s after the observation that recurrent late decelerations were associated with fetal hypoxemia. It is more sensitive but more labor-intensive than the NST.
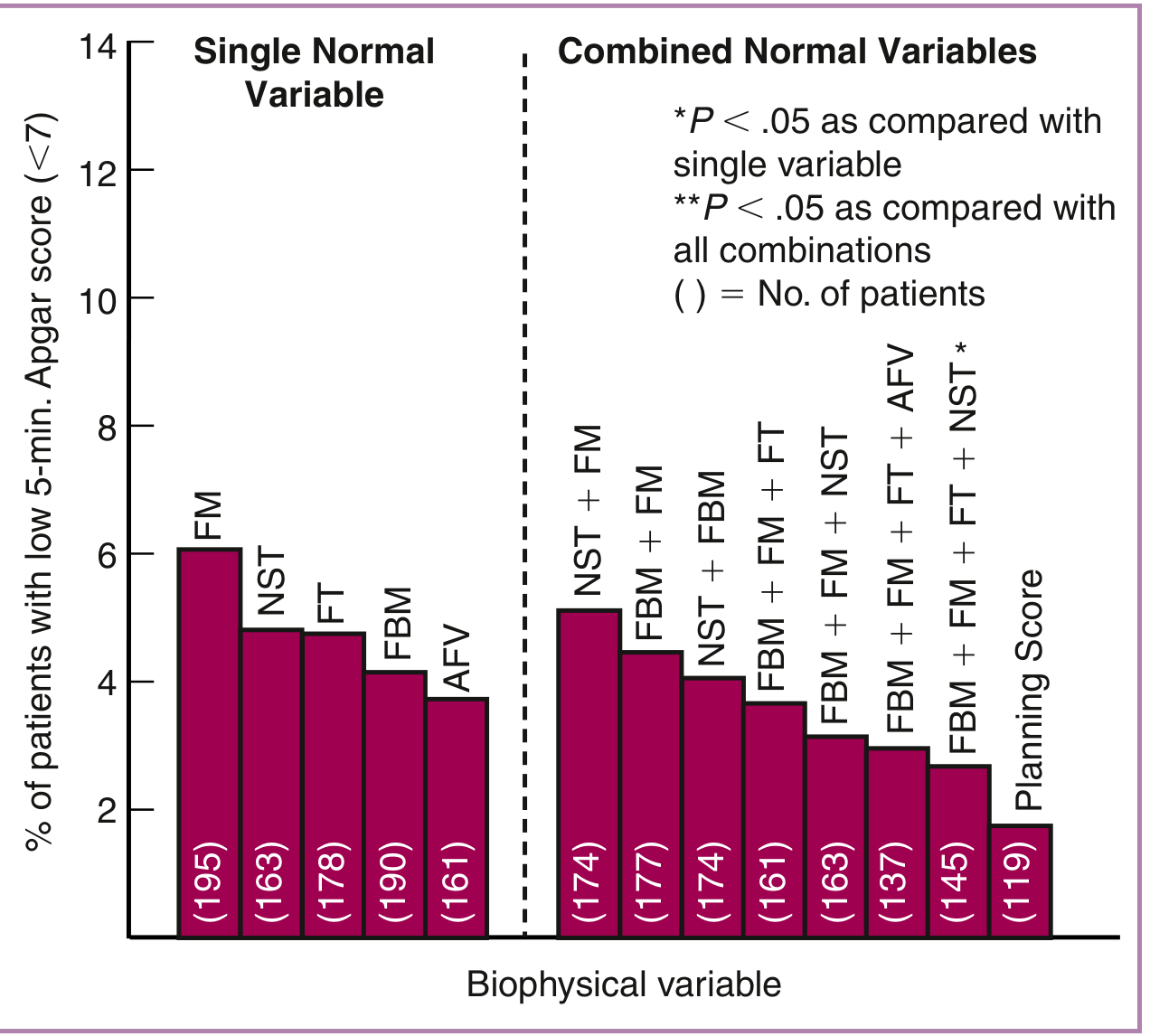
3.4 Biophysical Profile (BPP)
The BPP combines real-time ultrasound assessment with the NST to evaluate five fetal parameters, each scored 0 or 2 (maximum 10):
| Variable | Normal (Score = 2) | Abnormal (Score = 0) |
|---|---|---|
| Fetal breathing movements (FBM) | ≥1 episode of sustained FBM >30 s within 30 min | Absent or no sustained episodes |
| Gross body/limb movements | ≥3 discrete movements in 30 min | <3 movements |
| Fetal tone | Active extension with rapid return to flexion; brisk repositioning | Low-velocity movement only; incomplete flexion; flaccid extremities |
| Nonstress test (NST) | Moderate variability; accelerations coupled with FMs | Decelerative trace; absent or insufficient accelerations |
| Amniotic fluid volume (AFV) | ≥1 cord-free pocket >2 cm | No cord-free pocket >2 cm, or subjectively reduced fluid |
Interpretation:
- BPP ≥8/10: Normal — low risk of fetal asphyxia
- BPP 6/10: Equivocal — repeat within 24 hours or deliver if at term
- BPP ≤4/10: Abnormal — strong consideration for delivery
Performance: In a study of 19,221 high-risk pregnancies, the fetal death rate after a normal BPP (≥8) was 0.726 per 1,000 births; in FGR pregnancies specifically, only 4 fetal deaths occurred after a normal test (false-negative rate <1 per 1,000).
Modified BPP: NST + amniotic fluid index (AFI). This is widely used in practice as a simpler, faster screen.
3.5 Amniotic Fluid Assessment
Oligohydramnios reflects chronic fetal hypoxia causing blood flow redistribution away from kidneys → reduced urinary output. It is an important marker of chronic placental insufficiency.
- AFI <5 cm or single vertical pocket (SVP) <2 cm = oligohydramnios
- SVP correlates more closely with outcome and causes less unnecessary induction compared to AFI
- Severe oligohydramnios: AFI <5 cm was present in 89% of intrauterine demises in early-onset FGR in one study
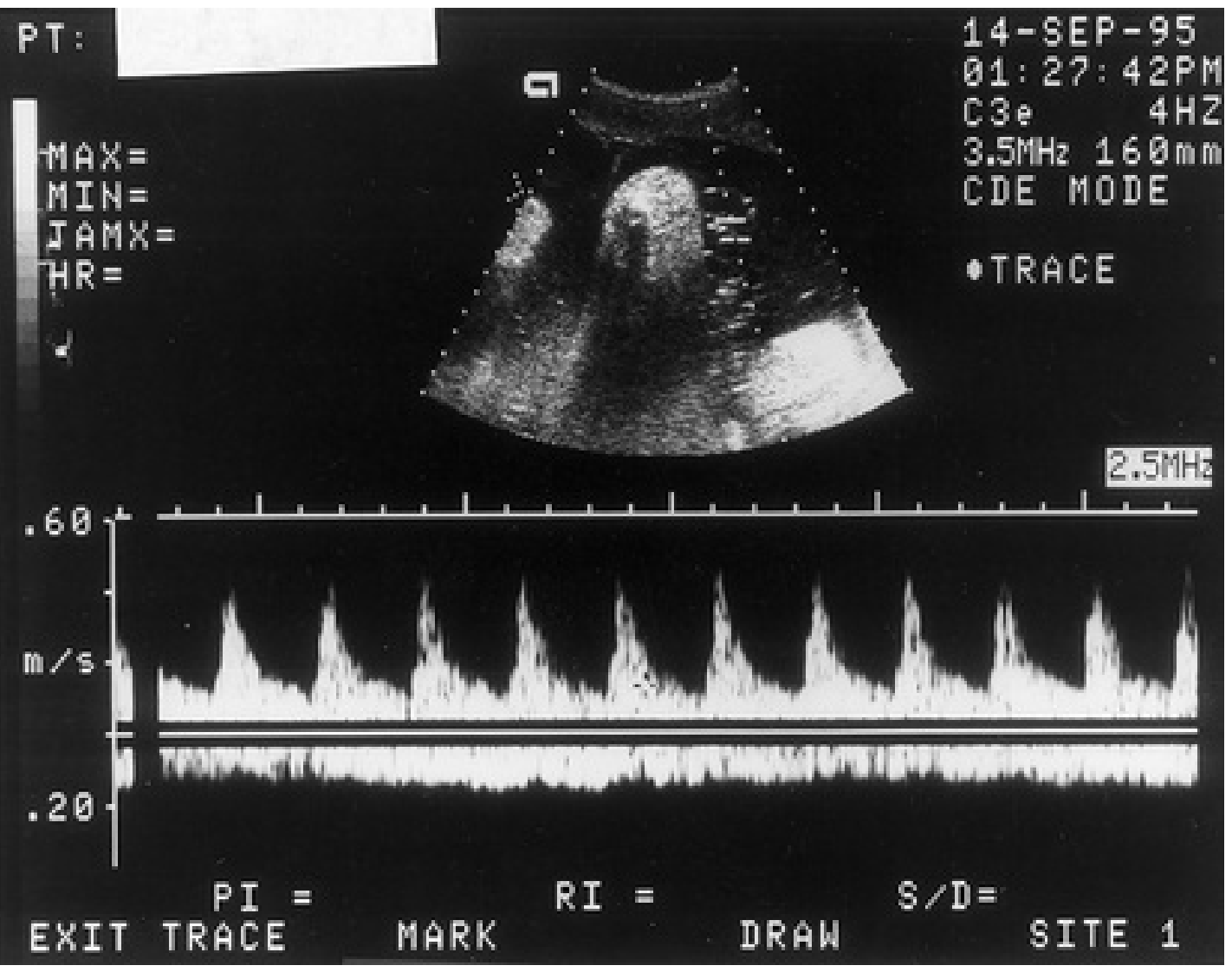
3.6 Doppler Velocimetry — Umbilical Artery (UA)
Most important surveillance tool for FGR. Reflects placental vascular resistance.
| UA Finding | Significance |
|---|---|
| Normal diastolic flow in a small fetus | Usually constitutionally small, well fetus (adverse outcome rate ~1.3%) |
| Diminished end-diastolic flow | Rarely associated with significant morbidity but warrants close monitoring |
| Absent end-diastolic flow (AEDV) | Increased perinatal morbidity and mortality; maldevelopment of placental terminal villi |
| Reversed end-diastolic flow (REDV) | Most severe; 5-fold higher perinatal mortality vs. AEDV |
Pathological basis: AEDV correlates with obliteration of >60–70% of placental vascular cross-sectional area. A Cochrane analysis of 19 RCTs found that UA Doppler assessment was associated with fewer perinatal deaths (RR 0.71), fewer labor inductions, and fewer cesarean sections.
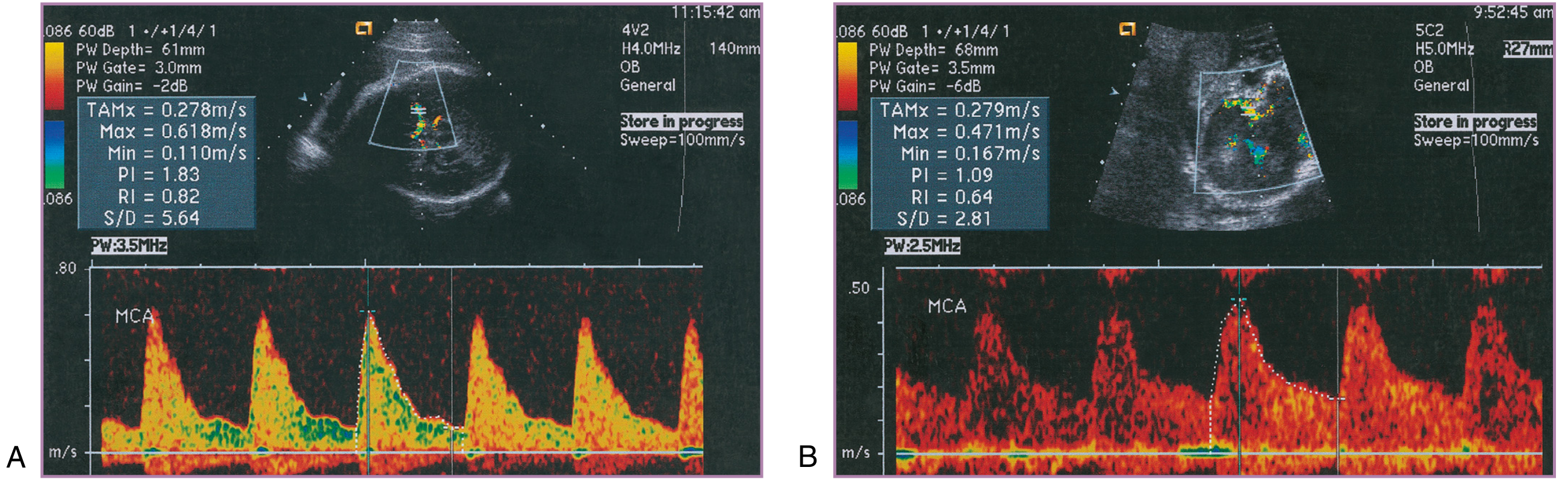
3.7 Middle Cerebral Artery (MCA) Doppler — "Brain-Sparing"
Principle: Chronic fetal hypoxia causes vasodilation of cerebral arteries to maintain oxygen delivery to the brain — detected as a reduced MCA Pulsatility Index (PI).
- Normal MCA: high resistance, low diastolic velocities
- Hypoxic fetus: falling MCA PI (increased diastolic velocities) — centralization of flow
- "Normalization" of MCA PI in a previously brain-sparing fetus is an ominous sign — indicates cardiac decompensation and failure to maintain cerebrovascular response
The cerebroplacental ratio (CPR = MCA PI / UA PI) is used to distinguish the constitutionally small fetus (both PIs normal) from the pathologically growth-restricted fetus (one or both abnormal). An abnormal MCA PI may precede abnormal UA PI in early FGR.
3.8 Ductus Venosus (DV) Doppler
The ductus venosus reflects cardiac function and is the most sensitive venous marker of severe fetal compromise. Its waveform mirrors cardiac events:
- a-wave: Corresponds to atrial systole; normally shows reduced (but forward) flow
- Progressive deepening of a-wave: Rising cardiac afterload from placental resistance
- Absent a-wave: Onset of significant cardiac impairment
- Reversed a-wave: Preterminal sign — severe cardiac decompensation, high risk of fetal demise
The DV can actively dilate in response to hypoxemia, making it uniquely sensitive among venous vessels. DV deterioration frequently precedes BPP changes and strongly predicts the need for delivery.
3.9 Fetal MCA Peak Systolic Velocity (PSV)
Used specifically to screen for fetal anemia (e.g., Rh isoimmunization):
- MCA PSV >1.5 MoM = significant fetal anemia → indication for cordocentesis and intrauterine transfusion
- Anemia causes increased cardiac output → increased MCA PSV
3.10 Umbilical Artery Doppler in Context
From The Developing Human: "Doppler velocimetry of the uteroplacental and fetoplacental circulation is used to investigate complications of pregnancy, such as IUGR and fetal distress resulting from fetal hypoxia and asphyxia... there is a statistically significant association between IUGR and abnormally increased resistance in an umbilical artery."
4. Sequential Deterioration Pattern (Staging of Fetal Compromise)
In placental insufficiency-driven FGR, Doppler changes follow a predictable sequence useful for timing delivery:
1. Abnormal UA Doppler (↑PI or absent/reversed EDF)
↓
2. MCA brain-sparing (↓MCA PI)
↓
3. Oligohydramnios / abnormal BPP
↓
4. Ductus venosus a-wave abnormality (absent → reversed)
↓
5. Umbilical venous pulsations / Fetal bradycardia / non-reactive NST
↓
6. Intrauterine demise
5. Integrated Surveillance Protocol (FGR Example)
From Creasy & Resnik's:
- Weekly BPP/NST + UA and MCA Doppler in FGR
- Fetal growth measurements every ~3 weeks
- For FGR <32 weeks with AEDV/REDV: inpatient monitoring with NST every 8–12 hours + daily BPP
- Delivery timing: at 39 weeks if all parameters remain normal; earlier if deterioration detected
6. Summary Comparison of Methods
| Method | What It Detects | Best Used For |
|---|---|---|
| Kick counting | Reduced fetal activity | First-line maternal screening |
| NST | FHR reactivity (oxygenation) | Routine surveillance, first-line |
| CST/OCT | Uteroplacental reserve | Adjunct when NST non-reactive |
| BPP (5 variables) | Acute + chronic hypoxia | Comprehensive assessment |
| Modified BPP | NST + AFI | Practical daily surveillance |
| UA Doppler | Placental resistance | Primary tool for FGR |
| MCA Doppler | Cerebral redistribution | Distinguish FGR from SGA; anemia |
| DV Doppler | Cardiac function, severe compromise | Timing delivery in severe FGR |
| MCA PSV | Fetal anemia | Rh isoimmunization, hydrops |
Recent Evidence
A 2023 comprehensive review of major guidelines for fetal growth restriction (PMID 38134339) confirms that UA Doppler remains the primary surveillance tool, with MCA and DV Doppler added in high-risk cases. A 2024 prospective study (PMID 38339783) found that growth trajectory assessment identifies infants at highest perinatal mortality risk, reinforcing serial growth measurement.
Sources:
- Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice — Chapter 32 (Antepartum Fetal Surveillance), Chapter on FGR
- The Developing Human: Clinically Oriented Embryology — Umbilical Artery Doppler Velocimetry (p. 381)
This is a shared conversation. Sign in to Orris to start your own chat.