Teach me renal system and blood
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is your complete nursing-level lesson on both systems. Sources: Ganong's Review of Medical Physiology (26e), Histology: A Text and Atlas, Comprehensive Clinical Nephrology (7e).
🫁 PART 1: THE RENAL SYSTEM
1. Overview and Functions of the Kidneys
The kidneys are two bean-shaped organs sitting retroperitoneally (behind the peritoneum) on either side of the vertebral column. Their major functions as a nurse you must know:
| Function | What it means clinically |
|---|---|
| Filter waste | Remove urea, creatinine, drug metabolites from blood |
| Regulate fluid balance | Control how much water stays in the body |
| Regulate electrolytes | Na+, K+, Ca2+, Cl-, phosphate |
| Acid-base balance | Excrete H+ ions, reabsorb bicarbonate |
| Blood pressure control | Via renin-angiotensin system |
| Hormone production | Erythropoietin (stimulates RBC production), calcitriol (active vitamin D) |
| Glucose regulation | Gluconeogenesis during prolonged fasting |
2. Gross Anatomy
Each kidney has three layers:
- Cortex (outer layer) - where most nephrons sit
- Medulla (inner layer) - contains loops of Henle and collecting ducts, arranged in cone-shaped renal pyramids
- Renal pelvis - funnel-shaped area that collects urine and drains into the ureter
Blood supply: The renal arteries branch off the aorta. The kidneys receive about 1,273 mL of blood per minute (about 20-25% of cardiac output) - a massive flow for organs their size.
3. The Nephron - The Functional Unit
Each kidney contains approximately 1 million nephrons. Think of the nephron as a tiny urine-making factory. Each nephron has:
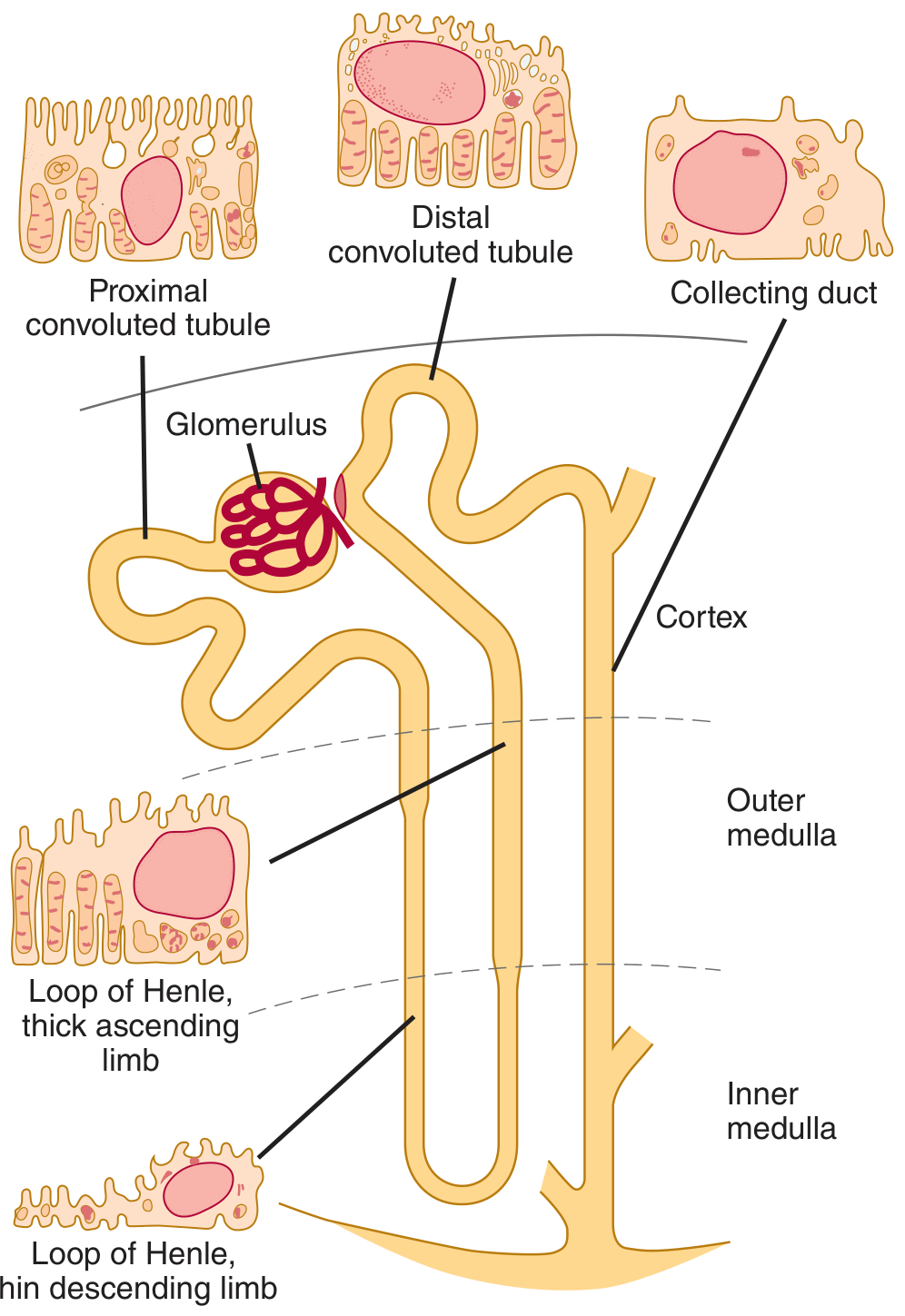
Nephron diagram from Ganong's Review of Medical Physiology, 26e
Parts of the Nephron (in order of flow):
- Bowman's Capsule + Glomerulus - filtration unit (renal corpuscle)
- Proximal Convoluted Tubule (PCT) - major reabsorption site (~15 mm long)
- Loop of Henle (descending + ascending limbs) - concentrates urine
- Distal Convoluted Tubule (DCT) - fine-tunes electrolyte balance
- Collecting Duct - final water reabsorption (controlled by ADH)
4. How Urine is Formed - 3 Processes
Process 1: Glomerular Filtration
Blood enters via the afferent arteriole (wider) into the glomerulus - a tuft of capillaries about 200 μm in diameter. The pressure difference forces fluid out of the blood into Bowman's capsule, forming the glomerular filtrate.
The filtration barrier has 3 layers:
- Fenestrated capillary endothelium (pores 70-90 nm)
- Glomerular basement membrane (negatively charged - repels albumin)
- Podocytes with filtration slits (~25 nm wide)
What gets filtered: Water, glucose, urea, creatinine, electrolytes, small molecules.
What does NOT get filtered: Blood cells, large proteins (albumin), clotting factors.
Key nursing value: GFR (Glomerular Filtration Rate)
- Normal: ~125 mL/min (180 L/day!)
- Only ~1 L becomes urine - meaning 99% of filtrate is reabsorbed
- Used clinically to stage chronic kidney disease (CKD)
- Normal serum creatinine = 1 mg/dL
Process 2: Tubular Reabsorption
As filtrate travels down the tubule, useful substances are pulled back into the blood:
| Tubule Segment | What is Reabsorbed | Key Points |
|---|---|---|
| PCT | ~65% of Na+, water, glucose, amino acids, HCO3- | Brush border (microvilli) increases surface area |
| Loop of Henle (descending) | Water | Permeable to water only |
| Loop of Henle (ascending) | Na+, K+, Cl- | Impermeable to water - creates medullary concentration gradient |
| DCT | Na+ (aldosterone-controlled), Ca2+ (PTH-controlled) | Fine-tuning |
| Collecting Duct | Water (ADH-controlled) | Final concentration of urine |
Glucose threshold: Glucose is fully reabsorbed until plasma glucose ~180 mg/dL. Above this (e.g. in diabetes), it spills into urine - glycosuria.
Process 3: Tubular Secretion
The tubules also actively secrete waste products FROM the blood INTO the filtrate:
- H+ ions (acid-base balance)
- K+ ions (potassium balance)
- Drugs and toxins (penicillin, morphine)
5. Regulation of Kidney Function
Renin-Angiotensin-Aldosterone System (RAAS)
When blood pressure drops or Na+ is low:
- Juxtaglomerular cells (near afferent arteriole) release renin
- Renin converts angiotensinogen → Angiotensin I
- ACE (in lungs) converts Ang I → Angiotensin II
- Angiotensin II: vasoconstricts blood vessels + stimulates aldosterone release
- Aldosterone → kidneys retain Na+ and water → blood pressure rises
Nursing link: ACE inhibitors (e.g., ramipril, lisinopril) block step 3. Widely used for hypertension and CKD protection.
ADH (Antidiuretic Hormone / Vasopressin)
Released from posterior pituitary when blood is too concentrated (high osmolality):
- ADH makes collecting duct permeable to water
- Water is reabsorbed, urine becomes concentrated
- When dehydrated → high ADH → small volume of dark, concentrated urine
- When well-hydrated → low ADH → large volume of dilute urine
6. Key Lab Values to Know
| Test | Normal Range | What Low/High Means |
|---|---|---|
| Serum Creatinine | 0.6-1.2 mg/dL | High = kidney damage |
| BUN (Blood Urea Nitrogen) | 7-20 mg/dL | High = poor kidney clearance or dehydration |
| eGFR | >60 mL/min/1.73m² | <60 for 3 months = CKD |
| Urine specific gravity | 1.005-1.030 | High = concentrated (dehydrated) |
| Urine pH | 4.5-8.0 | Helps assess acid-base status |
7. Common Renal Conditions (nursing-level awareness)
- UTI - ascending infection; most common in females (shorter urethra)
- AKI (Acute Kidney Injury) - sudden drop in GFR, oliguria (<400 mL/day), rising creatinine
- CKD - progressive loss of nephrons; stages 1-5 based on eGFR
- Nephrotic syndrome - damage to filtration barrier → massive proteinuria, edema, hypoalbuminemia
- Nephrolithiasis (kidney stones) - crystallized minerals in renal pelvis; colicky flank pain
🩸 PART 2: BLOOD
1. What is Blood?
Blood is a connective tissue - it has cells (formed elements) suspended in a liquid matrix (plasma). Total blood volume is approximately 5,600 mL (~5.6 L) in a 70 kg person (about 8% of body weight). Of this:
- ~55% is plasma
- ~45% is formed elements (mostly red blood cells - this is the hematocrit)
2. Components of Blood
A. Plasma (55% of blood)
A protein-rich fluid containing:
- Water (~91%)
- Proteins (~7%):
- Albumin - maintains oncotic pressure, transports hormones/drugs; normal = 3.5-5.0 g/dL
- Globulins - immune antibodies (immunoglobulins)
- Fibrinogen - clotting protein made by the liver
- Electrolytes (Na+, K+, Ca2+, Cl-)
- Glucose, hormones, waste products
Key nursing point: Low albumin (hypoalbuminemia) → fluid leaks out of vessels → edema. Seen in liver disease, malnutrition, nephrotic syndrome.
B. Formed Elements (45% of blood)
Red Blood Cells (Erythrocytes)
| Feature | Value |
|---|---|
| Count (male) | 5.4 million/μL |
| Count (female) | 4.8 million/μL |
| Hemoglobin (male) | 16 g/dL |
| Hemoglobin (female) | 14 g/dL |
| Hematocrit (male) | 47% |
| Hematocrit (female) | 42% |
| Mean Cell Volume (MCV) | 87 fL (normal range 80-95 fL) |
| Lifespan | ~120 days |
Structure: Biconcave disc shape (no nucleus in mature RBCs). This shape maximizes surface area for gas exchange and lets them bend through tiny capillaries.
Function: Carry oxygen via hemoglobin (Hb). Each Hb molecule has 4 heme groups, each binding one O2 molecule.
Clinical notes:
- MCV >95 fL = macrocyte (large cell - seen in B12/folate deficiency)
- MCV <80 fL = microcyte (small cell - seen in iron deficiency anemia)
- MCHC <25 g/dL = hypochromic (pale cells - iron deficiency)
Hemolysis warning: Red cells will hemolyze (burst) in hypotonic solutions. A 0.9% NaCl solution is isotonic with plasma. Always use isotonic IV fluids (normal saline, Lactated Ringer's) to prevent hemolysis!
White Blood Cells (Leukocytes)
Normal WBC count: 4,000-11,000/μL
| Type | Normal % | Function | Nursing notes |
|---|---|---|---|
| Neutrophils | 50-70% | First responders; phagocytose bacteria | Elevated in bacterial infections |
| Lymphocytes | 20-40% | T cells (cell immunity), B cells (antibodies) | Elevated in viral infections |
| Monocytes | 2-8% | Become macrophages; phagocytosis | Elevated in chronic infections |
| Eosinophils | 1-4% | Fight parasites; allergic reactions | Elevated in allergies, asthma |
| Basophils | <1% | Release histamine (inflammation/allergy) | Involved in anaphylaxis |
Memory trick: "Never Let Monkeys Eat Bananas" = Neutrophils, Lymphocytes, Monocytes, Eosinophils, Basophils (in order of frequency).
Leukocytosis (WBC >11,000) = infection, inflammation, leukemia Leukopenia (WBC <4,000) = bone marrow suppression, chemotherapy, sepsis (late stage)
Platelets (Thrombocytes)
- Normal count: 150,000-400,000/μL
- Lifespan: ~10 days
- Produced from megakaryocytes in bone marrow
- Function: First step in stopping bleeding (primary hemostasis)
Thrombocytopenia (<150,000) = bleeding risk. Critical concern when <50,000; spontaneous bleeding risk at <20,000.
3. Hematopoiesis - Where Blood Cells Come From
All blood cells originate from Hematopoietic Stem Cells (HSCs) in the bone marrow.
In adults: Active red marrow found in flat bones (sternum, ribs, vertebrae, pelvis, skull) and the proximal ends of the humerus and femur. Long bone shafts become inactive yellow marrow by about age 20.
In fetuses: Blood cells also form in the liver and spleen (extramedullary hematopoiesis), which can recur in adults with bone marrow disease.
HSC (totipotent)
├── Myeloid progenitor
│ ├── RBCs (erythrocytes)
│ ├── Platelets (from megakaryocytes)
│ ├── Neutrophils & Monocytes (common precursor)
│ ├── Eosinophils
│ └── Basophils
└── Lymphoid progenitor
├── T lymphocytes
└── B lymphocytes
The bone marrow is roughly the size and weight of the liver - one of the largest organs in the body. Normally 75% of marrow cells are WBC precursors and only 25% are RBC precursors - because WBCs live for hours to days while RBCs live for 120 days.
4. Hemostasis - How Bleeding Stops
Hemostasis is the process of stopping bleeding. It has 3 stages:
Stage 1: Vascular Spasm
Damaged blood vessel immediately constricts to reduce blood flow.
Stage 2: Primary Hemostasis (Platelet Plug)
- Damaged vessel exposes collagen underneath
- Platelets adhere to collagen (via von Willebrand Factor, vWF)
- Platelets activate and release ADP, thromboxane A2
- More platelets aggregate → platelet plug forms
- This is temporary
Stage 3: Secondary Hemostasis (Coagulation Cascade)
Clotting factors (proteins made mostly by the liver) activate in a cascade to produce fibrin, which reinforces the platelet plug into a stable clot.
Two pathways:
- Intrinsic pathway (triggered by contact with damaged vessel)
- Extrinsic pathway (triggered by tissue factor released from injured tissue)
- Both converge at Factor X → common pathway → thrombin → fibrin clot
Key nursing implications:
- Warfarin (Coumadin) - inhibits Vitamin K-dependent clotting factors (II, VII, IX, X). Monitor with PT/INR.
- Heparin - inhibits thrombin and Factor Xa. Monitor with aPTT.
- Vitamin K deficiency (in liver disease, malnutrition, newborns) = bleeding risk.
5. Blood Types (ABO and Rh System)
| Blood Type | Antigens on RBC | Antibodies in Plasma | Can donate to | Can receive from |
|---|---|---|---|---|
| A | A | Anti-B | A, AB | A, O |
| B | B | Anti-A | B, AB | B, O |
| AB | A and B | None | AB only | All (universal recipient) |
| O | None | Anti-A and Anti-B | All (universal donor) | O only |
Rh factor: If Rh antigen is present = Rh positive (+). If absent = Rh negative (-).
Critical nursing point: Rh-negative mothers carrying Rh-positive babies risk hemolytic disease of the newborn in subsequent pregnancies. Give Rh immunoglobulin (RhoGAM) at 28 weeks and after delivery.
6. Key Blood Lab Values for Nurses
| Test | Normal Range | Clinical Significance |
|---|---|---|
| Hemoglobin | M: 13.5-17.5 g/dL; F: 12-15.5 g/dL | Low = anemia |
| Hematocrit | M: 41-53%; F: 36-46% | Low = anemia; High = dehydration or polycythemia |
| WBC | 4,000-11,000/μL | High = infection; Low = immunosuppression |
| Platelets | 150,000-400,000/μL | Low = bleeding risk |
| PT/INR | INR 0.8-1.2 (therapeutic 2-3) | Monitors warfarin, liver function |
| aPTT | 25-35 seconds | Monitors heparin |
7. The Renal-Blood Connection
These two systems are deeply connected:
- Kidneys produce erythropoietin (EPO) → stimulates bone marrow to make RBCs. In CKD, EPO production falls → anemia of chronic kidney disease
- Kidneys regulate potassium - hyperkalemia (>5.5 mEq/L) in kidney failure can cause fatal cardiac arrhythmias
- Kidneys activate Vitamin D (calcitriol) → regulates calcium → affects bone marrow environment
- Blood carries oxygen and nutrients to the kidney; ~25% of cardiac output goes to the kidneys every minute
Quick Summary Tables
Renal System at a Glance
| Structure | Key Function |
|---|---|
| Glomerulus | Filtration (GFR 125 mL/min) |
| PCT | Reabsorption (glucose, Na+, water) |
| Loop of Henle | Concentration gradient |
| DCT | Aldosterone-regulated Na+ reabsorption |
| Collecting Duct | ADH-regulated water reabsorption |
| Juxtaglomerular cells | Renin secretion (blood pressure control) |
Blood at a Glance
| Component | Key Function | Normal Value |
|---|---|---|
| RBCs | O2 transport via Hb | 4.8-5.4 million/μL |
| WBCs | Immunity and defense | 4,000-11,000/μL |
| Platelets | Primary hemostasis | 150,000-400,000/μL |
| Plasma proteins | Oncotic pressure, clotting, transport | Albumin 3.5-5.0 g/dL |
Sources: Ganong's Review of Medical Physiology (26e), Ch. 31 & 37 | Histology: A Text and Atlas | Comprehensive Clinical Nephrology (7e)
This is a shared conversation. Sign in to Orris to start your own chat.