Dental caries
Reading File
Finding Sources
Finding Sources
Searching PubMed
"dental caries"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Let me compile a thorough response on dental caries.
Dental Caries
Dental caries (tooth decay) is a dynamic, multifactorial, infectious disease of teeth characterized by progressive dissolution of mineralized tooth tissue driven by acid produced by plaque bacteria metabolizing dietary carbohydrates.
Pathophysiology
The four-factor model: The development of caries depends on the interplay of four essential factors:
| Factor | Role |
|---|---|
| Dental plaque | Microbial biofilm adherent to tooth surfaces; creates a microenvironment that favours demineralization and shields bacteria from salivary buffering |
| Substrate | Refined and naturally occurring fermentable carbohydrates (especially sucrose); provides fuel for bacterial acid production |
| Dental factors | Anatomical sites favouring plaque accumulation - pits, fissures, interproximal contacts, poor restoration margins |
| Saliva | Provides buffering, antibacterial activity, and remineralization capacity; when compromised, caries risk rises sharply |
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, p. 701
Cariogenesis: Step by Step
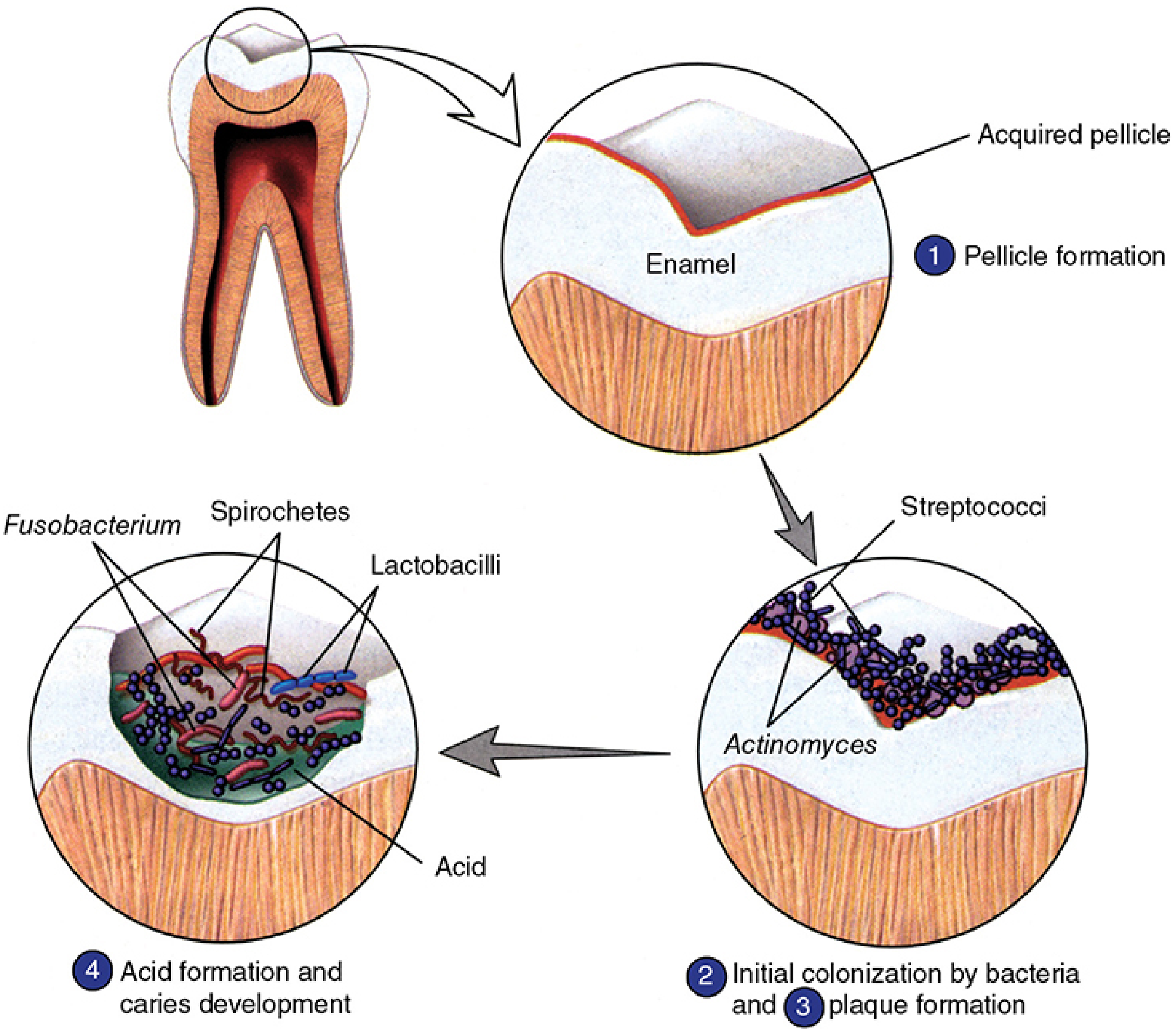
Cariogenesis (Sherris & Ryan's Medical Microbiology): (1) Acquired pellicle forms on enamel. (2) Initial colonization by Streptococci and Actinomyces. (3) Mature plaque biofilm develops. (4) Acid production drives enamel demineralization.
Stage 1 - Pellicle formation: A salivary glycoprotein film (acquired pellicle) coats the enamel surface within minutes of tooth cleaning.
Stage 2 - Bacterial colonization: Early colonizers, predominantly Streptococcus mutans and Actinomyces species, adhere to the pellicle.
Stage 3 - Plaque (biofilm) maturation: The biofilm matures with additional organisms - S. salivarius, S. sanguis, S. sobrinus, Lactobacillus acidophilus, L. casei, A. viscosus, and A. naeslundii.
Stage 4 - Acid production and demineralization: Plaque bacteria ferment dietary carbohydrates (glucose, fructose, sucrose, lactose, maltose). The pH at the plaque-enamel interface drops below critical (approximately pH 5.5), dissolving hydroxyapatite into soluble calcium and phosphate ions.
- Sherris & Ryan's Medical Microbiology, 8th Edition, p. 1503-1506
Why S. mutans is Most Cariogenic
S. mutans has several virulence properties that make it the dominant caries-initiating organism:
- Efficient sucrose metabolism - metabolizes sucrose more rapidly than other oral bacteria via glycolysis
- Glucosyltransferases - synthesizes extracellular polyglucans (dextrans, levans) that promote bacterial aggregation and adherence to tooth surfaces
- Extracellular polysaccharide storage - stores carbohydrate extracellularly and breaks it down during substrate shortage, prolonging acid production beyond oral clearance time
- Intracellular glycogen - similarly prolongs acidogenesis after the dietary substrate is exhausted
- Acid tolerance - can survive and continue producing acid at lower pH levels than most competing oral bacteria
- Sherris & Ryan's Medical Microbiology, 8th Edition, p. 1505-1506
Demineralization - Remineralization Cycle
A critical concept: caries is not a one-way process. Acid demineralizes enamel, but when substrate runs out, the plaque pH returns toward neutral and saliva drives partial remineralization. Repeated snacking prevents pH recovery, causing demineralization to dominate. This is why snacking frequency matters more than total sugar intake.
Progression of Disease
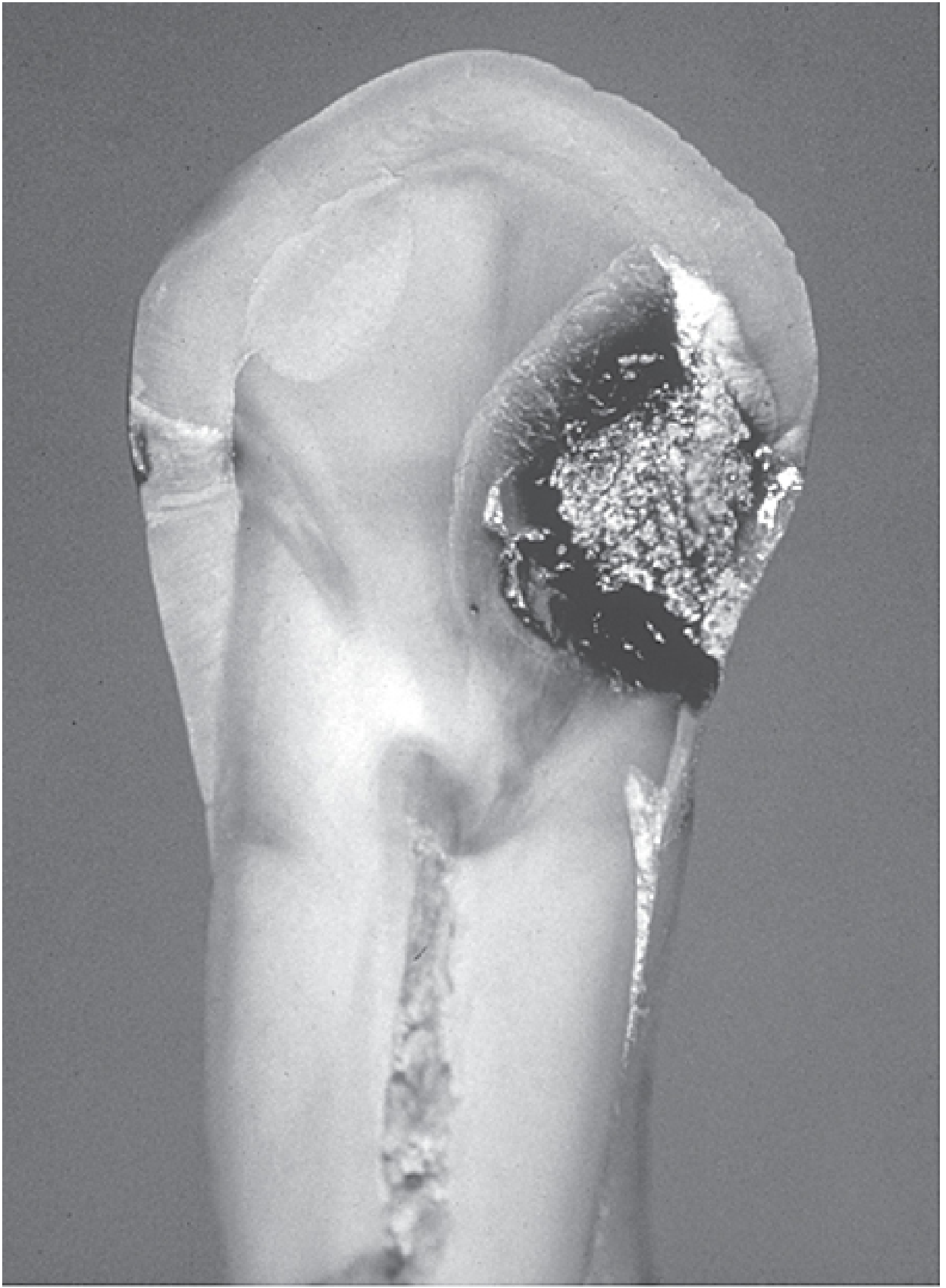
Advanced carious lesion: note progression through enamel and dentin pointing toward the pulp (Sherris & Ryan's Medical Microbiology).
The lesion progresses inward from the tooth surface:
- Initial enamel lesion (white spot): Subsurface demineralization, no cavitation. The surface enamel remains intact due to salivary remineralization. Reversible at this stage with preventive treatment.
- Enamel caries: Acid permeates alongside enamel prism sheaths, causing localized enamel dissolution.
- Dentine-enamel junction (DEJ) involvement: Once the DEJ is breached, caries spreads rapidly along dentinal tubules. Cavitation occurs. The lesion is no longer self-limiting.
- Dentine caries: Acid dissolution, proteolysis, and bacterial invasion of dentinal tubules. Sensitivity to cold/sweet stimuli develops (reversible pulpitis).
- Pulp involvement (pulpitis): Bacteria reach the vital pulp, causing inflammation.
- Reversible pulpitis: Pain lasts seconds, triggered by cold or sweet stimuli.
- Irreversible pulpitis: Pain lasts minutes to hours; may be spontaneous and throbbing.
- Pulpal necrosis → periapical extension: Infection spreads through root canals to periapical tissues, forming periapical abscess, periapical granuloma, or radicular cyst.
- Tintinalli's Emergency Medicine, p. 1623; Scott-Brown's Otorhinolaryngology, p. 701-702
Complications
| Complication | Description |
|---|---|
| Irreversible pulpitis | Persistent pain; requires root canal or extraction |
| Pulpal necrosis | Asymptomatic or acute; precedes periapical spread |
| Periapical abscess | Acute suppurative inflammation at root apex |
| Periapical granuloma | Chronic non-suppurating lesion |
| Radicular cyst | Cyst forming within granuloma |
| Osteomyelitis | Spread to alveolar bone |
| Fascial space infection | Cellulitis spreading along head and neck fascial planes |
| Septic thrombophlebitis | Venous ascent of infection |
In immunocompromised patients or with virulent organisms, spread to fascial spaces of the head and neck (e.g., Ludwig's angina) can be life-threatening.
- Sherris & Ryan's Medical Microbiology, 8th Edition, p. 1506
Risk Factors
- High fermentable carbohydrate intake (especially sucrose) with long oral clearance times
- Frequent snacking (prevents pH recovery)
- Poor oral hygiene / inadequate plaque removal
- Hyposalivation (xerostomia from medications, Sjogren's, radiation)
- Narrow pits and fissures, poor interdental contacts, inadequate restoration margins
- Inadequate fluoride exposure
- Smokeless tobacco use
- Early childhood: rampant caries may be the only sign of underlying hyposalivation
Diagnosis
- Clinical: Visual and tactile examination (blunt dental probe) - cavitation, discoloration
- Radiographic: Bitewing radiographs detect interproximal and sub-surface lesions; periapical X-rays evaluate pulp and periapical involvement
- Newer adjuncts: Laser fluorescence (DIAGNOdent), transillumination, AI-assisted radiographic detection (emerging evidence)
Treatment
Preventive / Early lesion (no cavitation)
- Topical fluoride application (promotes remineralization, inhibits acid production)
- Fissure sealants
- Dietary counseling (reduce snacking frequency, limit sucrose)
- Chlorhexidine (reduces S. mutans load)
- Oral hygiene instruction
Established caries with cavitation
- Operative treatment: remove carious tissue, restore tooth with amalgam, composite resin, glass ionomer, or indirect ceramic restoration
Pulpitis
- Reversible: Removal of carious tissue + restoration may suffice
- Irreversible / pulpal necrosis: Root canal treatment (RCT) or extraction; NSAIDs ± acetaminophen for pain (preferred over opioids by the American Dental Association); local anesthetic block for acute pain management
Periapical abscess
-
Drainage (incision and drainage if fluctuant); appropriate antibiotics; root canal or extraction
-
Amoxicillin is first-line; clindamycin for penicillin allergy
-
Tintinalli's Emergency Medicine, p. 1623; Scott-Brown's Otorhinolaryngology, p. 702
Prevention - Public Health Perspective
-
Water fluoridation is the cornerstone population-level intervention
-
Fluoride toothpaste prevents caries across all age groups
-
Reducing free sugar intake - WHO recommends <10% of total energy from free sugars
-
Dental caries remains the most prevalent non-communicable disease globally; severe tooth loss was among the top 10 causes of years lived with disability in high-income countries
-
Park's Textbook of Preventive and Social Medicine; Katzung's Basic and Clinical Pharmacology, 16th Ed.
Recent Evidence (2024-2025)
- A 2025 systematic review and meta-analysis (Mazurel et al., J Dent Res, PMID 39895020) confirmed S. mutans as the dominant caries-associated organism, reinforcing classical microbiology.
- A 2024 meta-analysis (Maklennan et al., BMC Oral Health, PMID 39049051) provided updated global prevalence data on early childhood caries, highlighting it as a major pediatric public health burden.
- AI-assisted caries detection on dental radiographs is a growing area, with a 2024 umbrella review (Negi et al., Clin Exp Dent Res, PMID 39206581) summarizing promising but still-developing evidence for clinical implementation.
This is a shared conversation. Sign in to Orris to start your own chat.