How to differentiate arteritic vs non arteritic crao clinically and on fundus Examination with difference in ffa images and treatment
Reading File
Finding Sources
Finding Sources
Searching PubMed
arteritic non-arteritic central retinal artery occlusion differentiation
Reading File
Reading File
Reading File
Searching PubMed
central retinal artery occlusion giant cell arteritis
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Loading Image
Finding Sources
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Loading Image
I now have all the information needed for a comprehensive answer. Let me compile the full response.
Arteritic vs Non-Arteritic CRAO: Complete Differentiation
Overview
Central retinal artery occlusion (CRAO) can be:
- Non-arteritic (NA-CRAO) - >90% of all cases; embolic or thrombotic in origin
- Arteritic (A-CRAO) - caused by Giant Cell Arteritis (GCA/temporal arteritis); ~5-10% of cases; a sight-threatening and life-threatening emergency
Clinical Differentiation
Systemic Features
| Feature | Non-Arteritic CRAO | Arteritic CRAO (GCA) |
|---|---|---|
| Age | 50-70 years | Usually >70 years (rarely <55) |
| Pain | Painless | Painful - jaw claudication, scalp tenderness, temporal headache |
| Systemic symptoms | None specific | Fever, malaise, weight loss, polymyalgia rheumatica |
| Temporal artery | Normal | Tender, thickened, nodular, non-pulsatile |
| Risk factors | Atherosclerosis, HTN, DM, hyperlipidemia, AF, carotid disease | Systemic vasculitis (GCA) |
| Preceding TIA | Amaurosis fugax may precede | Less typical |
| ESR/CRP | Normal | Markedly elevated (ESR often >50 mm/hr, CRP elevated) |
| Platelets | Normal | Often elevated |
| Fellow eye risk | Low for CRAO | Very high - bilateral involvement in >50% if untreated |
Kanski's Clinical Ophthalmology: "Sudden profound loss of vision, painless except in GCA" - the presence of pain is the single most important clinical differentiator.
Fundus Examination Differences
Non-Arteritic CRAO
Classic findings:
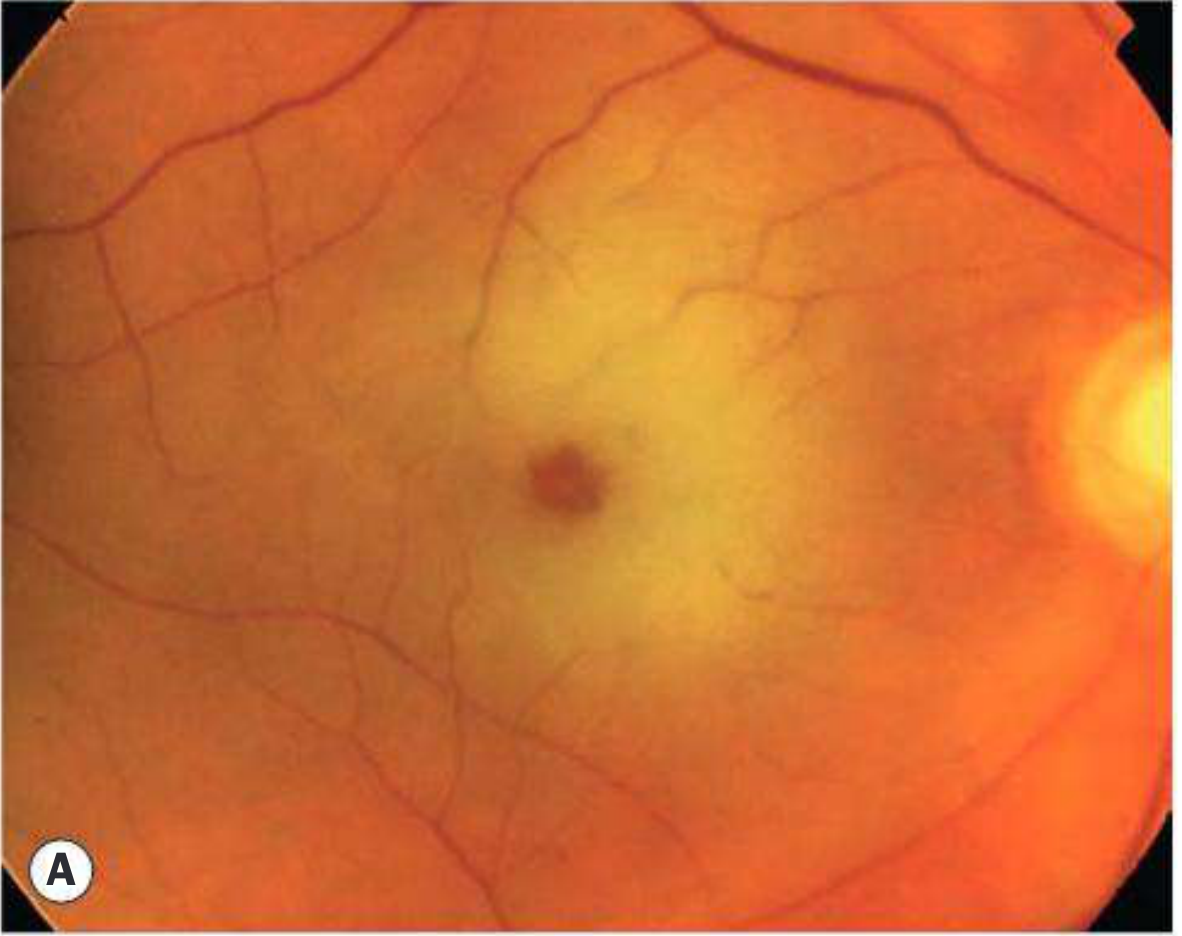

- Cherry-red spot at the fovea (hallmark) - the orange choroidal reflex shows through the thin, avascular foveola against the surrounding pale edematous retina
- Diffuse milky-white retinal edema in the posterior pole
- Attenuated retinal arterioles with "boxcarring" or "cattle trucking" (segmentation of blood column)
- Emboli visible in ~20% - at arteriolar bifurcations (Hollenhorst cholesterol plaques = refractile yellow; calcium = white; platelet-fibrin = dull white)
- Cilioretinal artery sparing - if present, an island of normal-colored retina at the macula preserves some central vision
- Occasional small hemorrhage
- Disc may appear normal initially; peripapillary retina especially swollen
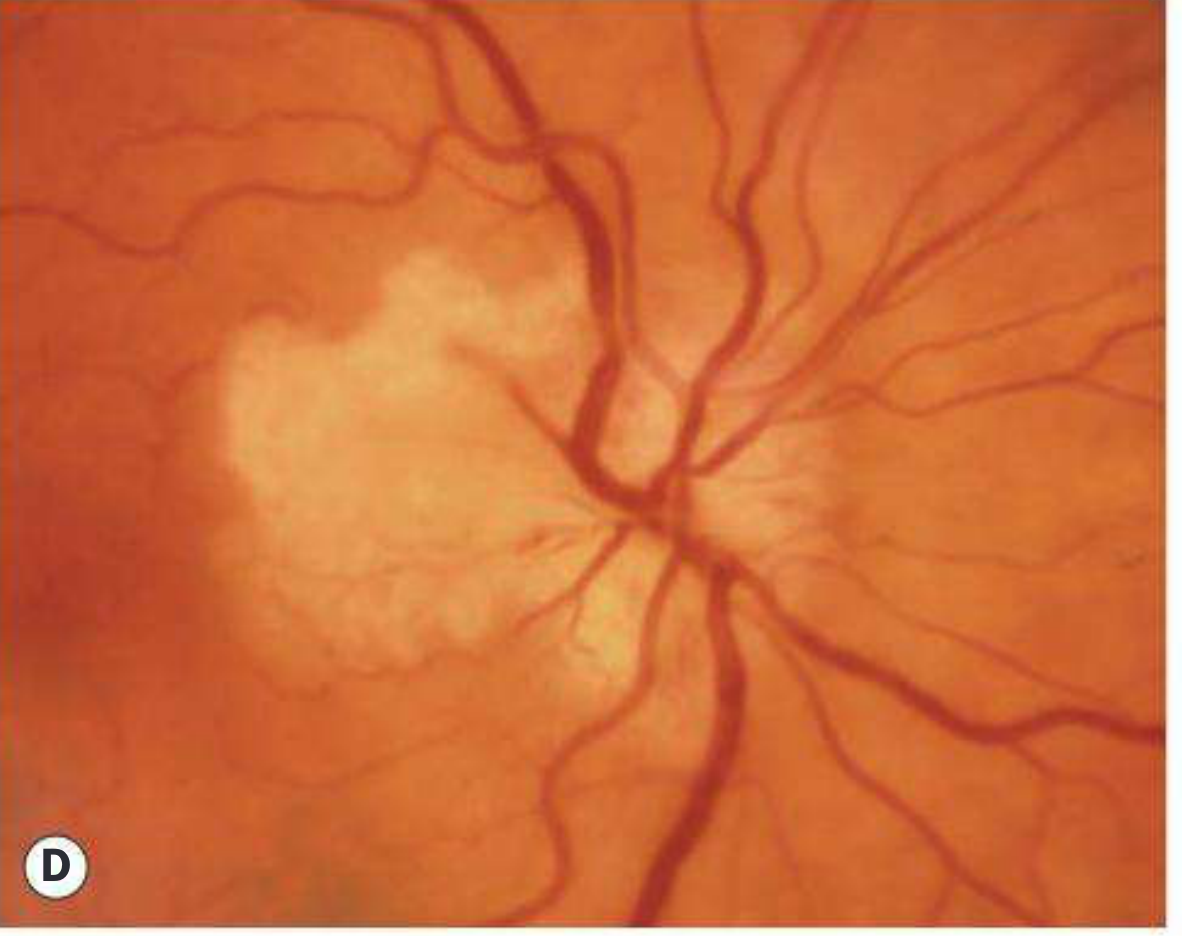
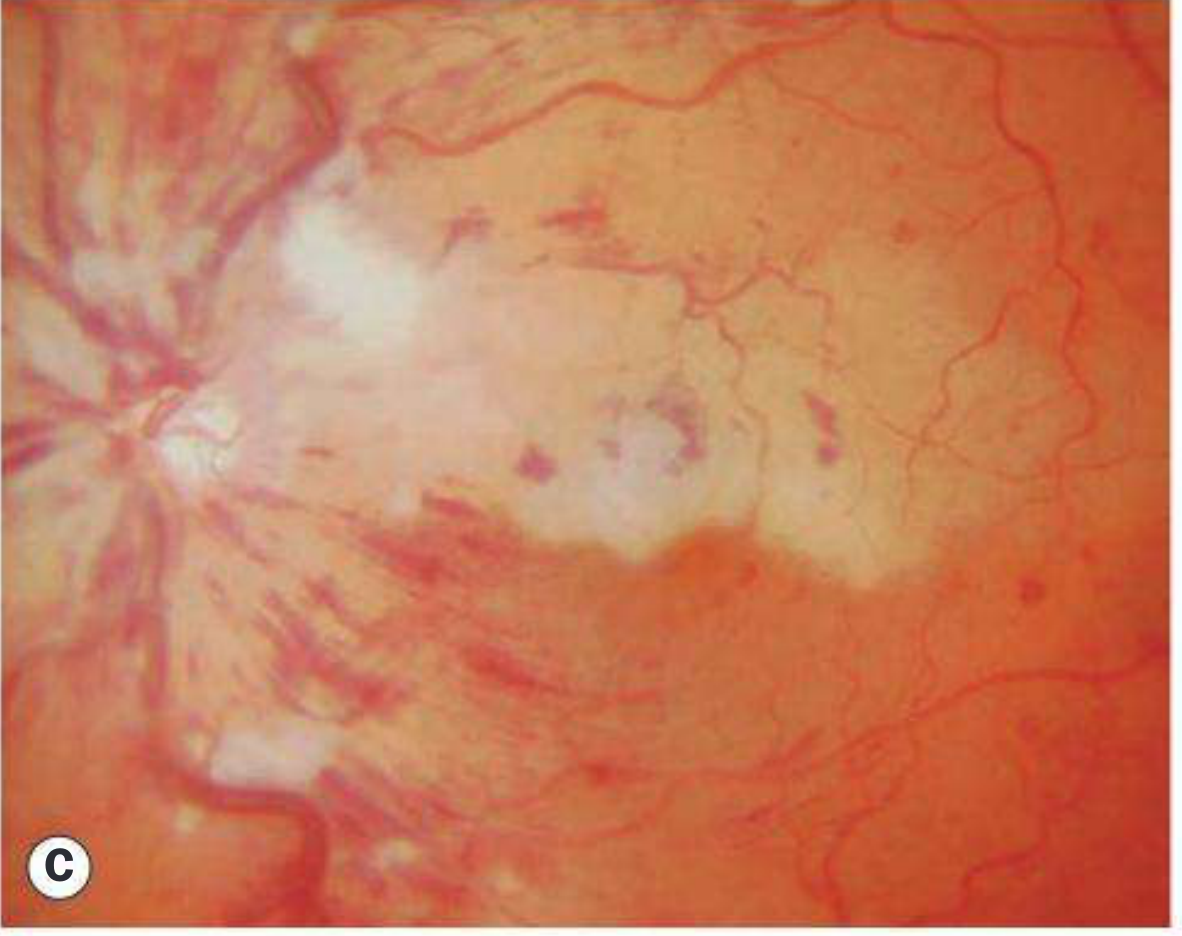
Arteritic CRAO (GCA)
- No cherry-red spot (or less prominent cherry-red spot) - this is the key fundus differentiator
- If the ophthalmic artery is also involved (common in GCA), the entire retina including the foveola is white/chalky, obliterating the cherry-red appearance
- VA = no light perception - absence of any light perception strongly points to GCA or ophthalmic artery occlusion
- The disc may show ischemic pallor/swelling (concurrent arteritic AION is common in GCA)
- Choroidal involvement: GCA typically involves the posterior ciliary arteries too, so you may see choroidal ischemia (triangular/geographic pale areas) alongside retinal whitening
- No visible emboli (it is a vasculitis/inflammation of the vessel wall, not embolic)
FFA (Fluorescein Angiography) Differences
Both Types Share These General CRAO FFA Features
- Delayed or absent arterial filling (prolonged arteriovenous transit time)
- Hypofluorescence of the posterior pole from masking of choroidal fluorescence by edematous/opaque retina
- Slow, stuttering arterial filling with "pruning" of arterioles
- In recovery phase: arteriovenous shunting or re-canalization
Non-Arteritic CRAO - FFA
| Phase | Finding |
|---|---|
| Choroidal phase | Normal/near-normal choroidal flush - background fluorescence of choroid is intact and appears at normal time |
| Arterial phase | Grossly delayed or absent; central retinal artery fills very late or not at all |
| Venous phase | Prolonged laminar venous flow; delayed AV transit |
| Cilioretinal artery | If present, fills early during the choroidal phase (before the CRA fills) - this is a key FFA finding |
| Late phase | Disc hyperfluorescence from staining; retinal edema masks background choroidal fluorescence |
Key FFA point for non-arteritic: The choroidal circulation (posterior ciliary arteries) fills normally because the occlusion is at or distal to the lamina cribrosa within the central retinal artery only. The background choroidal flush is preserved but masked by overlying retinal edema.
Arteritic CRAO (GCA) - FFA
| Phase | Finding |
|---|---|
| Choroidal phase | Delayed/absent or patchy choroidal flush - this is the critical differentiator on FFA |
| Choroidal filling | Geographic/sectoral areas of choroidal non-perfusion (triangular, wedge-shaped hypofluorescent zones corresponding to short posterior ciliary artery territories) |
| Arterial phase | Absent or severely delayed, similar to NA-CRAO |
| Optic disc | Hypofluorescent disc (ischemic disc) in concurrent AION; no normal disc perfusion |
| Late phase | Disc staining may be absent (unlike NA-CRAO where disc often stains) |
The critical FFA differentiator: In arteritic CRAO, the choroidal circulation is also compromised because GCA involves the posterior ciliary arteries (which are branches of the ophthalmic artery, the site of granulomatous vasculitis). This results in patchy choroidal non-perfusion visible on FFA. In non-arteritic CRAO, the choroid fills normally since only the central retinal artery is blocked.
Summary Comparison Table
| Parameter | Non-Arteritic CRAO | Arteritic CRAO |
|---|---|---|
| Cause | Embolus, thrombosis | GCA (giant cell arteritis) |
| Pain | No | Yes (headache, jaw claudication) |
| Vision loss | Profound; light perception often preserved | Profound; often no light perception |
| Amaurosis fugax | May precede | Uncommon |
| Cherry-red spot | Present (hallmark) | Absent or poorly defined |
| Emboli on fundus | Visible in 20% | Absent |
| Disc | Normal/slightly swollen | Ischemic swelling (AION component) |
| Choroidal involvement | None | Present (ciliary artery ischemia) |
| ESR/CRP | Normal | Elevated |
| FFA: Choroid | Normal filling | Patchy/absent filling (geographic) |
| FFA: CRA filling | Delayed/absent | Absent |
| FFA: Choroidal flush | Present (masked by edema) | Delayed/patchy/absent |
| Bilateral risk | Low (<1%) | Very high (>50% untreated) |
Treatment
Non-Arteritic CRAO
Time window is critical - irreversible damage within ~4 hours (primate data); human threshold uncertain
Acute (<4.5 hours from onset):
- Ocular massage with fundus contact lens or digital massage (firm pressure for 10-15 sec, release) - to dislodge emboli
- Anterior chamber paracentesis - to rapidly lower IOP and increase perfusion pressure
- IOP lowering - acetazolamide 500 mg IV/PO; topical beta-blocker (timolol 0.5%)
- IV alteplase (tPA) - 0.9 mg/kg (10% over 1 min, remainder over 59 min); consider within 4.5 hours of onset; treat as acute ischemic stroke
- Intra-arterial thrombolysis (ophthalmic artery) - may have benefit within 6 hours; evidence remains heterogeneous
- Rebreathing CO2 (5% CO2 / 95% O2 carbogen) - vasodilatory; largely anecdotal
- Nd:YAG embolysis - if visible embolus; variable success; risk of vitreous/subretinal hemorrhage
- Refer immediately to stroke center (AAO 2018 guidelines)
Workup (non-arteritic):
- CBC, fasting glucose, HbA1c, lipid profile, PT/PTT
- Carotid Doppler (30% have severe carotid disease)
- ECG + echocardiography (cardiac embolism workup)
- In patients <50 years: hypercoagulable screen (ANA, antiphospholipid Ab, protein C/S, factor V Leiden, homocysteine, SPEP)
- ESR/CRP/platelets if age ≥55 (to rule out GCA)
Follow-up:
- Ophthalmic review at 3-4 weeks, then monthly for 2 more months
- Monitor for rubeosis iridis (up to 1 in 5 eyes, usually at 4-5 weeks) and NVD/NVE (~2%) - treat with PRP and/or anti-VEGF if neovascularization develops
Arteritic CRAO (GCA) - Emergency
This is a true ophthalmic emergency. Do not delay for biopsy.
- Immediate high-dose IV corticosteroids - methylprednisolone 500 mg-1 g IV daily for 3 days, then transition to oral prednisolone 1 mg/kg/day
- Do NOT wait for temporal artery biopsy results before starting steroids
- Biopsy should be performed within 1-2 weeks (steroid effect on biopsy is minimal in the first 2 weeks)
- Goal: Prevent fellow eye involvement (bilateral blindness risk >50% if untreated)
- Aspirin (low-dose) may be added for its anti-platelet/anti-inflammatory effect
- NO thrombolytics - not indicated; the mechanism is vasculitis, not thromboembolism
- Tocilizumab (IL-6 inhibitor) - now used for long-term GCA management/steroid-sparing
- Urgent rheumatology referral
- Temporal artery biopsy as soon as logistically possible (same side as symptoms)
Kanski's Clinical Ophthalmology (10e) - Key clinical pearl: "Absence of light perception usually indicates either GCA or ophthalmic artery occlusion." This sign should trigger immediate ESR/CRP and steroids.
Wills Eye Manual: "If GCA suspected, start high-dose systemic steroids immediately. Immediate ESR, CRP, and platelets in all patients ≥55 years with no visible embolus."
Quick Clinical Algorithm
Sudden profound painless monocular vision loss
↓
Age ≥55 years?
↓ ↓
YES NO → Non-arteritic workup → Stroke center
↓
Check ESR/CRP/Plt + query GCA symptoms
↓
Cherry-red spot present? Embolus visible?
Choroid looks normal? → NON-ARTERITIC
↓
No cherry-red spot? NLP? Disc swollen?
Headache/jaw claudication? ESR elevated? → ARTERITIC GCA
↓
Immediate IV methylprednisolone (do not wait for biopsy)
Sources: Kanski's Clinical Ophthalmology 10e, p. 551-555; Wills Eye Manual 8e, p. 782-785; Rosen's Emergency Medicine 10e, p. 4282-4332
This is a shared conversation. Sign in to Orris to start your own chat.