Diabetes
Reading File
Asking for Preferences
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Searching PubMed
"type 1 diabetes" AND pathogenesis
Excellent - rich content from three major textbooks. Let me now compile a thorough answer.
Pathophysiology of Type 1 Diabetes Mellitus (T1DM)
Overview
Type 1 DM is a syndrome of impaired carbohydrate, fat, and protein metabolism resulting from an absolute deficiency of insulin caused by destruction of the insulin-secreting pancreatic beta (β) cells. It accounts for approximately 5-10% of all diabetes cases.
- Guyton and Hall Textbook of Medical Physiology, p. 973
- Tietz Textbook of Laboratory Medicine, 7th Ed.
1. Triggering Factors
A complex interplay of genetic, environmental, and autoimmune factors drives selective destruction of β cells:
-
Viral infections (e.g., enteroviruses, Coxsackievirus B) can trigger or accelerate β-cell destruction
-
Environmental triggers are strongly implicated - even identical twins show only 30-40% concordance, meaning non-genetic factors are essential
-
Hereditary predisposition to β-cell degeneration can exist even without overt infection or autoimmune disease
-
Goldman-Cecil Medicine, block 37
2. Genetic Susceptibility
About 60 genes contribute to T1DM susceptibility:
| Gene/Locus | Contribution |
|---|---|
| HLA genes (chr. 6p) | ~50% of genetic susceptibility |
| HLA DR4-DQ8 and DR3-DQ2 haplotypes | Present in ~90% of children with T1DM |
| DR4-DQ8 + DR3-DQ2 genotype (both) | Highest risk (~5%), early-onset disease |
| DR15-DQ6 haplotype | Highly protective - found in only 1% of T1DM vs. 20% of general population |
| Insulin gene (chr. 11) | Contributes to susceptibility |
| IFIH1 (chr. 2) | Encodes innate immunity protein; involved in viral RNA recognition |
Nonidentical HLA-identical siblings of a proband carry a 12-15% risk of developing T1DM by age 20. Fathers with T1DM have a higher risk of passing it to offspring (6-9%) than mothers (1-3%).
- Goldman-Cecil Medicine, block 37
3. Autoimmune Mechanism
T1DM is predominantly classified as Type 1A (immune-mediated).
Cellular Immunity (Primary Driver)
- CD8+ cytotoxic T cells and CD4+ helper T cells infiltrate the islets - this inflammatory infiltrate is called insulitis
- T-cell mediated immune responses cause apoptosis or direct cellular destruction of β cells
- Macrophages also participate in the inflammatory infiltrate
Humoral Immunity (Antibody Markers)
Over 90% of newly diagnosed T1DM patients have one or more autoantibodies:
| Autoantibody | Target | Notes |
|---|---|---|
| GAD65 antibodies | Glutamic acid decarboxylase | Most widely tested |
| IA-2 antibodies | Tyrosine phosphatase (islet β cells) | Highly specific |
| ZnT8 antibodies | Zinc transporter (IA-2β) | Newer marker |
| IAA (Insulin autoantibodies) | Insulin | ~80-90% of children < age 5; <40% if onset after age 12 |
| ICA (Islet cell cytoplasmic antibodies) | Sialoglycoconjugate in islet cytoplasm | Found in 75-85% at diagnosis |
-
The autoimmune process begins months to years before clinical presentation
-
80-90% reduction in β-cell volume is required before symptomatic T1DM appears
-
2 or more autoantibodies in a normoglycemic relative = highly predictive of T1DM within 5 years
-
Tietz Textbook of Laboratory Medicine, block 19; Goldman-Cecil Medicine, block 37
4. Selective β-Cell Destruction
- The autoimmune attack is highly selective - only β cells are destroyed
- α cells (glucagon), δ cells (somatostatin), and other islet cells remain intact
- Over time, islets become completely devoid of β cells and inflammatory infiltrates
- Destruction is more rapid in children than in adults; adults may follow a slower course called LADA (Latent Autoimmune Diabetes in Adults)
5. Metabolic Consequences of Absolute Insulin Deficiency
Once β-cell mass falls below the critical threshold, insulin deficiency causes widespread metabolic disruption:
Glucose Metabolism
- Decreased peripheral glucose uptake + increased hepatic glucose production
- Blood glucose rises to 300-1200 mg/dL in severe, untreated disease
- Renal glucose threshold (~200 mg/dL) is exceeded → glycosuria
- Glycosuria causes osmotic diuresis → polyuria, polydipsia, dehydration
Fat Metabolism
- Massive fat mobilization from adipose tissue
- Hepatic fatty acid oxidation → ketone body formation (acetoacetate, β-hydroxybutyrate, acetone)
- Accumulation of ketones → diabetic ketoacidosis (DKA) - a life-threatening complication more characteristic of T1DM than T2DM
Protein Metabolism
-
Protein catabolism predominates
-
Amino acids converted to glucose (gluconeogenesis) → muscle wasting, weight loss
-
Nitrogen excretion increases
-
Guyton and Hall Textbook of Medical Physiology, p. 973-975
6. Disease Progression Summary
Genetic susceptibility (HLA + other loci)
↓
Environmental trigger (viral infection, gut microbiome, etc.)
↓
Initiation of autoimmunity (T-cell activation against β-cell antigens)
↓
Insulitis (CD4+/CD8+ T cells + macrophages infiltrate islets)
↓
Progressive β-cell destruction (months to years — subclinical phase)
↓
~80-90% β-cell loss → Symptomatic hyperglycemia
↓
Absolute insulin deficiency → Polyuria, polydipsia, weight loss, DKA
Idiopathic Type 1B
A small subset of T1DM patients have no evidence of autoimmunity - this is termed idiopathic (Type 1B) diabetes. The mechanism is poorly understood but leads to the same outcome: absolute insulin deficiency.
Sources: Goldman-Cecil Medicine (International Edition), Tietz Textbook of Laboratory Medicine 7th Ed., Guyton and Hall Textbook of Medical Physiology.
Circle of willia
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Excellent - comprehensive content from multiple textbooks plus a clear diagram. Here is the full answer:
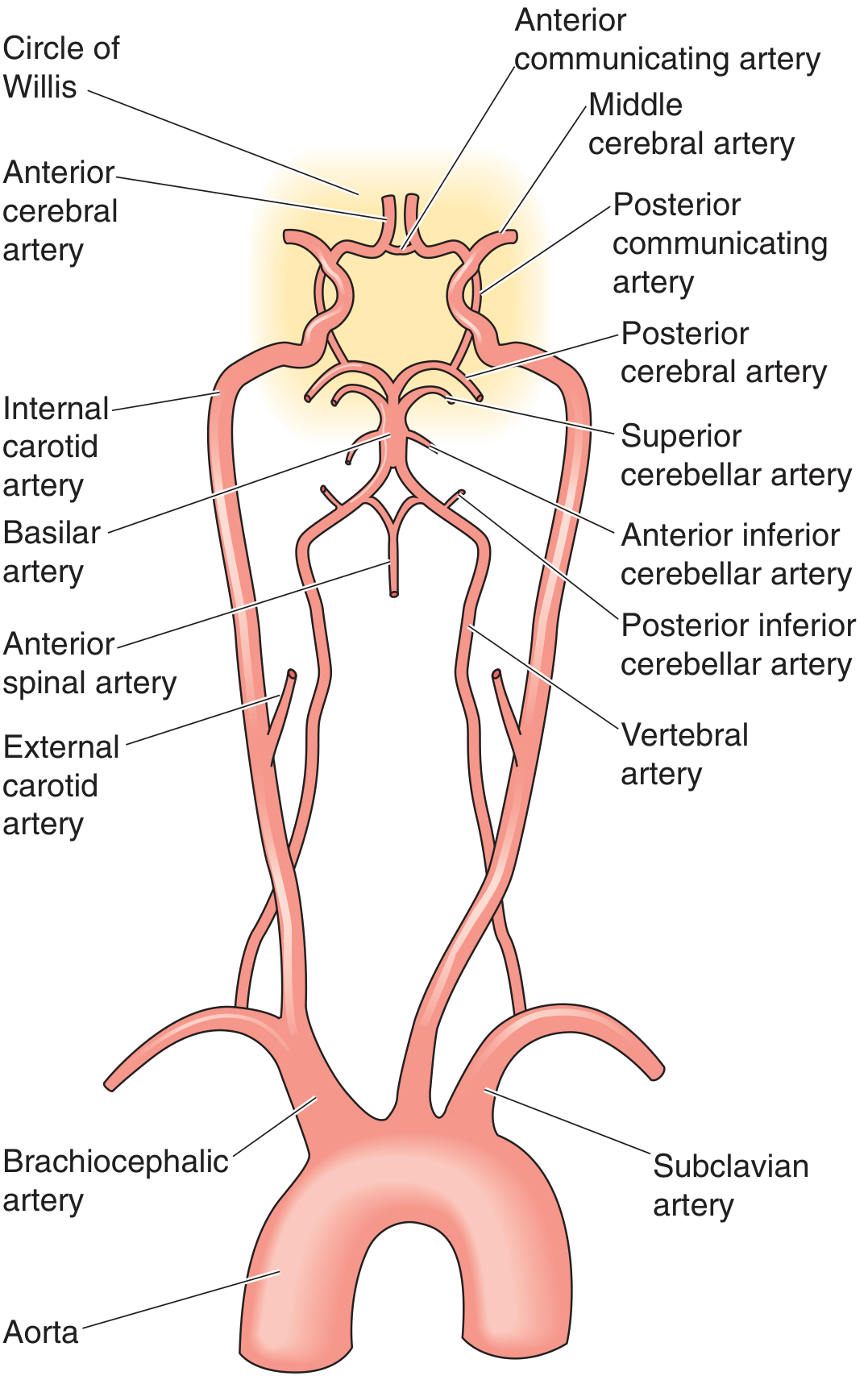
Circle of Willis
Medical Physiology (Boron & Boulpaep) - Major arterial supply and Circle of Willis
Definition
The Circle of Willis is an anastomotic arterial ring at the base of the brain where the anterior circulation (internal carotid arteries) and posterior circulation (vertebrobasilar system) meet and interconnect. It is the origin of all major cerebral arteries and serves as the primary collateral pathway of the brain.
- Neuroanatomy through Clinical Cases, 3rd Ed.; Goldman-Cecil Medicine
Anatomy and Components
The circle is roughly heptagonal in shape and sits on the ventral surface of the brain, at the level of the optic chiasm and hypothalamus. It is formed by the following vessels:
Anterior Circulation (from Internal Carotid Arteries)
| Vessel | Role |
|---|---|
| Internal Carotid Arteries (ICA) | Main inflow vessels; give rise to ACA and MCA |
| Anterior Cerebral Arteries (ACA) | Terminal branches of ICA; run anteriorly |
| Anterior Communicating Artery (AComm) | Connects the two ACAs; bridges the left and right anterior circulations |
| Middle Cerebral Arteries (MCA) | Largest branches of ICA; not technically part of the ring but arise from it |
| Posterior Communicating Arteries (PComm) | Connect the ICA to the posterior cerebral arteries; join anterior and posterior circulations |
Posterior Circulation (from Vertebrobasilar System)
| Vessel | Role |
|---|---|
| Vertebral Arteries | Arise from subclavian arteries; ascend through foramina transversaria of cervical vertebrae |
| Basilar Artery | Formed by fusion of both vertebral arteries at the pontomedullary junction |
| Posterior Cerebral Arteries (PCA) | Terminal branches of the basilar artery; join the PComms to complete the ring |
- Neuroanatomy through Clinical Cases, 3rd Ed., p. 417; Barash Clinical Anesthesia, 9th Ed.
How the Ring Is Completed
Aorta
├── Brachiocephalic → Right Common Carotid → Right ICA ─────┐
└── Left Common Carotid → Left ICA ──────────────────────────┤
├── ACA (left + right)
Subclavian → Vertebral arteries (bilateral) │ └── connected by AComm
└── Basilar artery │
└── Posterior Cerebral Arteries (PCA) ───────────┘
└── connected to ICA via PComm
The basilar artery also gives off the superior cerebellar artery (SCA), anterior inferior cerebellar artery (AICA), and posterior inferior cerebellar artery (PICA) before terminating as the PCAs.
Function - Collateral Circulation
The Circle of Willis provides extensive collateral blood supply. In a person with an intact circle, the entire intracranial circulation can theoretically be supplied by a single patent ICA or vertebral artery.
This is clinically vital: patients with complete occlusion of one carotid artery proximal to the circle may remain asymptomatic if the contralateral circulation can compensate via the communicating arteries.
- Goldman-Cecil Medicine, block 37; Schwartz's Principles of Surgery, 11th Ed.
Completeness and Anatomical Variants
A fully patent, complete Circle of Willis is actually uncommon - present in only approximately 34% of individuals (Neuroanatomy through Clinical Cases) or under 50% (Barash Clinical Anesthesia). Common variants include:
| Variant | Description |
|---|---|
| Hypoplastic/absent A1 segment | The segment of ACA between ICA and AComm is absent; both ACAs fill from one ICA |
| "Fetal" PCA | P1 segment (between basilar and PComm) is absent/hypoplastic; distal PCA territory is supplied by the carotid system rather than vertebrobasilar |
| Hypoplastic PComm | Reduces posterior-anterior collateral capacity |
These variants are highly relevant during neurosurgery, carotid endarterectomy, and when assessing stroke risk. Autopsy studies confirm the majority of specimens show anatomical anomalies.
- Goldman-Cecil Medicine, block 37; Barash Clinical Anesthesia, block 14
Clinical Significance
| Condition | Relevance |
|---|---|
| Ischemic stroke | Collateral flow through the circle determines severity of infarct when a feeding artery is occluded |
| Berry (saccular) aneurysms | Most commonly form at bifurcation points of the circle (e.g., AComm, PComm-ICA junction, MCA bifurcation) - the classic cause of subarachnoid hemorrhage |
| Carotid endarterectomy | If the circle is incomplete, surgeons must monitor for ischemia during carotid clamping |
| Watershed infarcts | Occur at territories between major vessels when perfusion pressure falls |
Berry aneurysms form at these high-pressure bifurcation points due to congenital weakness in the arterial wall media. Rupture causes subarachnoid hemorrhage - classically presenting as the "thunderclap" worst headache of life.
- Robbins & Cotran Pathologic Basis of Disease; Neuroanatomy through Clinical Cases, 3rd Ed.
Territories of the Three Main Cerebral Arteries
| Artery | Territory Supplied |
|---|---|
| ACA | Medial frontal and parietal lobes (leg/foot motor and sensory cortex), anterior corpus callosum |
| MCA | Lateral frontal, parietal, temporal lobes (arm/face motor and sensory, Broca's area, Wernicke's area) - largest territory |
| PCA | Occipital lobes (primary visual cortex), inferior temporal lobe, thalamus, midbrain |
Sources: Neuroanatomy through Clinical Cases, 3rd Ed. | Goldman-Cecil Medicine, International Ed. | Medical Physiology (Boron & Boulpaep) | Barash Clinical Anesthesia, 9th Ed. | Robbins & Cotran Pathologic Basis of Disease
Micturition according to gk pal physiology
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Loading Image
All content and diagrams are in hand. Here is the complete, detailed answer.
Note: GK Pal's Textbook of Medical Physiology is not available in the library. The content below is drawn from Guyton & Hall (the standard global physiology reference most equivalent to GK Pal in depth and style), Ganong's Review, and Boron & Boulpaep Medical Physiology - all covering micturition at the same level of detail as GK Pal.
Micturition (Urination)
Micturition is the process by which the urinary bladder empties when it becomes filled. It involves two main steps:
- Progressive bladder filling until wall tension exceeds a threshold
- The micturition reflex - a nervous reflex that empties the bladder
The reflex is an autonomic spinal cord reflex but is modulated by higher brain centers (cortex and brainstem).
1. Physiological Anatomy of the Bladder
The bladder is a smooth muscle chamber with two parts:
| Part | Description |
|---|---|
| Body | Main reservoir where urine collects |
| Neck (posterior urethra) | Funnel-shaped, 2-3 cm long; connects to urethra; contains the internal sphincter |
Detrusor Muscle
- Smooth muscle making up the bladder wall
- Fibers run in all directions - when contracted, raises intravesical pressure to 40-60 mmHg
- Smooth muscle cells are electrically fused (gap junctions) - action potentials spread cell-to-cell to contract the entire bladder at once
Trigone
- Triangular smooth area on the posterior wall just above the bladder neck
- Apex: opens into the posterior urethra
- Upper two angles: ureteric orifices
- Mucosa is smooth (no rugae, unlike the rest of the bladder)
Sphincters
| Sphincter | Type | Control | Location |
|---|---|---|---|
| Internal sphincter | Smooth muscle (detrusor extension) | Involuntary | Bladder neck |
| External sphincter | Skeletal (voluntary) muscle | Voluntary (pudendal nerve) | Urogenital diaphragm |
2. Innervation of the Bladder
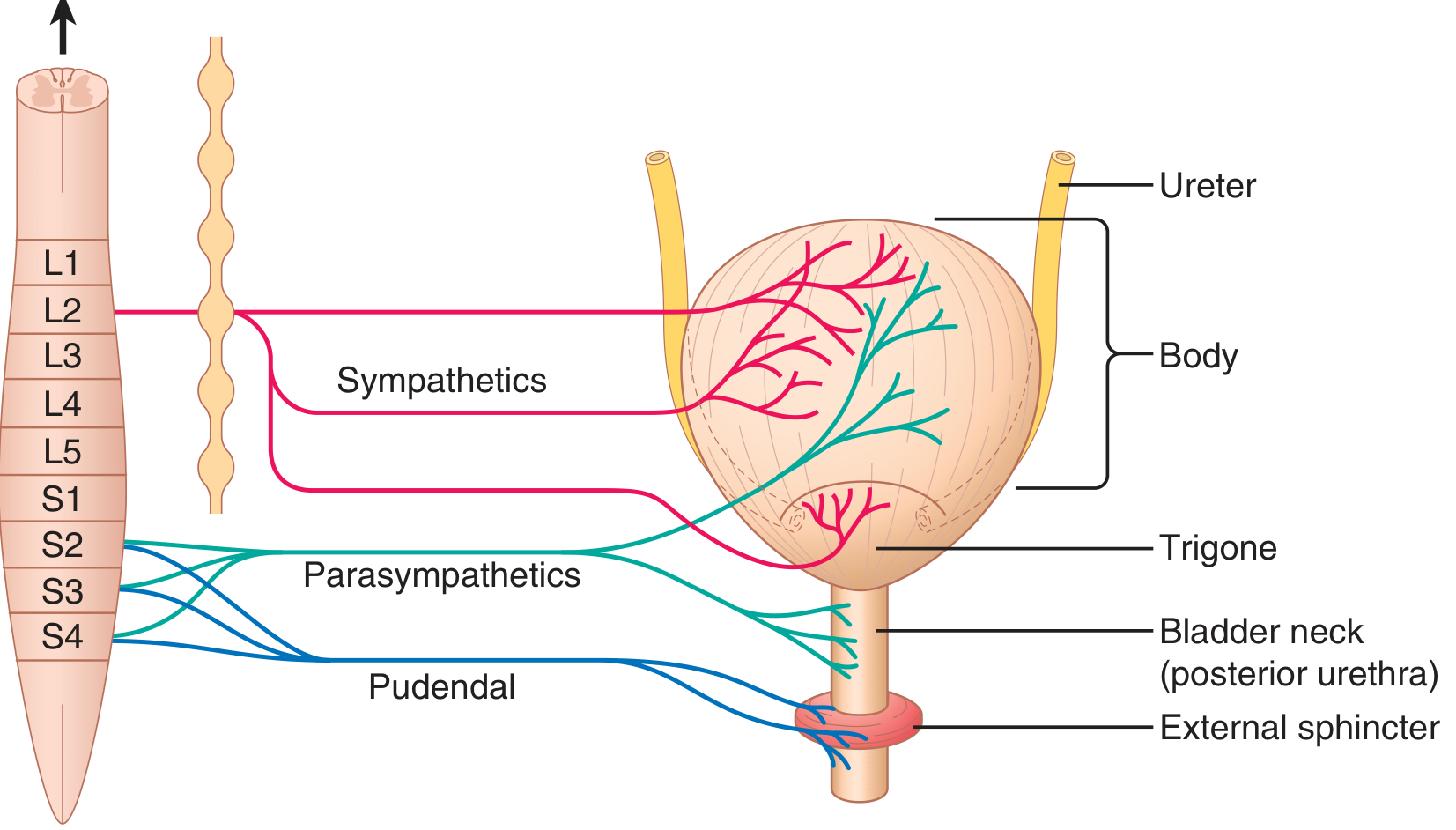
Guyton & Hall - Innervation of the urinary bladder
Three sets of nerves supply the bladder:
A. Pelvic Nerves (Parasympathetic) - S2, S3, S4
- Primary micturition nerves
- Both afferent (sensory, stretch receptors) and efferent (motor) fibers
- Efferents: stimulate detrusor contraction → promotes micturition
- Afferents: carry sensation of bladder fullness and urgency
B. Hypogastric/Sympathetic Nerves - L1, L2, L3 (via inferior mesenteric ganglion)
- Supply blood vessels and facilitate urine storage
- Inhibit detrusor contraction (β-receptors on body)
- Stimulate internal sphincter contraction (α-receptors on neck)
- Sensory fibers via sympathetics may convey fullness and pain in some cases
C. Pudendal Nerves (Somatic) - S2, S3, S4
- Supply the external sphincter (voluntary skeletal muscle)
- Allow conscious control over voiding
- During micturition reflex: inhibitory impulses via pudendal nerves relax the external sphincter
3. The Cystometrogram
A cystometrogram records intravesical pressure vs. bladder volume and has three phases:
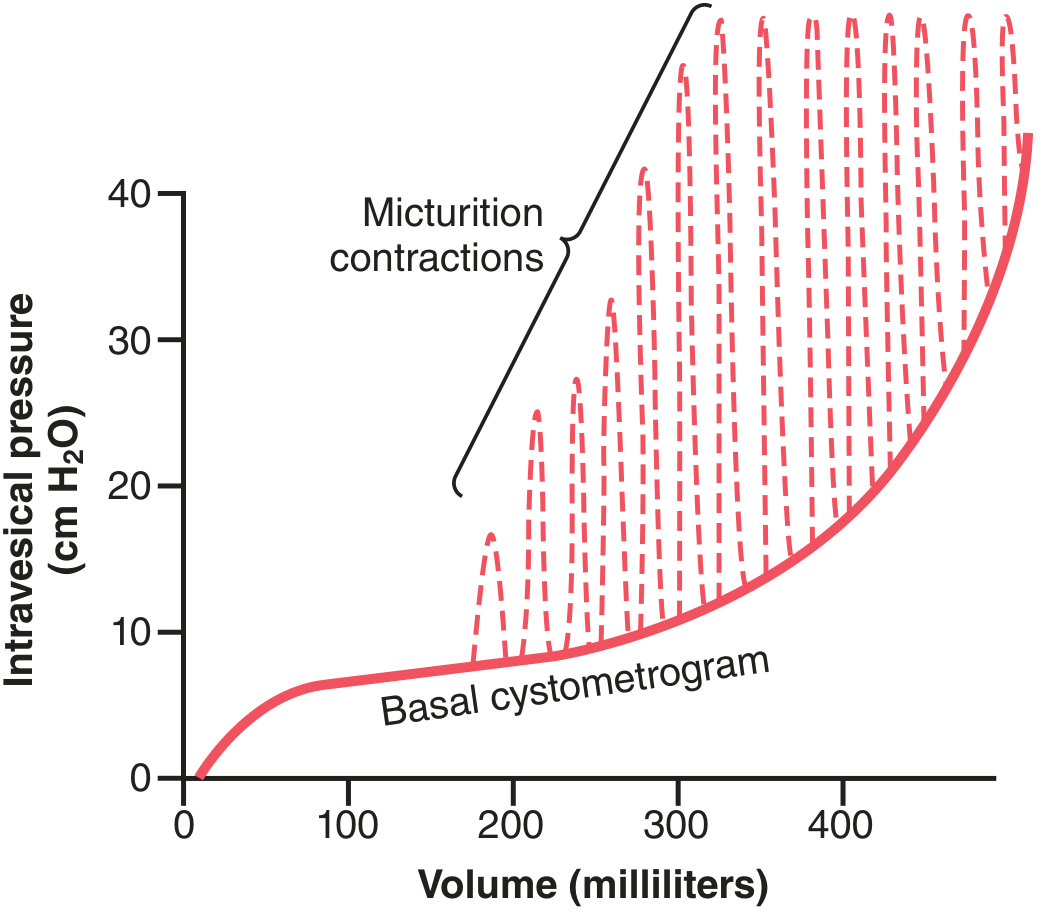
Guyton & Hall - Normal cystometrogram showing micturition waves
| Phase | Volume | Pressure change |
|---|---|---|
| Initial | 0 → ~50 mL | Slight rise in pressure |
| Tonic/Compliance phase | 50 → 300-400 mL | Pressure remains almost constant (high compliance - detrusor accommodates/relaxes) |
| Steep rise | >300-400 mL | Rapid pressure increase; urgency |
Micturition waves (dashed spikes on the graph) = superimposed pressure peaks caused by the micturition reflex firing periodically as the bladder fills. These peaks may rise from a few cmH₂O up to >100 cmH₂O.
Conscious first urge to void is felt at ~150 mL; fullness is felt at 400-500 mL.
4. The Micturition Reflex
Stimulus
As the bladder fills, stretch receptors in the bladder wall (especially in the posterior urethra) are activated when pressure rises above threshold.
Reflex Arc
Stretch receptors in bladder wall
↓ (afferent via pelvic nerves)
Sacral micturition center (S2-S4)
↓ (efferent via pelvic parasympathetics)
Detrusor muscle CONTRACTS
↓
Increased pressure → activates more stretch receptors
↓ (SELF-REGENERATIVE / positive feedback loop)
Stronger contraction → more stretch activation → greater contraction...
↓
Eventual fatigue of reflex → bladder relaxes
Key Feature: Self-Regenerative Nature
Once the micturition reflex starts, it is self-reinforcing:
- Bladder contraction → activates more stretch receptors → stronger sensory signals → stronger reflex contraction → and so on
- This cycle repeats until the bladder reaches maximum contraction
- After a few seconds to 1 minute, the reflex fatigues and the bladder relaxes
One Complete Micturition Reflex Cycle
- Progressive, rapid rise in intravesical pressure
- A period of sustained pressure
- Return of pressure to basal tone (relaxation/fatigue)
If voiding does not occur, the reflex is inhibited for a few minutes to over 1 hour before recurring. As the bladder fills further, reflexes become more frequent and powerful.
5. Facilitation and Inhibition by Higher Centers
The micturition reflex is a spinal reflex but the brain exerts final control:
| Center | Effect |
|---|---|
| Pontine micturition center (PMC) | Coordinates detrusor contraction AND sphincter relaxation; facilitates voiding |
| Cerebral cortex | Primarily inhibitory - keeps the reflex suppressed until a socially appropriate moment |
| Cortex (when voiding desired) | Can switch to facilitatory - initiates reflex and simultaneously inhibits external sphincter |
Normal Voluntary Voiding Sequence
- Cortex removes tonic inhibition of sacral micturition center
- PMC coordinates: parasympathetic activation → detrusor contracts
- Inhibitory signals via pudendal nerves relax the external sphincter
- Small amount of urine reaches posterior urethra → afferents signal cortex that voiding is imminent
- Full detrusor contraction → bladder empties
If voluntary retention is desired: cortex maintains tonic contraction of the external sphincter via pudendal nerves, overriding the reflex - until a suitable time.
6. Abnormalities of Micturition
| Lesion | Bladder Effect |
|---|---|
| Afferent nerve interruption only (sacral dorsal roots) | Flaccid, distended bladder; no reflex contractions; residual urine; wall thins |
| Both afferent + efferent interruption (decentralized bladder) | Initially flaccid; later small uncoordinated contractions; dribbling; hypertrophied small bladder |
| Spinal cord transection (above sacral center) | Spinal shock phase: overflow incontinence; After shock: voiding reflex returns but no voluntary control → spastic neurogenic bladder (reduced capacity, hypertrophied wall, reflex hyperactivity) |
| Brain lesions (above pons) | Loss of cortical inhibition → urge incontinence; reflex voiding at low volumes |
Summary Diagram
FILLING PHASE VOIDING PHASE
─────────────────────────────────────────────────────────
Bladder fills → stretch receptors Cortex permits voiding
↓ ↓
Afferents → sacral cord (S2-S4) Removes inhibition
↓ ↓
Signal ascends to cortex PMC coordinates:
(urge sensation at ~150 mL) • Detrusor contracts (parasympathetic)
↓ • Internal sphincter opens
Cortex INHIBITS voiding • External sphincter relaxes (pudendal)
(tonic suppression) ↓
↓ Urine → posterior urethra
Bladder continues to fill → self-regenerative reflex → full void
Sources: Guyton and Hall Textbook of Medical Physiology | Ganong's Review of Medical Physiology, 26th Ed. | Medical Physiology (Boron & Boulpaep)
What are the differences between spastic vs. flaccid neurogenic bladder?
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Femoral triangle with diagram
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
All diagrams and content are in hand. Here is the comprehensive answer:
Femoral Triangle
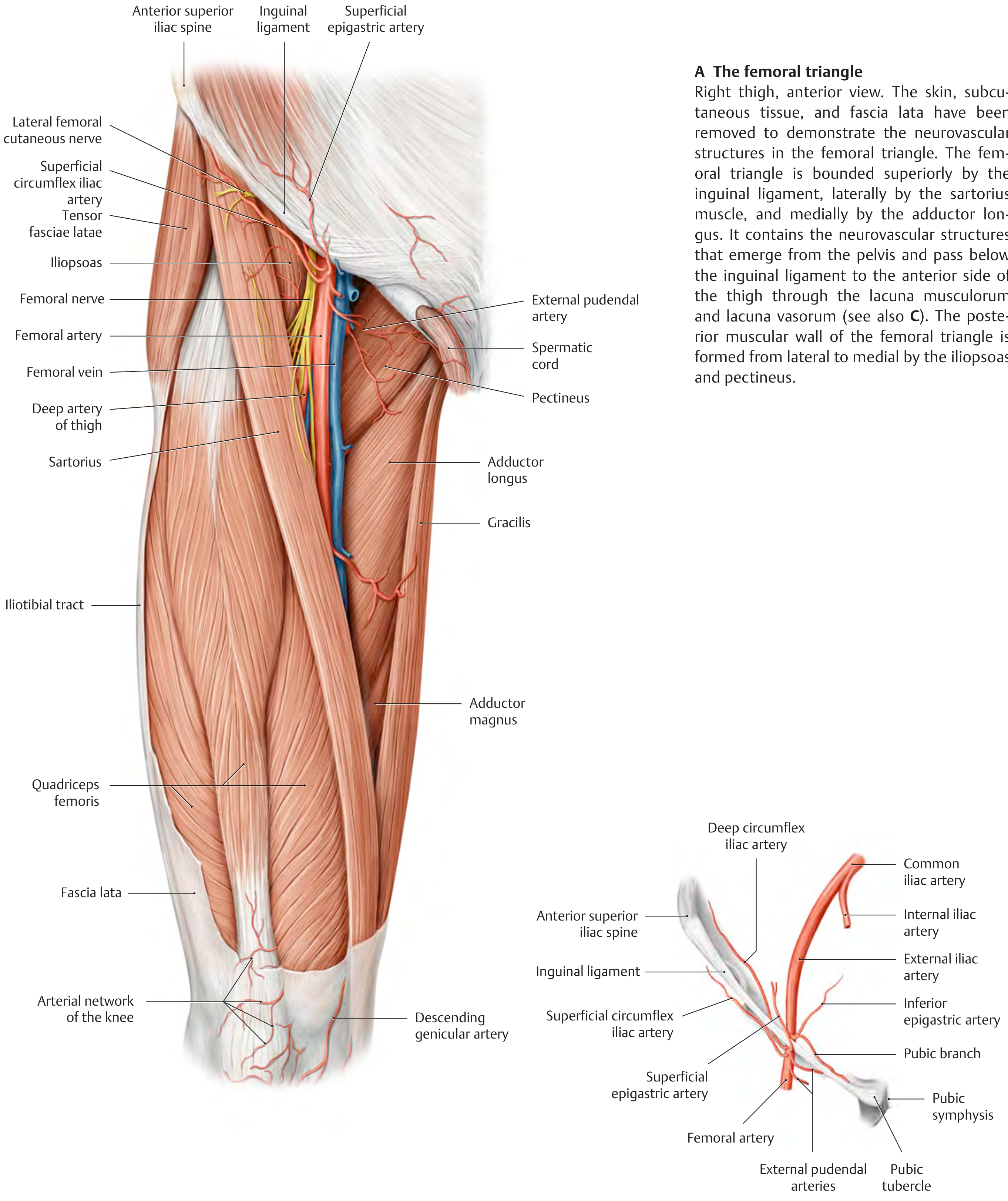
Overview
The femoral triangle is a wedge-shaped (triangular) subfascial depression in the upper anterior thigh, at the junction between the anterior abdominal wall and the lower limb. It acts as a conduit for major neurovascular structures passing from the abdomen into the lower extremity.
Boundaries
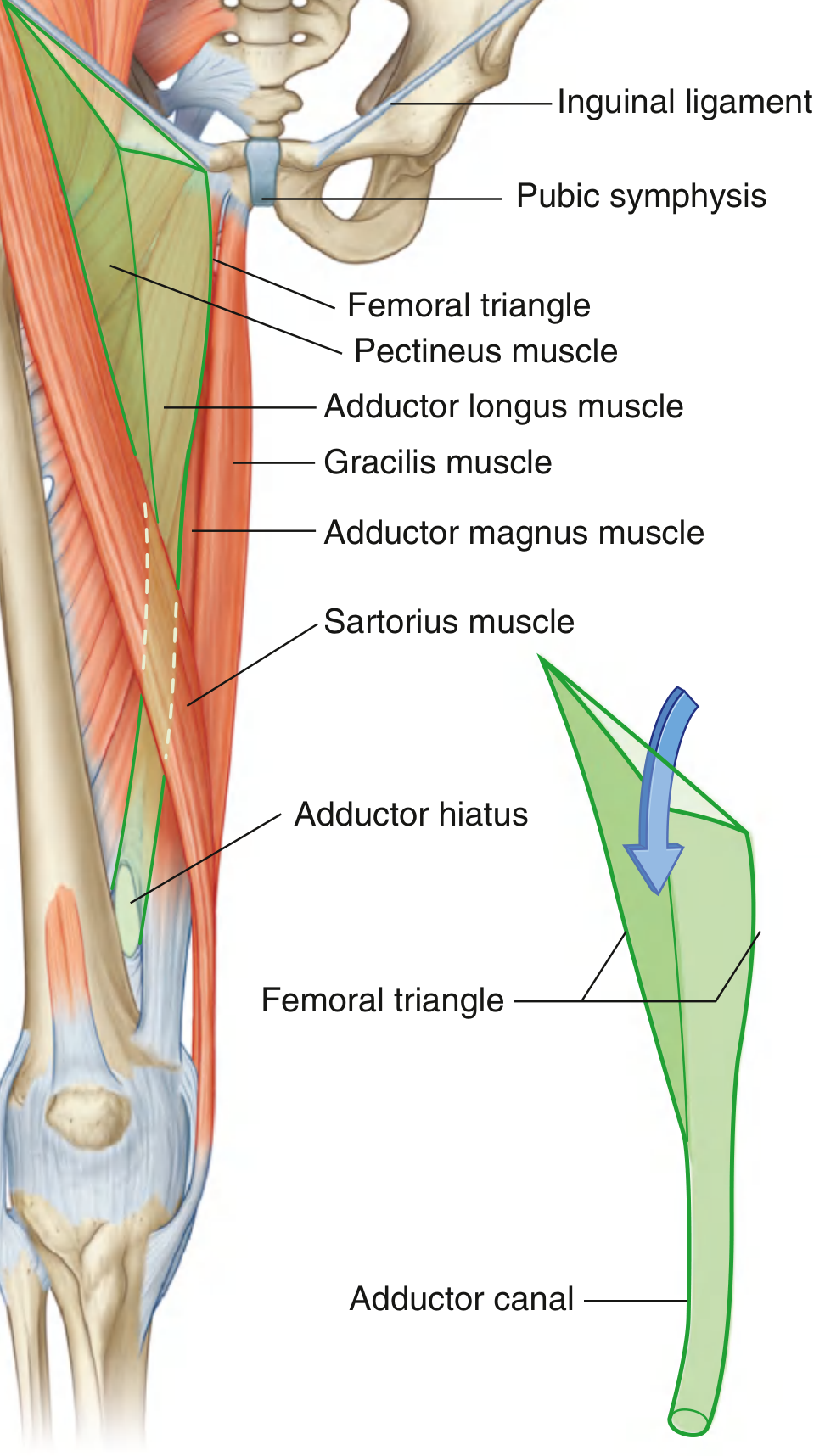
Fig. 6.42 - Boundaries of the Femoral Triangle (Gray's Anatomy for Students)
| Border | Structure |
|---|---|
| Base (superior) | Inguinal ligament (runs from ASIS laterally to pubic tubercle medially) |
| Lateral border | Medial margin of sartorius muscle |
| Medial border | Medial margin of adductor longus muscle |
| Apex | Points inferiorly - where sartorius and adductor longus converge; continuous with the adductor canal |
Floor (posterior wall)
Formed by two muscles, from lateral to medial:
- Iliopsoas (lateral part of the floor)
- Pectineus (medial part of the floor)
- Adductor longus also contributes at the medial aspect
Roof (anterior wall)
- Fascia lata (deep fascia of the thigh) - forms the roof
- Covered by skin and subcutaneous tissue
Contents
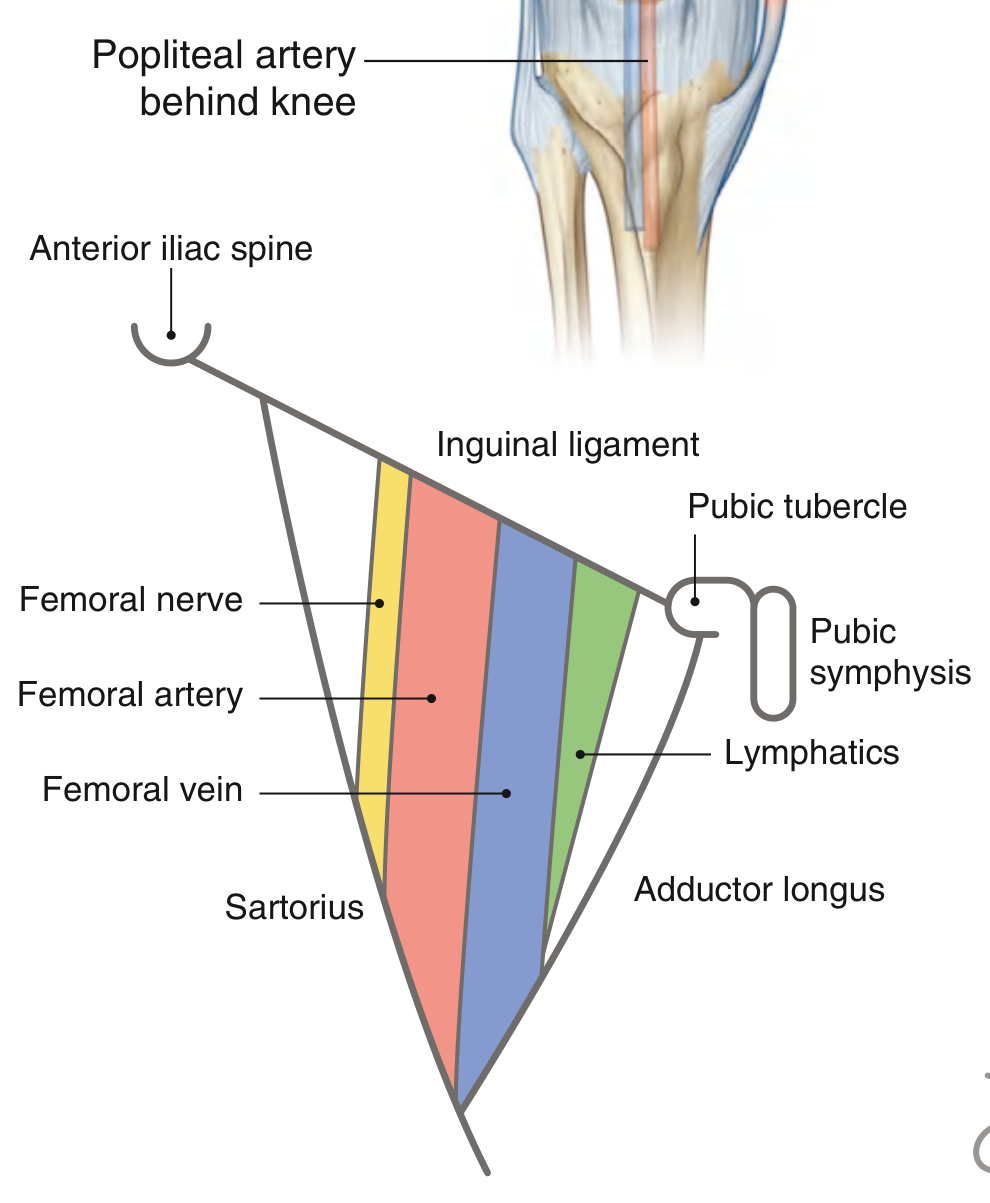
Fig. 6.43 - Contents of the Femoral Triangle (Gray's Anatomy for Students)
From lateral to medial (mnemonic: NAVY - Nerve, Artery, Vein, Y-fronts/lymphatics):
| Structure | Position | Notes |
|---|---|---|
| Femoral Nerve | Most lateral | Outside the femoral sheath; divides into anterior and posterior divisions shortly after entry |
| Femoral Artery | Middle | Palpable just below inguinal ligament, midway between ASIS and pubic symphysis |
| Femoral Vein | Medial to artery | Receives the great saphenous vein at the saphenous opening |
| Lymphatics / Femoral canal | Most medial | Within the femoral sheath; contains deep inguinal lymph nodes |
Key clinical landmark: The femoral artery pulse is felt midway between the anterior superior iliac spine (ASIS) and the pubic symphysis, just inferior to the inguinal ligament.
Femoral Sheath
THIEME Atlas of Anatomy - Femoral triangle contents, right thigh anterior view
The femoral artery, vein, and lymphatics are enclosed in a funnel-shaped fascial sleeve called the femoral sheath:
- Continuous superiorly with transversalis fascia and iliac fascia of the abdomen
- Divided into 3 compartments:
| Compartment | Position | Contents |
|---|---|---|
| Lateral | Lateral | Femoral artery |
| Intermediate | Middle | Femoral vein |
| Femoral canal | Most medial | Lymphatics + deep inguinal lymph node (Cloquet's / Rosenmüller node) |
Important: The femoral nerve is NOT enclosed within the femoral sheath - it lies lateral to it.
The femoral ring = the superior opening of the femoral canal. It is a potential weak point and is the site of femoral hernias.
Apex and Continuation - Adductor Canal
The apex of the femoral triangle is continuous inferiorly with the adductor canal (Hunter's canal / subsartorial canal), which:
- Descends medially down the thigh under sartorius
- Transmits the femoral artery and vein (and saphenous nerve)
- Opens posteriorly via the adductor hiatus in adductor magnus → vessels emerge as the popliteal artery and vein behind the knee
Summary Diagram (Schematic)
ASIS ──────────────────── Pubic tubercle
\ INGUINAL LIGAMENT /
\ (BASE) /
\ /
Sartorius \ / Adductor longus
(lateral) \ / (medial)
\ /
\ APEX /
↓
Adductor canal → Adductor hiatus → Popliteal fossa
FLOOR: Iliopsoas (lateral) + Pectineus (medial)
ROOF: Fascia lata
CONTENTS (lateral → medial):
[Femoral Nerve] | [Femoral Artery] | [Femoral Vein] | [Lymphatics]
←─── Femoral Sheath covers A, V, Lymph ───→
Clinical Significance
| Application | Detail |
|---|---|
| Femoral pulse palpation | Standard landmark for peripheral vascular exam - midpoint of inguinal ligament |
| Femoral artery cannulation | Used for cardiac catheterization, coronary angiography, angioplasty; access to aorta and cerebral vessels |
| Femoral vein cannulation | Access to right heart, pulmonary artery, renal veins, gonadal veins, IVC |
| Femoral hernia | Protrusion through the femoral ring (femoral canal); more common in women; lies below and lateral to the pubic tubercle (vs. inguinal hernia which is above and medial) |
| Femoral artery aneurysm / pseudoaneurysm | Complication of femoral arterial access procedures |
| Lymphadenopathy | Enlarged deep inguinal nodes palpable in the femoral triangle in lower limb/perineal infections or malignancies |
Sources: Gray's Anatomy for Students | THIEME Atlas of General Anatomy and Musculoskeletal System
Give popliteal fossa acc to bd Chaurasia
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
All content and diagrams retrieved. Here is the full answer:
Note: BD Chaurasia's Human Anatomy is not available in the library. The content below is drawn from Gray's Anatomy for Students and the THIEME Atlas of Anatomy - both standard regional anatomy references that cover the popliteal fossa in the same depth and format as BD Chaurasia.
Popliteal Fossa
Definition
The popliteal fossa is a diamond-shaped space (fossa) situated behind the knee joint. It is the major transitional region between the posterior thigh and the posterior leg, serving as the primary route through which neurovascular structures pass from one region to the other.
Shape
Diamond-shaped (rhomboidal), with:
- A wider upper half (between hamstring muscles)
- A narrower lower half (between gastrocnemius heads)
Boundaries
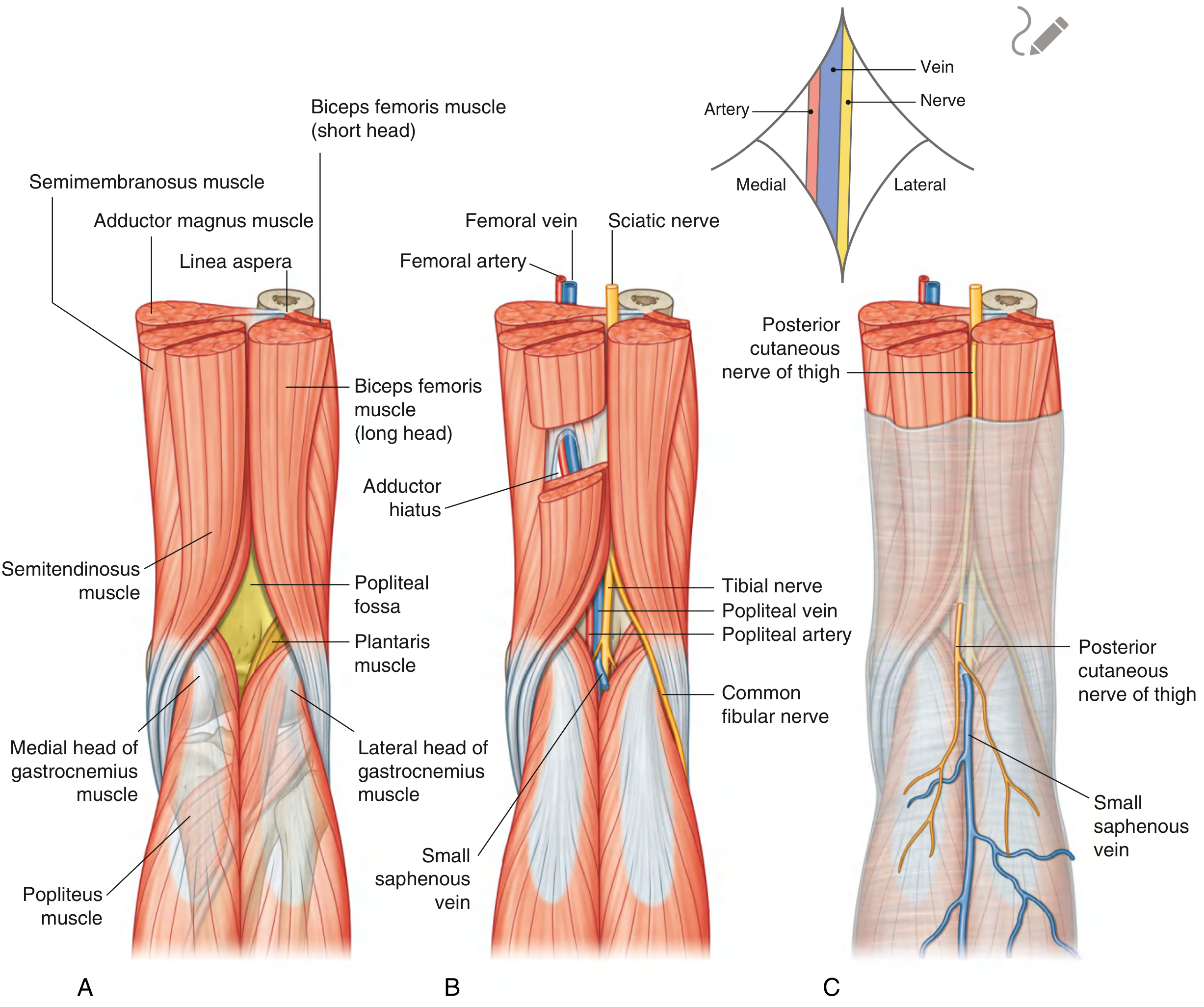
Fig. 6.85 - Popliteal Fossa: A) Boundaries, B) Contents, C) Superficial structures (Gray's Anatomy for Students)
Upper (Superomedial and Superolateral) Angles
| Border | Muscle |
|---|---|
| Superomedial | Semitendinosus + Semimembranosus |
| Superolateral | Biceps femoris (long and short heads) |
Lower (Inferomedial and Inferolateral) Angles
| Border | Muscle |
|---|---|
| Inferomedial | Medial head of gastrocnemius |
| Inferolateral | Lateral head of gastrocnemius + Plantaris |
Floor (Anterior Wall)
From above downward:
- Popliteal surface of the femur (lower end)
- Posterior capsule of the knee joint (including oblique popliteal ligament)
- Popliteus muscle (lower part of floor)
Roof (Posterior Wall)
- Deep fascia (popliteal fascia) - thick, perforated by the small saphenous vein and posterior cutaneous nerve of the thigh
- Continuous superiorly with fascia lata; inferiorly with deep fascia of the leg
- Overlying skin and superficial fascia
Contents
The major neurovascular structures pass through the popliteal fossa from deep (anterior) to superficial (posterior):
Deepest to Most Superficial Order:
DEEPEST → Popliteal Artery
↓
Popliteal Vein
↓
Tibial Nerve
↓
MOST Common Fibular (Peroneal) Nerve
SUPERFICIAL
Plus: small saphenous vein, posterior cutaneous nerve of thigh, popliteal lymph nodes, fat
1. Popliteal Artery
- Deepest structure in the fossa (hardest to palpate)
- Continuation of the femoral artery after it passes through the adductor hiatus in adductor magnus
- Enters the fossa from the upper medial side (under semimembranosus)
- Descends obliquely to exit below the popliteus, where it divides into:
- Anterior tibial artery (passes through interosseous membrane to anterior compartment)
- Posterior tibial artery (continues in posterior leg)
Branches within the fossa:
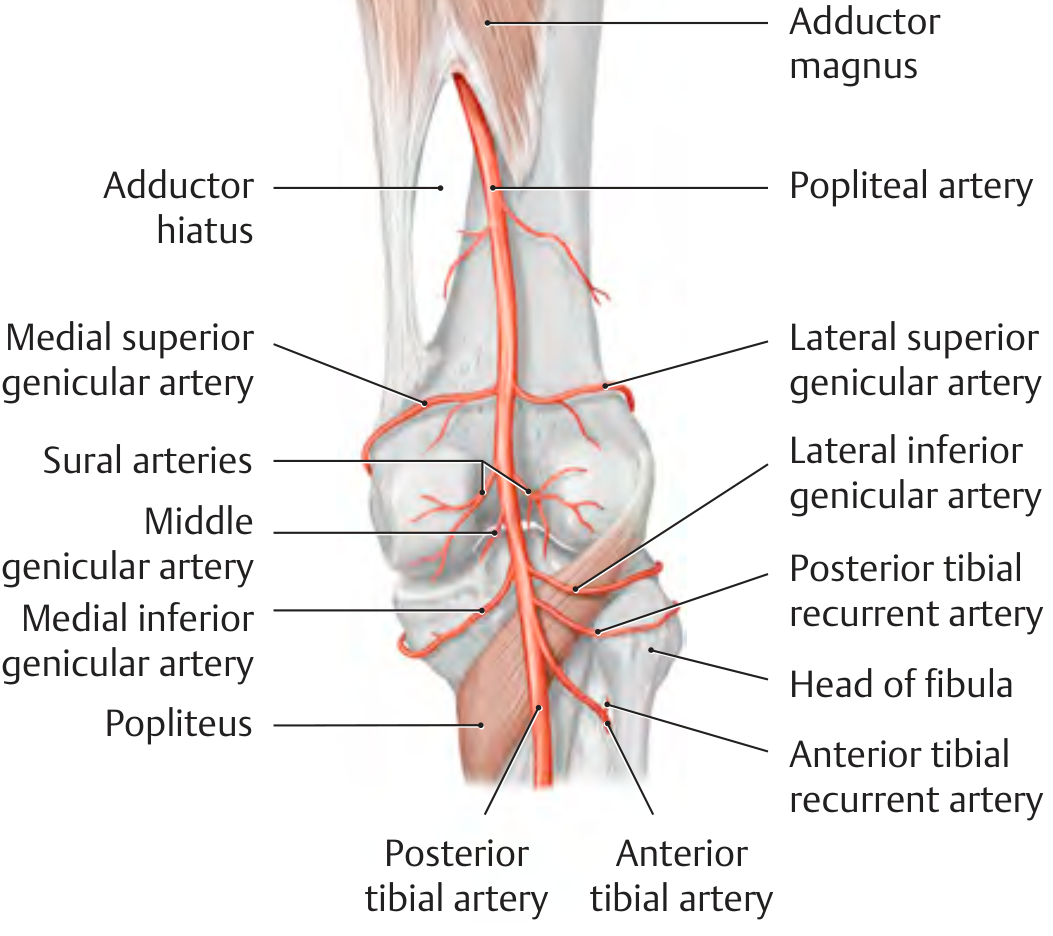
THIEME Atlas of Anatomy - Branches of the popliteal artery
| Branch | Notes |
|---|---|
| Medial superior genicular artery | Runs above medial condyle |
| Lateral superior genicular artery | Runs above lateral condyle |
| Middle genicular artery | Pierces posterior capsule; supplies cruciate ligaments and synovial membrane |
| Medial inferior genicular artery | Runs below medial condyle |
| Lateral inferior genicular artery | Runs below lateral condyle |
| Sural arteries (paired) | Supply gastrocnemius heads |
All genicular arteries (except middle) form the periarticular anastomosis (articular rete) of the knee - the collateral circulation around the knee joint.
2. Popliteal Vein
- Superficial to the popliteal artery
- Formed by the union of the anterior and posterior tibial veins at the lower border of the popliteus
- Exits the fossa superiorly through the adductor hiatus to become the femoral vein
- Receives the small saphenous vein which pierces the roof of the fossa
3. Tibial Nerve
- Branch of the sciatic nerve (L4, L5, S1, S2, S3)
- Most superficial of the deep neurovascular structures
- Descends vertically through the midline of the popliteal fossa
- Exits deep to the arch of the soleus (soleal arch) to enter the posterior compartment of the leg
- Branches in the fossa:
- Muscular branches to gastrocnemius, plantaris, soleus, popliteus
- Sural nerve (cutaneous - joins sural communicating branch of common fibular nerve to form the sural nerve proper)
4. Common Fibular (Peroneal) Nerve
- Branch of the sciatic nerve (L4, L5, S1, S2)
- Descends along the medial border of biceps femoris
- Exits the fossa at the superolateral angle by following the biceps femoris tendon
- Winds around the neck of the fibula to enter the lateral compartment
- Most vulnerable nerve in the fossa - easily injured at fibular neck (foot drop)
- Branches in the fossa:
- Lateral sural cutaneous nerve (skin of upper lateral leg)
- Sural communicating nerve
- Articular branches to the knee
5. Superficial Contents (in the roof/superficial fascia)
| Structure | Detail |
|---|---|
| Small (short/lesser) saphenous vein | Ascends from lateral foot, pierces popliteal fascia to join popliteal vein |
| Posterior cutaneous nerve of thigh | Descends superficial to hamstrings through roof; supplies skin of upper back of leg |
| Popliteal lymph nodes (6 nodes) | Embedded in fat; drain the leg, knee, and deep structures; drain to deep inguinal nodes |
| Fat | Fills the fossa; embeds all structures |
Relations - Structures Entering/Leaving
| Structure | Entry | Exit |
|---|---|---|
| Femoral artery → Popliteal artery | Through adductor hiatus (upper medial) | Divides at lower border of popliteus |
| Popliteal vein | Formed below popliteus | Through adductor hiatus → femoral vein |
| Sciatic nerve | Divides at apex above fossa | As tibial + common fibular nerves |
| Small saphenous vein | Pierces roof from posterior leg | Joins popliteal vein |
Summary Table
| Feature | Detail |
|---|---|
| Shape | Diamond (rhombus) |
| Superomedial border | Semitendinosus + semimembranosus |
| Superolateral border | Biceps femoris |
| Inferomedial border | Medial head of gastrocnemius |
| Inferolateral border | Lateral head of gastrocnemius + plantaris |
| Floor | Femur → knee joint capsule → popliteus |
| Roof | Deep fascia (popliteal fascia) |
| Deepest content | Popliteal artery |
| Most superficial deep content | Common fibular nerve (then tibial nerve) |
| Nerve at lateral exit | Common fibular nerve (around fibular neck) |
Clinical Significance
| Condition | Notes |
|---|---|
| Baker's cyst (popliteal cyst) | Distension of the gastrocnemio-semimembranosus bursa (communicates with knee joint); presents as posterior knee swelling; associated with knee OA or RA |
| Popliteal artery aneurysm | Most common peripheral artery aneurysm; risk of distal embolization and limb ischemia; often associated with aortic/femoral aneurysms; diagnosed by duplex ultrasound |
| Common fibular nerve injury | At fibular neck (lateral exit from fossa); causes foot drop (loss of dorsiflexion + eversion) and sensory loss over anterolateral leg + dorsum of foot |
| Popliteal pulse | Difficult to palpate (deepest structure); knee slightly flexed, deep pressure just medial to midline |
| Popliteal lymphadenopathy | Infection/malignancy of the leg, knee, foot |
Sources: Gray's Anatomy for Students | THIEME Atlas of General Anatomy and Musculoskeletal System
Is deltoid ligament part of ankle joint
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
All the content needed is in hand. Here is the complete answer:
Is the Deltoid Ligament Part of the Ankle Joint?
Yes - the deltoid ligament IS part of the ankle joint. It is the medial collateral ligament (MCL) of the ankle joint (talocrural joint), forming the entire medial reinforcement of the joint capsule.
What is the Deltoid Ligament?
The deltoid ligament (from Greek deltoeides = triangular/delta-shaped) is a strong, thick, fan-shaped or triangular ligament on the medial side of the ankle, arising from the medial malleolus of the tibia and fanning out to attach to multiple tarsal bones below.
It is the primary stabilizer of the ankle during the stance phase of walking and is considerably stronger than the lateral ankle ligaments - which is why isolated deltoid tears are far less common than lateral ankle sprains.
Structure - Two Layers
The deltoid ligament is classically divided into a superficial and a deep layer:
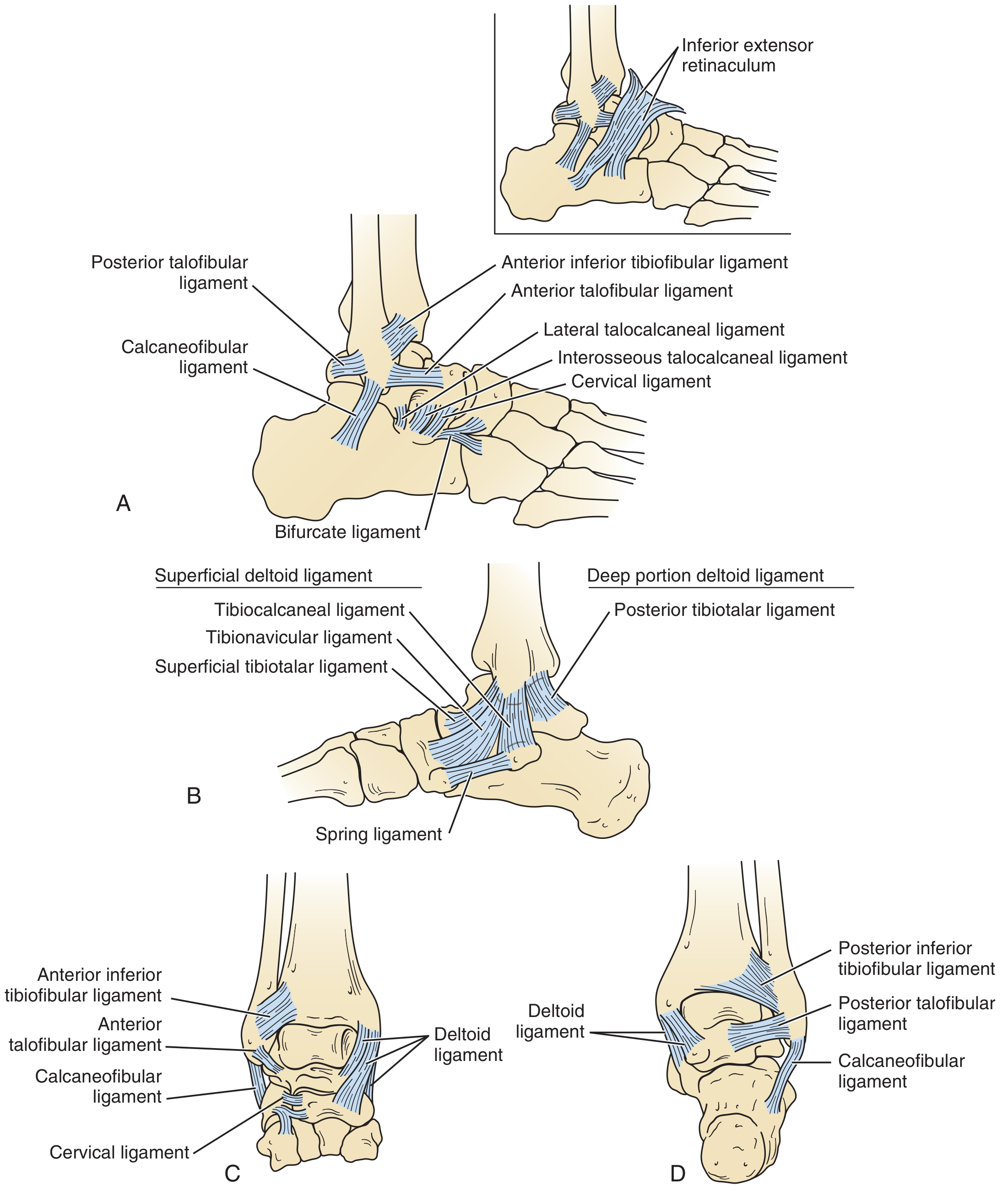
Ligaments of the Ankle - (A) Lateral, (B) Medial showing deltoid, (C) Anterior, (D) Posterior views
Superficial Layer
Arises from the anterior colliculus (distal surface) of the medial malleolus. It bridges both the talocrural (ankle) joint AND the subtalar joint. Consists of four components:
| Component | Origin | Insertion |
|---|---|---|
| Tibionavicular ligament | Anterior colliculus of medial malleolus | Dorsomedial aspect of navicular bone |
| Tibiospring (tibiocalcaneonavicular) ligament | Medial malleolus | Upper border of spring (plantar calcaneonavicular) ligament |
| Tibiocalcaneal ligament | Medial malleolus | Sustentaculum tali of calcaneus |
| Superficial posterior tibiotalar ligament | Medial malleolus | Medial talus (posterior) |
Function: Primarily resists valgus/eversion forces (talar tilt) at the ankle.
Deep Layer
Arises from the apex (intercollicular groove) of the medial malleolus. It is the stronger, shorter layer and bridges only the talocrural (ankle) joint - NOT the subtalar joint. Consists of:
| Component | Origin | Insertion |
|---|---|---|
| Deep anterior tibiotalar ligament | Medial malleolus (intercollicular groove) | Anterior medial surface of talar body |
| Deep posterior tibiotalar ligament | Medial malleolus (intercollicular groove) | Posterior medial surface of talar body |
Function: Primarily resists lateral talar translation and external rotation of the talus. The posterior deep deltoid is the most functionally important component.
- Miller's Review of Orthopaedics, 9th Ed.; Imaging Anatomy (THIEME), Vol. 3
Summary Table
| Feature | Detail |
|---|---|
| Also called | Medial collateral ligament of the ankle |
| Shape | Fan-shaped / deltoid (triangular) |
| Proximal attachment | Medial malleolus (tibia) |
| Distal attachments | Talus, navicular, calcaneus (sustentaculum tali), spring ligament |
| Layers | Superficial (4 bands) + Deep (2 bands) |
| Deep layer bridges | Talocrural joint only |
| Superficial layer bridges | Talocrural + subtalar joints |
| Primary function | Resist eversion, lateral talar translation, external rotation |
| Injury mechanism | Eversion / forced external rotation (opposite of the more common lateral sprain) |
Relationship to Adjacent Structures
The deltoid ligament has a special relationship with the spring (plantar calcaneonavicular) ligament - the tibiospring component of the superficial deltoid blends directly into the spring ligament, forming the medial ankle ligament complex together. This complex is important in supporting the medial longitudinal arch and is commonly disrupted in adult-acquired flatfoot deformity (AAFD).
Clinical Relevance
| Condition | Notes |
|---|---|
| Deltoid ligament tear | Usually from eversion injury; often occurs alongside lateral malleolus fracture (bimalleolar-equivalent); isolated tear is uncommon |
| Widened medial clear space on X-ray | >4 mm gap between medial malleolus and talus = deltoid rupture until proven otherwise |
| Ankle mortise instability | Intact deltoid prevents lateral talar shift; rupture allows widening of mortise |
| Adult-acquired flatfoot | Attenuation of deltoid + spring ligament → medial arch collapse |
| Maisonneuve fracture | High fibular fracture + deltoid tear → unstable ankle despite minimal bony deformity at mortise |
Sources: Imaging Anatomy, Vol. 3 - Bones, Joints, Vessels & Nerves (THIEME Atlas) | Miller's Review of Orthopaedics, 9th Ed. | Campbell's Operative Orthopaedics, 15th Ed. 2026
This is a shared conversation. Sign in to Orris to start your own chat.