89 y/o presenting with lethargy , weakness , retching and vomiting with a low sodium of 123 in blood tests , not improving much with normal saline IV fluids and ondansetron. What can be the differentials and treatment modalities
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
hyponatremia elderly management treatment
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
I now have all the information needed to write a thorough, well-cited clinical response. Let me compose it.
This is a classic presentation of severe symptomatic hyponatremia (Na 123 mEq/L) in an elderly patient, and the fact that normal saline is not improving the picture is a critical clue - it strongly points toward a euvolemic cause (especially SIADH), where normal saline can paradoxically worsen the sodium by providing free water that gets retained.
Diagnostic Approach - Start Here
The first step is to classify the hyponatremia using plasma osmolality and volume status assessment:
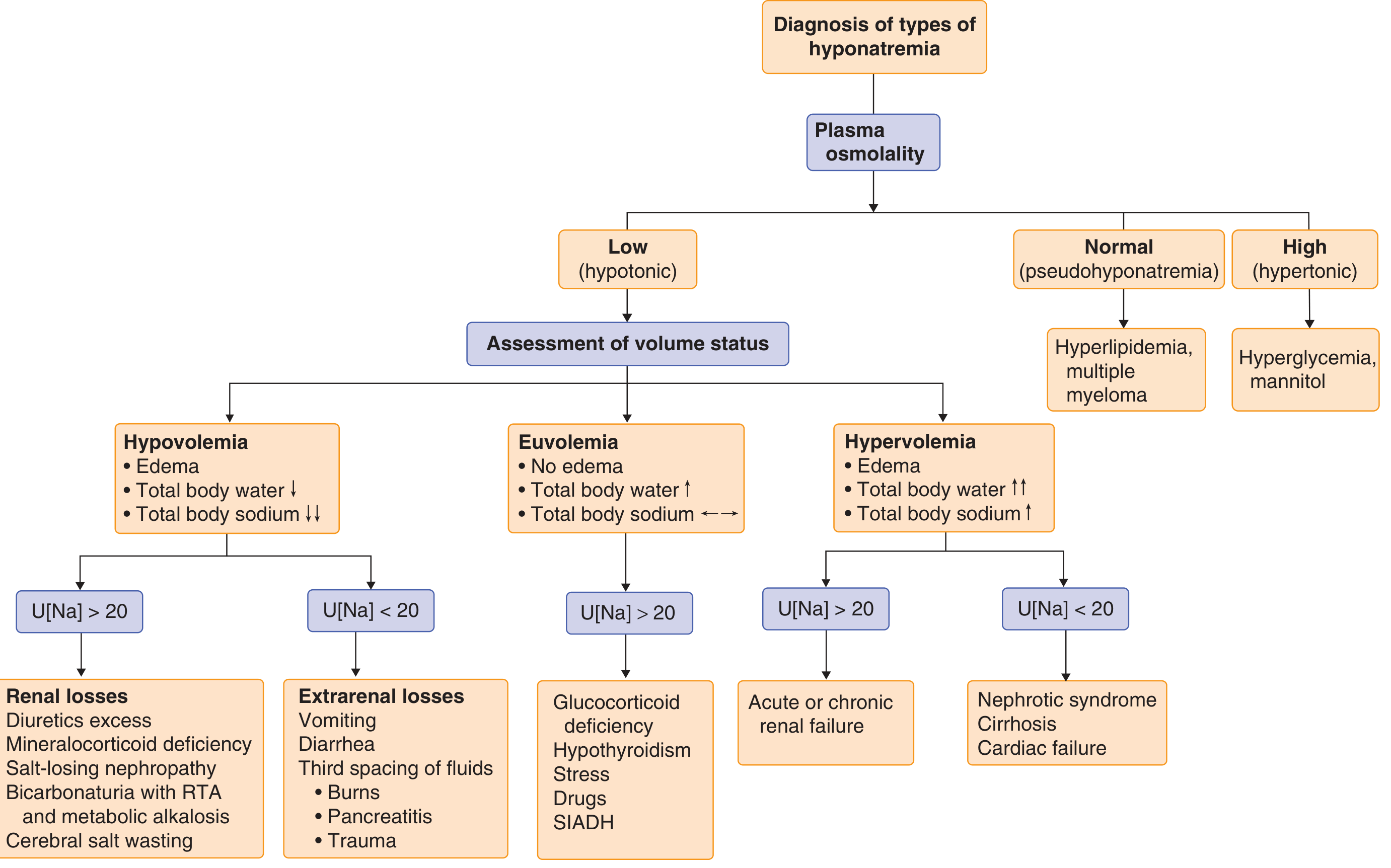
Diagnostic approach to hyponatremia - Goldman-Cecil Medicine
Key diagnostic workup to order now:
| Test | Why it matters |
|---|---|
| Serum osmolality | Confirm true hypotonic hyponatremia (expected <275 mOsm/kg) |
| Urine osmolality | >200 mOsm/kg despite hyponatremia = ADH activity present |
| Urine sodium (spot) | >40 mmol/L = SIADH or adrenal insufficiency; <20 = hypovolemia or extrarenal losses |
| Serum glucose | Exclude hyperglycemic dilutional hyponatremia |
| TSH, Free T4 | Hypothyroidism mimics SIADH |
| Short Synacthen / morning cortisol | Adrenal insufficiency - do not miss in the elderly |
| Serum urea, creatinine | Renal failure; low urea supports SIADH |
| Serum uric acid | Low uric acid strongly supports SIADH |
| LFTs, serum albumin | Cirrhosis/hepatic cause |
| BNP / echocardiogram | Heart failure |
| Serum K+, chloride | Hypokalemia worsens ODS risk; chloride for acid-base |
Differentials
At Na 123 mEq/L with nausea/vomiting, lethargy, and no improvement on normal saline, the differentials ranked by probability in a geriatric patient are:
1. SIADH (most likely euvolemic cause)
The failure of normal saline to correct is the hallmark - in SIADH, infused normal saline (154 mmol/L Na) gets retained as the kidneys excrete hypertonic urine (>154 mOsm), causing net water retention and worsening the sodium. Common causes in the elderly include:
- Pulmonary: pneumonia, lung cancer, COPD exacerbation
- CNS: stroke, subdural haematoma, meningitis (lethargy should prompt head imaging)
- Malignancy: small cell lung cancer is the classic
- Drugs: SSRIs, carbamazepine, chlorpropamide, opioids, diuretics, barbiturates, tricyclics
- Post-operative state
2. Adrenal Insufficiency (must exclude)
Glucocorticoid deficiency causes hyponatremia that can be indistinguishable from SIADH clinically - euvolemic picture, high urine sodium. Associated features include lethargy, weakness, nausea, vomiting, hypotension, hypoglycaemia, eosinophilia. In the elderly, secondary adrenal insufficiency from long-term steroid use (or recent discontinuation) is common. This is a treatable emergency. - Goldman-Cecil Medicine
3. Hypothyroidism / Myxoedema
Severe hypothyroidism impairs free water excretion and also mimics SIADH. Presents with lethargy, weakness, oedema, bradycardia, constipation. TSH will be grossly elevated. Treatment with IV levothyroxine gradually corrects sodium. - Goodman & Gilman's
4. Hypovolemic Hyponatremia (extrarenal losses)
Vomiting itself causes GI sodium losses - but in true hypovolemia you would expect urine Na <20 mmol/L and the patient should respond to normal saline. The failure to respond here argues against this being the primary mechanism, unless the patient is also on thiazide diuretics.
5. Thiazide-Induced Hyponatremia
Extremely common in elderly. Thiazides impair urinary dilution (blocking the diluting segment in the DCT) without affecting medullary concentration. Can cause profound hyponatremia even with modest fluid intake. Urine sodium will be elevated. Stop the thiazide immediately if present.
6. Hypervolemic Hyponatremia
Heart failure, hepatic cirrhosis, or nephrotic syndrome cause water retention exceeding sodium retention. These are usually clinically obvious (oedema, ascites, elevated JVP, raised BNP). Urine Na typically <20 mmol/L.
7. Cerebral Salt Wasting
If there is any CNS pathology (stroke, SAH, head injury) - cerebral salt wasting produces a hypovolemic hyponatremia with paradoxically high urine sodium due to inappropriate renal sodium wasting. Differentiating from SIADH requires measuring blood volume and fractional excretion of urate (high only in CSW).
8. Consider in Elderly Specifically
- Beer potomania / tea-and-toast syndrome - low solute intake impairs free water excretion even with low ADH
- Psychogenic polydipsia - less likely at 89 but worth asking
- Occult malignancy with paraneoplastic SIADH
Why Normal Saline is Failing (and Why it Can Make SIADH Worse)
In SIADH, the urine is concentrated (high osmolality). When you infuse normal saline (308 mOsm/L), the kidneys excrete that sodium in a smaller volume of concentrated urine (e.g., urine osmolality 600 mOsm/kg). The net result is a negative free water clearance - the patient retains water and the serum sodium can fall further. This is well established and warns against relying on normal saline when SIADH is suspected. - Rosen's Emergency Medicine
Treatment Modalities
Step 1 - Establish acuity: Is this acute (<48 hrs) or chronic (>48 hrs)?
At 89 years, assume chronic unless there is clear evidence of acute onset. This completely changes the safe correction rate.
Step 2 - Assess symptom severity
This patient has moderate-severe symptoms (lethargy, vomiting, weakness with Na 123). She does not appear to have seizures or coma, which would demand emergency correction.
Correction Targets (Goldman-Cecil Medicine)
| Risk level | Safe correction goal |
|---|---|
| Moderate/normal ODS risk | Max 10-12 mmol/L in first 24h; max 18 mmol/L in 48h |
| High ODS risk (Na <120, malnutrition, alcoholism, liver disease, hypokalemia) | Max 8 mmol/L in 24h; target 4-6 mmol/L/day |
| Severely symptomatic (seizures/coma) - acute | 3% NaCl 100 mL bolus IV over 10 min; repeat up to 2x |
This 89 year-old patient with Na 123 and chronic hyponatremia is at high ODS risk. Target <8 mmol/L correction in the first 24 hours.
Specific Treatments
A. For SIADH (euvolemic):
- Stop the normal saline - it is likely making things worse
- Fluid restriction to 500 mL/day below 24-hour urine output (e.g., 500-800 mL/day total fluid intake)
- If Na <120 with neurological symptoms: 3% hypertonic saline - cautious infusion at 0.5-2 mL/kg/hour, targeting a 4-6 mmol/L rise in the first few hours to relieve acute cerebral oedema, then slow down
- Treat the underlying cause (stop offending drugs, treat pneumonia/malignancy)
- If fluid restriction fails (urine osmolality >500, urine Na+K > serum Na, urine output <1500 mL/day): consider tolvaptan (oral V2-receptor antagonist, start 15 mg OD, max 60 mg OD) - monitor Na every 6-8 hours; do NOT use with fluid restriction simultaneously
- Oral urea (15-90 g/day in divided doses) is an effective, cheap alternative that increases urinary solute excretion
B. For Adrenal Insufficiency:
- Hydrocortisone 100 mg IV bolus immediately, then 50-100 mg IV every 6-8 hours
- Sodium corrects as adrenal function is restored - do not over-correct separately
C. For Hypothyroidism:
- IV levothyroxine (if severe myxoedema coma: 200-500 mcg loading dose)
- Concurrent hydrocortisone cover until coexisting adrenal insufficiency is excluded
D. For Thiazide-induced:
- Discontinue thiazide immediately
- Correct volume deficit with careful isotonic fluids if hypovolemic (urine Na <20)
- Replace potassium (hypokalemia lowers serum Na and increases ODS risk)
E. For Hypovolemic causes:
- Normal saline is the correct treatment here
- Avoid over-correcting - if ADH drops suddenly when volume is restored, free water diuresis can cause Na to rise too fast
Watch For: Osmotic Demyelination Syndrome (ODS)
ODS (previously called central pontine myelinolysis) is the feared complication of overcorrection. It causes fluctuating consciousness, pseudobulbar palsy, dysarthria, dysphagia, ataxia, and characteristic pontine/extrapontine changes on MRI.
High-risk features in this patient: Na <120 mmol/L, age 89, likely malnutrition, possible underlying liver disease or hypokalemia.
If overcorrection occurs (>12 mmol/L rise in 24h starting from Na <120): re-lower the sodium with hypotonic saline (5% dextrose) or desmopressin (DDAVP 2-4 mcg IV/SC every 8h) to clamp the Na rise while awaiting renal water excretion to slow. - Goldman-Cecil Medicine
Practical ICU/Ward Management
- Stop ondansetron if it is the cause of SIADH (it is a 5-HT3 receptor antagonist and is rarely implicated, but SSRIs/opioids given concurrently are a more common culprit - review the full medication list)
- Admit to a monitored bed or ICU given Na 123 with neurological symptoms
- Foley catheter for accurate hourly urine output measurement
- Monitor serum Na every 4-6 hours until stable and rising appropriately
- Consult nephrology for guidance on hypertonic saline and vaptan use
- Comprehensive metabolic panel including cortisol at 9 AM (or random cortisol if acutely unwell) and TSH
- CT head to exclude CNS pathology causing SIADH or altered consciousness
- CXR +/- CT chest to evaluate for pulmonary causes or occult malignancy
Bottom line: This 89 year-old is presenting with symptomatic moderate-severe hyponatremia that is not responding to normal saline. SIADH is the most likely diagnosis (and normal saline may be worsening it), but adrenal insufficiency and hypothyroidism must be excluded urgently as they are both treatable emergencies. Thiazide diuretics are also a very common culprit in this age group. The cornerstone of management is identifying and treating the underlying cause, fluid restriction for SIADH, and cautious sodium correction not exceeding 8-10 mmol/L in 24 hours to avoid osmotic demyelination.
Sources: Goldman-Cecil Medicine, 26th ed., Ch. 102; Rosen's Emergency Medicine, 9th ed., Ch. 114; Symptom to Diagnosis, 4th ed., Ch. 24; Brenner & Rector's The Kidney; Goodman & Gilman's Pharmacological Basis of Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.