Histologies types of Hodgkin lyphoma from pathology mbbs
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
I now have everything I need for a comprehensive, image-rich answer. Here is the full breakdown:
Histological Types of Hodgkin Lymphoma
Source: Robbins & Cotran Pathologic Basis of Disease + Robbins & Kumar Basic Pathology
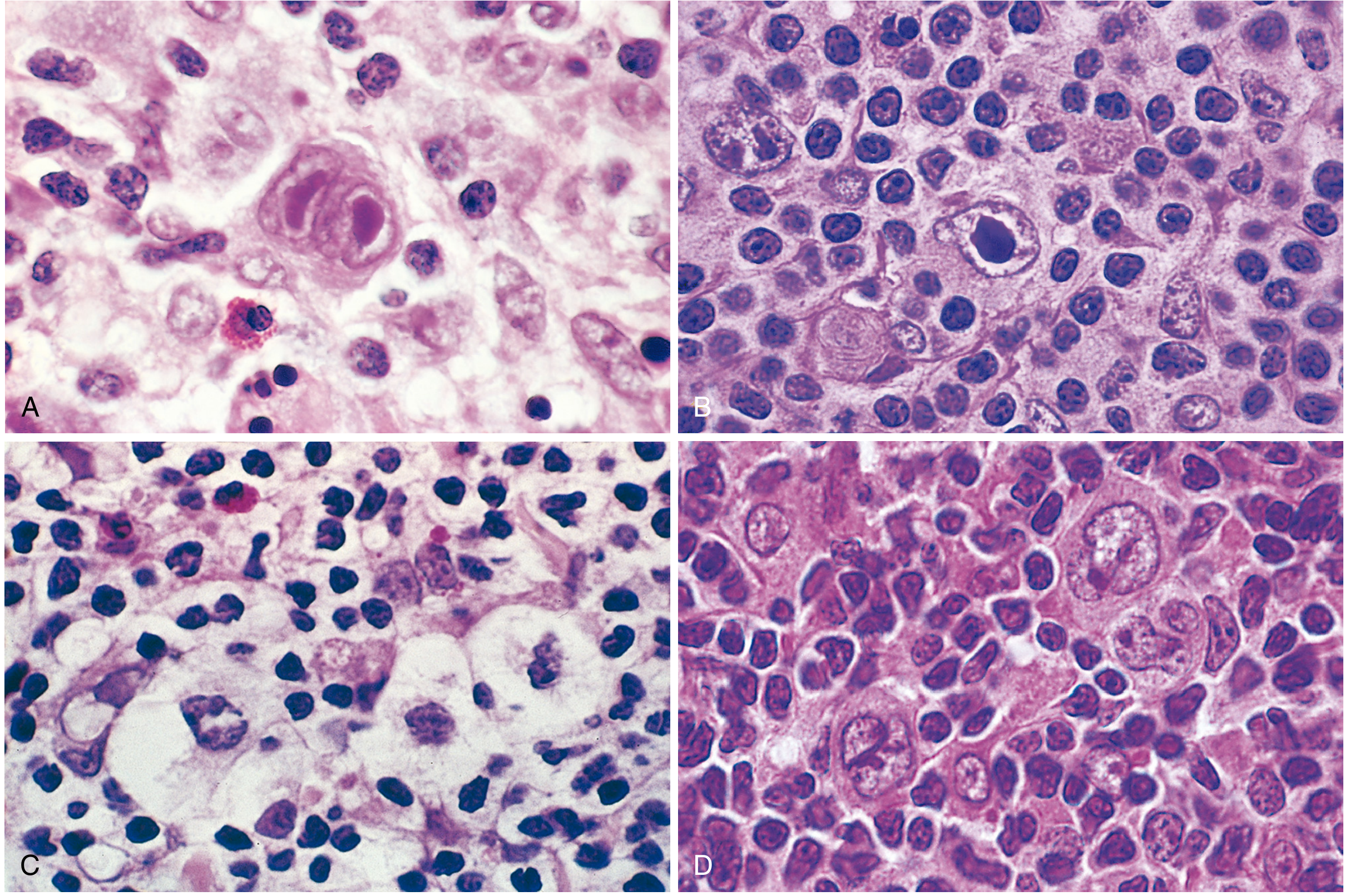
The Reed-Sternberg Cell - The Hallmark
The sine qua non of Hodgkin lymphoma is the Reed-Sternberg (RS) cell - a very large cell (15-45 µm diameter) with an enormous multilobate nucleus, exceptionally prominent nucleoli, and abundant slightly eosinophilic cytoplasm. The classic "owl-eye" appearance comes from two mirror-image nuclei, each with a large acidophilic nucleolus surrounded by a clear halo.
- Origin: Germinal center B cell (proven by clonal IGH gene rearrangements + somatic hypermutation in microdissected RS cells)
- Classic RS cell immunophenotype: CD15+, CD30+, PAX5 (dim)+, CD45-, CD20-, T-cell markers-
Below: RS cells and their variants (A = classic owl-eye, B = mononuclear variant, C = lacunar variant, D = lymphohistiocytic/popcorn variant)
WHO Classification: 5 Subtypes
The first four are grouped as Classic Hodgkin Lymphoma (cHL). The fifth is non-classic.
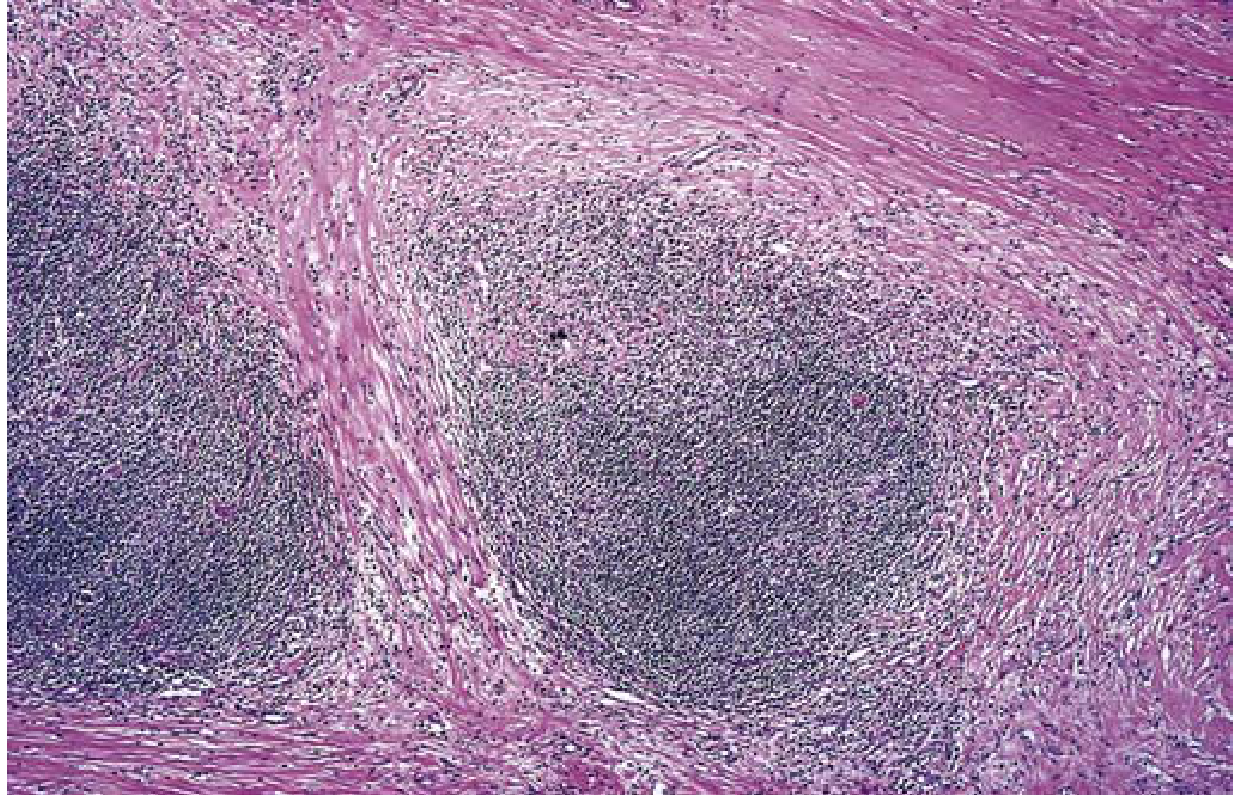
1. Nodular Sclerosis (NS-HL)
Most common - 65-70% of all HL
| Feature | Detail |
|---|---|
| RS cell variant | Lacunar cells - multilobed nucleus, multiple small nucleoli, abundant pale cytoplasm; nucleus retracts in formalin leaving an empty "lacune" |
| Background | T lymphocytes, eosinophils, plasma cells, macrophages |
| Key histology | Collagen bands dividing lymph node into nodules |
| Immunophenotype | CD15+, CD30+, CD45-, EBV usually negative |
| Demographics | Equal M:F, adolescents and young adults |
| Sites | Lower cervical, supraclavicular, mediastinal nodes |
| Stage at presentation | Usually stage I or II |
| Prognosis | Excellent |
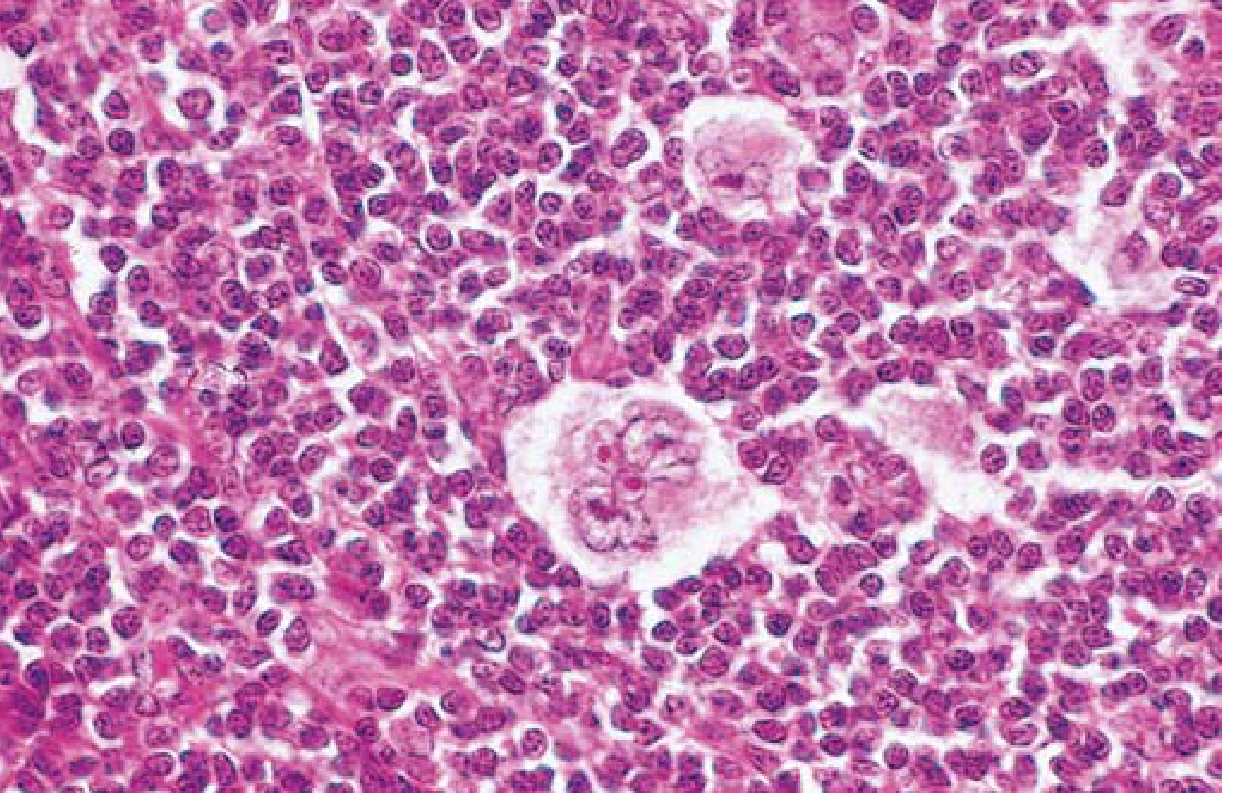
2. Mixed Cellularity (MC-HL)
Second most common - 20-25% of cases
| Feature | Detail |
|---|---|
| RS cell variant | Classic diagnostic RS cells and mononuclear variants - plentiful |
| Background | Heterogeneous mix: T cells, eosinophils, plasma cells, macrophages |
| Key histology | Diffuse effacement of lymph node; no fibrosis |
| Immunophenotype | CD15+, CD30+; EBV+ in ~70% |
| Demographics | Male predominance; most common HL in >50 years; biphasic incidence |
| Stage at presentation | >50% present as stage III or IV |
| Symptoms | More likely to have B symptoms (fever, night sweats, weight loss) |
| Prognosis | Very good overall |
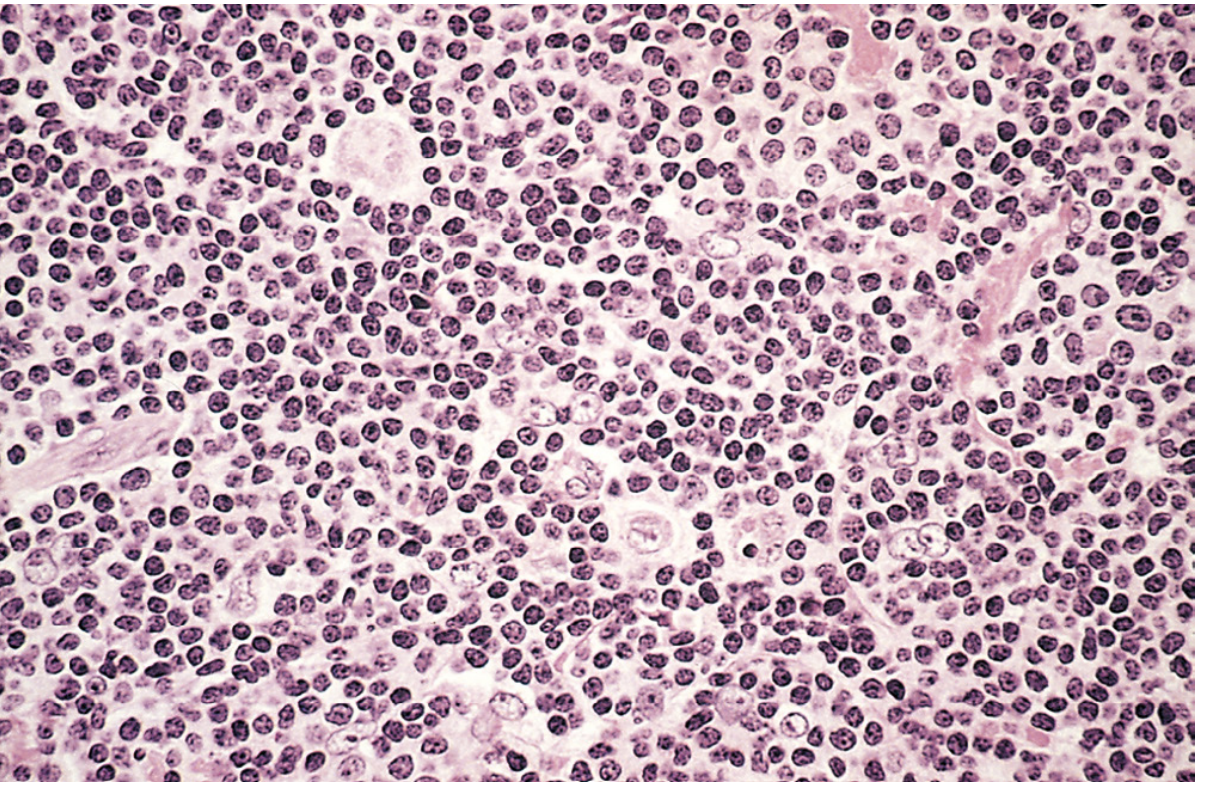
3. Lymphocyte-Rich (LR-HL)
Uncommon classic subtype
| Feature | Detail |
|---|---|
| RS cell variant | Frequent mononuclear and classic diagnostic RS cells |
| Background | Predominantly reactive T lymphocytes; eosinophils/plasma cells scanty |
| Key histology | Diffuse pattern; sometimes vague nodularity from residual B-cell follicles |
| Immunophenotype | CD15+, CD30+; EBV+ in ~40% |
| Demographics | Male predominance; tends to be seen in older adults |
| Prognosis | Very good to excellent |
Distinguished from Nodular Lymphocyte Predominant by the presence of mononuclear/classic RS cells with the "classic" CD15+/CD30+ immunophenotype
4. Lymphocyte-Depleted (LD-HL)
Least common classic subtype - <5% of cases
| Feature | Detail |
|---|---|
| RS cell variant | Abundant RS cells and pleomorphic variants |
| Background | Paucity of lymphocytes (hence the name) |
| Key histology | Reticular variant: sheets of RS cells with few reactive cells |
| Immunophenotype | CD15+, CD30+; EBV+ in >90% |
| Demographics | Older adults, HIV-positive individuals, people in developing countries |
| Stage at presentation | Advanced stage; systemic symptoms frequent |
| Prognosis | Least favorable among HL subtypes |
Key exam point: Most tumors suspected clinically to be LD-HL turn out to be NHL on immunophenotyping - so immunophenotyping is essential for diagnosis.
5. Nodular Lymphocyte Predominant (NLP-HL)
Non-classic - ~5% of cases
| Feature | Detail |
|---|---|
| RS cell variant | L&H (lymphohistiocytic) variants = "Popcorn cells" - multilobed, crumpled, delicate nucleus resembling popped corn |
| Background | Large nodules of reactive small B cells + follicular dendritic cells; eosinophils and plasma cells scanty/absent |
| Key histology | Nodular growth pattern; classic RS cells absent or very rare |
| Immunophenotype | CD20+, BCL6+; CD15-, CD30- (opposite of classic!) |
| EBV | Rarely associated |
| Demographics | Predominantly males <35 years; cervical or axillary lymphadenopathy |
| Special note | In 3-5% of cases, transforms to diffuse large B-cell lymphoma |
| Prognosis | Excellent, but more prone to late relapses |
The ICC (International Consensus Classification) has renamed this entity "Nodular Lymphocyte-Predominant B-cell Lymphoma", dropping the Hodgkin moniker entirely, because the immunophenotype is closer to a B-cell lymphoma than to classic HL.
Quick Comparison Table
| Subtype | Frequency | RS Cell Variant | EBV | CD15 | CD30 | CD20 | Prognosis |
|---|---|---|---|---|---|---|---|
| Nodular Sclerosis | 65-70% | Lacunar cell | Rare | + | + | - | Excellent |
| Mixed Cellularity | 20-25% | Classic RS | ~70% | + | + | - | Very good |
| Lymphocyte-Rich | Uncommon | Classic/mononuclear | ~40% | + | + | - | Excellent |
| Lymphocyte-Depleted | <5% | Pleomorphic/abundant | >90% | + | + | - | Poor (relative) |
| NLP (non-classic) | ~5% | L&H / Popcorn | Rare | - | - | + | Excellent |
Key Pathogenesis Points (Exam Favorites)
- All RS cells originate from germinal center B cells (proven by clonal Ig gene rearrangements)
- In classic HL, RS cells lose all B-cell gene expression due to epigenetic changes
- NF-κB activation is the central survival mechanism in classic HL
- RS cells express PD-L1 and PD-L2 (chromosome 9p amplification) - explains response to anti-PD-1 (pembrolizumab/nivolumab) therapy
- RS cells constitute only a small minority of the tumor mass - most is reactive inflammatory infiltrate
- The reactive cells are recruited by RS cell-secreted cytokines (IL-5 for eosinophils, TGF-β for fibrosis, IL-10 for immune suppression)
Sources: Robbins, Cotran & Kumar - Pathologic Basis of Disease (10th ed.), p. 573-575; Robbins & Kumar Basic Pathology, p. 417-420
This is a shared conversation. Sign in to Orris to start your own chat.